Anterior bone loss after cervical disc replacement: A systematic review
2020-04-07XiaoFeiWangYangMengHaoLiuYingHongBeiYuWang
Xiao-Fei Wang, Yang Meng, Hao Liu, Ying Hong, Bei-Yu Wang
Xiao-Fei Wang, Yang Meng, Hao Liu, Bei-Yu Wang, Department of Orthopaedic Surgery, West China Hospital, Sichuan University, Chengdu 610041, Sichuan Province, China
Ying Hong, Department of Anesthesia and Operation Center/West China School of Nursing,West China Hospital, Sichuan University, Chengdu 610041, Sichuan Province, China
Abstract BACKGROUND Anterior bone loss (ABL) is a relatively easily neglected condition after cervical disc replacement (CDR). Whether this phenomenon is a radiological anomaly or a complication remains controversial. Several studies have reported the clinical characteristics of ABL and speculated on the pathogenic mechanism based on a certain type of artificial disc, while the overall understanding of ABL is lacking.AIM To describe the prevalence, impacts, and risk factors of ABL after CDR.METHODS We searched the PubMed, Cochrane Library, and Excerpta Medica databases using the terms “bone loss” or “bone remodeling” or “bone absorption” or“osteolysis” or “implant loosening” or “implant migration” or “hypersensitivity”or “hyperreactivity”, “cervical disc replacement” or “cervical disc arthroplasty” or“total disc replacement”. Eligible manuscripts on the prevalence and impacts of ABL were reviewed by the authors. Data extraction was performed using an established extraction form. The results of the included studies were described narratively.RESULTS Six studies met the inclusion and exclusion criteria. One was a prospective study and the others were retrospective studies. A total of 440 patients with 536 segments were included. The artificial cervical discs included Bryan, Baguera-C,Discocerv, and Mobi-C. The prevalence of ABL ranged from 3.13% to 91.89%, with a combined overall prevalence of 41.84%. ABL occurred within 6 mo and stopped 12 mo after surgery. Several cases were noted to have a self-healing process.Severe ABL resulted in segmental kyphosis, implant subsidence, and persistent neck pain. ABL may be related to heterotopic ossification. Multilevel surgery may be one of the risk factors for ABL.CONCLUSION ABL is a common condition after CDR. The underlying mechanisms of ABL may include stress concentration and injury to nutrient vessels. ABL should be considered a complication after CDR as it was associated with neck pain, implant subsidence, and heterotopic ossification.
Key Words: Bone loss; Bone remodeling; Stress shielding; Risk factor; Systematic review
INTRODUCTION
Anterior cervical discectomy and fusion (ACDF) is recognized as the standard procedure for cervical degenerative disc disease. However, concerns such as nonunion, pseudarthrosis, and acceleration of adjacent segment degeneration have been raised[1-4]. Compared with ACDF, cervical disc replacement (CDR), a motion preservation technique, can reduce intervertebral disc pressure in adjacent levels and better simulate the physiological condition of the cervical spine[5,6]. Studies have shown that CDR and ACDF have equivalent efficiency in clinical outcomes such as symptom relief[7,8]. However, CDR is better in some respects, such as faster recovery, higher patient satisfaction, and is more cost-effective[9,10].
Although CDR is widely performed and patients have benefited due to its satisfying results, it has some implant-related complications, such as heterotopic ossification(HO), implant migration, and implant subsidence[11-16].With regard to these complications, in-depth studies have been performed to determine the potential risk factors and clinical impacts[17-20]. In contrast to excessive bone formation (which is HO),anterior bone loss (ABL) is another implant-related condition after CDR and has gained more attention in recent years[21]. ABL is the process of bone rebuilding in the ventral part of vertebral bodies, and can usually be recognized from lateral radiographs. Peri-prosthetic bone loss has been extensively described in large joint arthroplasty. However, ABL is easily ignored in cervical disc arthroplasty.
The prevalence of ABL after CDR varies from 3.13% to 91.89% and differs greatly among different types of artificial cervical discs[22-27]. Several studies have reported the clinical characteristics of ABL and speculated the pathogenic mechanism based on a certain type of artificial disc, while the overall understanding of ABL after CDR is lacking. In addition, it remains controversial whether ABL is a radiological anomaly or a complication. Therefore, we performed this systematic review of currently available clinical data to comprehensively describe the prevalence, impacts, and risk factors of ABL after CDR.
MATERIALS AND METHODS
A comprehensive literature search was carried out in PubMed, Cochrane Library, and the Excerpta Medica databases. Studies before May 2019 were included. The following keywords were used in the search: “bone loss” or “bone remodeling” or “bone absorption” or “osteolysis” or “implant loosening” or “implant migration” or“hypersensitivity” or “hyperreactivity”, “cervical disc replacement” or “cervical disc arthroplasty” or “total disc replacement”. Articles published in English that involved peri-prosthetic bone absorption after CDR were specifically identified. The references of all identified papers were manually reviewed to identify further potentially relevant studies.
The search produced 1460 published articles. We then systematically assessed the selected articles. The inclusion criteria were as follows: (1) peri-prosthetic bone loss occurred in the surgical segment after CDR; and (2) bone remodeling occurred in the anterior/ventral part of vertebral bodies. The exclusion criteria were as follows: (1)Peri-prosthetic bone loss occurred in another part of the vertebral bodies, (2) Case reports, (3) Reviews, (4) Commentaries, and (5) Cadaveric or experimental studies. The results of the literature search are shown in Figure 1.
The screening of titles and abstracts was performed by two reviewers (Wang XF and Meng Y) independently. Articles that met the eligibility criteria on the first screening were further assessed by reading the full text. After screening, six clinical studies were included in the systematic review. The two reviewers (Wang XF and Meng Y) then performed data extraction and rated the level of evidence of each article independently using the published guideline[28]. The results of this study were described narratively.
RESULTS
One randomized controlled study and five retrospective studies were included in this review[22-27]. A total of 440 patients with 536 segments were included. The mean age of these patients ranged from 45.3 to 50.1 years, and the mean follow-up time ranged from 32.3 to 74.4 mo. The artificial cervical discs included Bryan, Baguera-C,Discocerv, and Mobi-C. The surgical procedure included single-level CDR, doublelevel CDR, triple-level CDR, and hybrid surgery. Study information and level of evidence are listed in Table 1. Detailed information on ABL including the prevalence,course, effects, and outcomes are summarized in Tables 2-4 and Figure 2.
Overview of ABL after cervical disc arthroplasty
ABL was identified on lateral X-rays in all six studies, and had the following two signs:first, the ventral-inferior part of the cranial vertebra or the ventral-superior part of the caudal vertebra at the arthroplasty level disappeared; second, the cortical bone margin of the ABL area still existed and shifted dorsally.
The prevalence of ABL ranged from 3.13% to 91.89%, with a combined overall prevalence of 41.84%, and it differed depending on the implant type. The Mobi-C showed the highest prevalence of ABL (91.89%), followed by the Baguera-C (60.42%-64.29%, 62.50% after combination), Discocerv (47.73%) and Bryan (3.13%-57.14%,22.16% after combination). In the study by Kieseret al[26], the cranial vertebra showed a higher ABL rate.
ABL occurred within 3-6 mo postoperatively and did not progress after 12 mo postoperatively in most cases. Kieseret al[26,27]reported a “self-healing phenomenon” of ABL in several cases, but they did not present other radiological evidence to prove that the self-healing was not caused by HO. In the study by Hacker, one patient with ABL received revision fusion surgery to relieve symptoms[23].
The grading system of ABL
Three studies reported the grading system of ABL based on the lateral radiographs(Table 2). Heoet al[25]divided the ABL into three grades: Grade 1 refers to a small part of the vertebra with ABL; Grade 2 indicates a larger portion of the vertebra with ABL compared with Grade 1, but the implant was not exposed; Grade 3 refers to significant bone loss with exposure of the implant. This non-quantitative grading method is ambiguous when classifying Grade 1 and 2 ABL. The authors then assigned Grade 1 and 2 ABL into the minor change Group (without exposure of implants), and assigned Grade 3 into the major change group (with implant exposure). The prevalence of ABL was 43.75% in the minor change group and 16.67% in the major change group. This grading system is not suitable for artificial discs with an anterior flange such as Bryan,because a small portion of ABL would cause implant exposure. Besides, an obvious ABL may be assigned to the minor change group due to the posteriorly positioned implant.
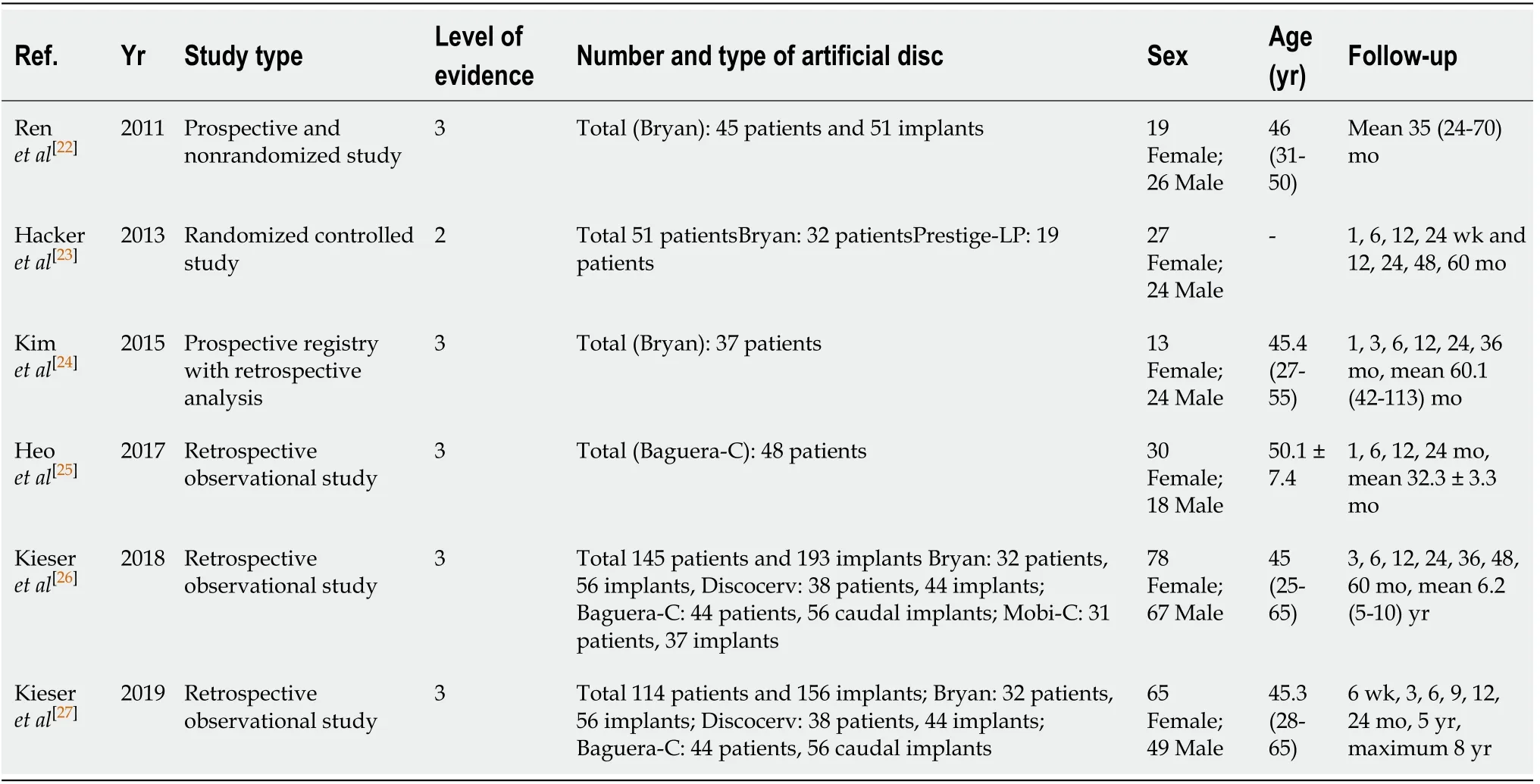
Table 1 Studies included in the systematic review
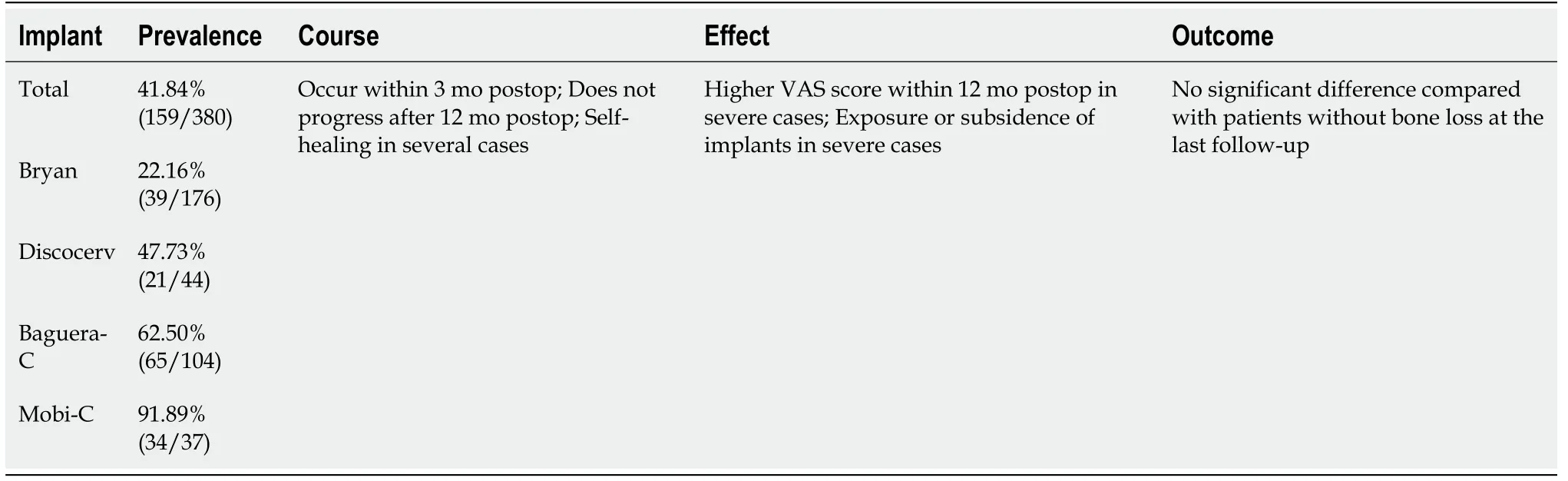
Table 2 Summary of the combined data of anterior bone loss in cervical disc replacement
Kieseret al[26]introduced a quantitative grading method based on the lateral radiographs. They calculated the ratio of the bone loss distance and the initial length of the endplate and then divided the ABL into three groups: mild (ratio ≤ 5%), moderate(5% < ratio ≤ 10%), and severe (ratio > 10%). The prevalence of ABL was 48.7% in the mild group, 11.92% in the moderate group, and 3.11% in the severe group,respectively. Severe ABL caused implant exposure or subsidence.
In 2019, Kieseret al[27]slightly revised their grading system. They divided severe ABL into two subgroups: severe with endplate collapse (four patients), and severe without endplate collapse (one patient, who showed a self-healing process). However,in their grading system, there was no significant difference among the groups in terms of radiological or clinical outcomes. Therefore, this grading system is not instructive in clinical work.
Outcomes of ABL
All patients with ABL achieved similar clinical outcomes at the last follow-up,compared with those who did not develop ABL. In the study by Renet al[22], three patients had ABL, and they did not complain of any subjective discomfort. Two patients had ABL < 2 mm and Grade 2 HO was observed in one of them; one patienthad ABL > 2 mm, and grade 4 HO was noted in this patient. It is noteworthy that the authors only observed HO in three patients in this study.
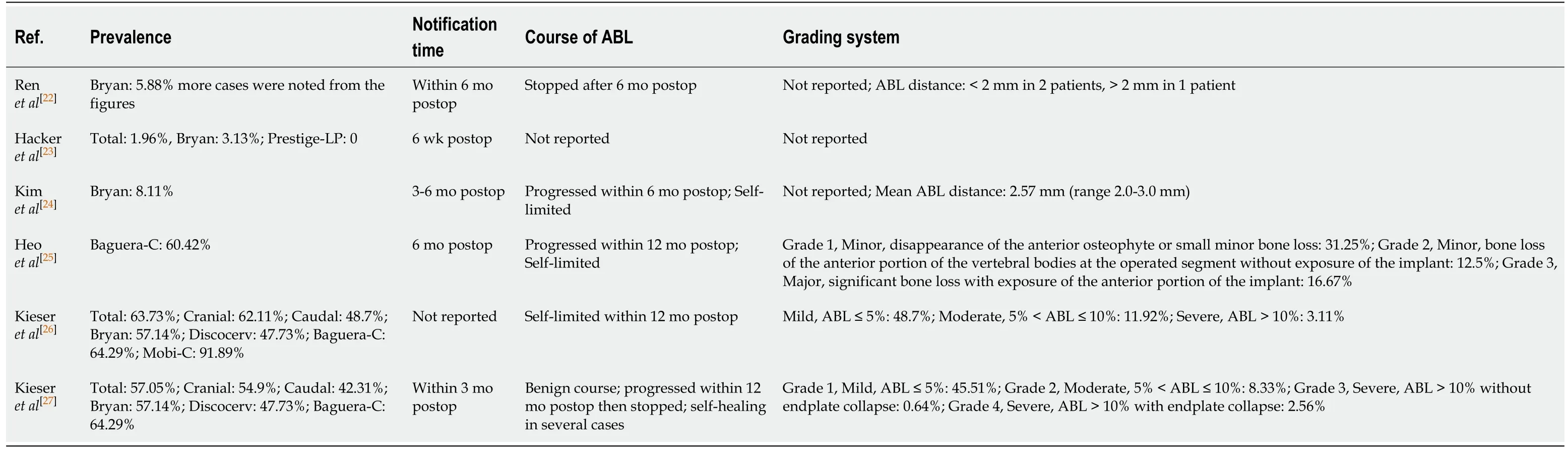
Table 3 Summarized data of incidence and identification of anterior bone loss
Hackeret al[23]reported one patient with ABL who suffered from recurrent neck and arm pain after surgery for 52 mo. The shell angle was kyphosis at the last follow-up, as well as the functional spine unit angle. This patient received revision surgery, in which the Bryan disc was removed and two-level anterior cervical fusion was performed.
Kimet al[24]described the outcomes of ABL in three patients. The average distance of ABL was 2.57 mm (range 2.0-3.0 mm). These three patients achieved satisfying clinical outcomes without any change in symptoms during follow-up, and their pre- and postoperative read only memory were in the average range of this study. Ossification of the anterior longitudinal ligament (ALL) at the inferior adjacent level was noted in one patient at the two-year follow-up.
Heoet al[25]addressed the clinical effects of ABL. In their research, patients in the major change group (implant exposure) suffered from obvious neck pain postoperatively. The visual analogue scores for neck pain at 6 mo and 12 mo after surgery were 5.3 ± 2.0 and 4.7 ± 1.7, respectively, in the major change group; and 1.8 ±1.1 and 1.8 ± 0.9, respectively, in the minor change group. Statistical differences were found between the two groups. The motion function was preserved at the last followup in the patients with ABL.
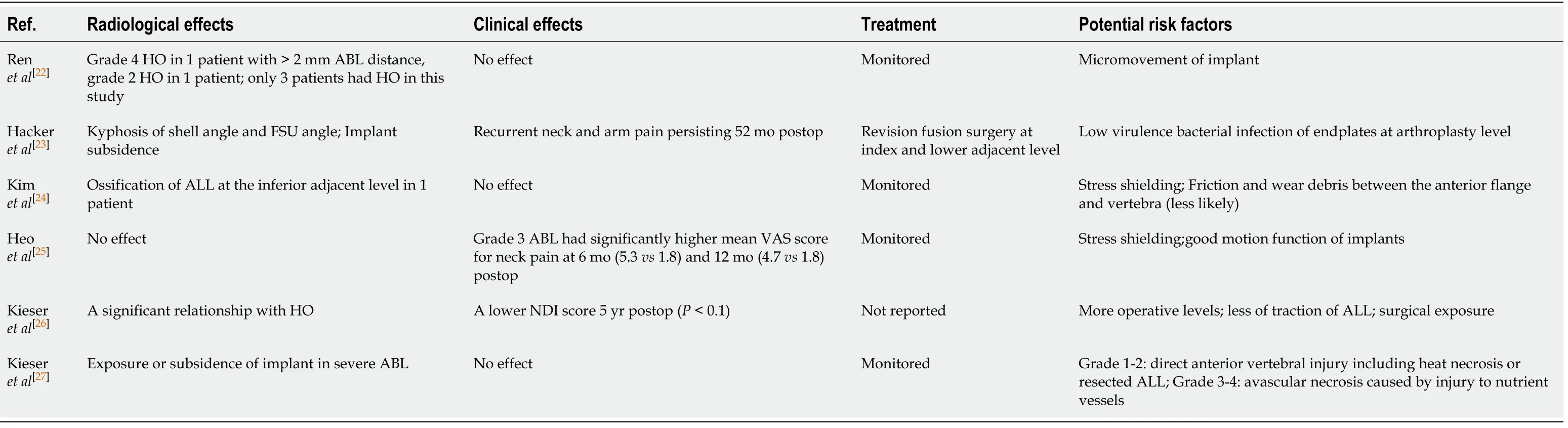
Table 4 Effects, outcomes, and risk factors of anterior bone loss
Kieseret al[26,27]reported that ABL caused no statistical difference in visual analogue score for arm or neck pain at any time after surgery, although the neck disability index score showed a decreasing trend at the last follow-up in patients with ABL (18.9 in the non-ABL group, 11.2 in the mild group, 10.1 in the moderate group, and 9.0 in the severe group,P= 0.094). Implant exposure or subsidence was observed in patients with severe ABL. Additionally, a significant relationship between Grade 4 HO and ABL was found in their research.
Potential risk factors and mechanism of ABL
Kieseret al[26,27]analyzed the potential risk factors for ABL. In their retrospective studies with a minimum follow-up of five years, they found that the number of levels operated was the only risk factor. Other variables including age, sex, cervical alignment, read only memory, and implant position were not related to ABL. They hypothesized that the extensive exposure and drilling of vertebra might cause a direct osteolytic insult, and the more the dissection and soft-tissue stripping during multilevel surgery, the greater the bone insult. In addition, Kieser found that the cranial endplate was exposed to a greater risk of ABL, which could be due to resection of the ALL. The ALL attaches tightly to the inferior portion of the ventral surface of the cervical vertebrae, and this region would be non-loaded and subsequently resorbed after resection of the ALL.
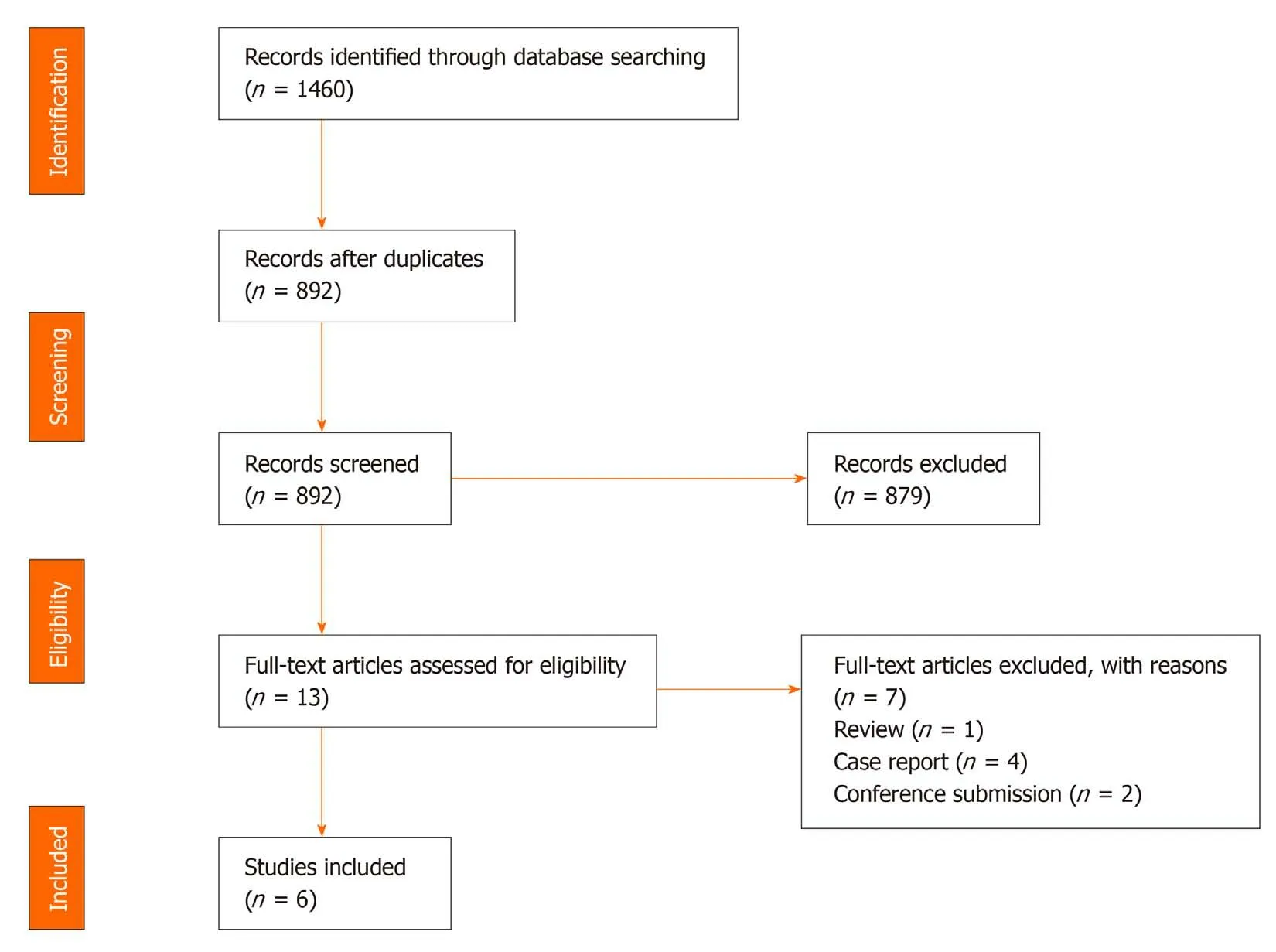
Figure 1 Preferred reporting items for systematic reviews. Preferred reporting items for systematic reviews flow diagram for selection of studies based on inclusion criteria during systematic review.
In 2019, Kieseret al[27]proposed the mechanism of ABL of different degrees. The direct heat necrosis of the vertebra and resection of the ALL may cause Grade 1-2 ABL.Injury to nutrient vessels of the vertebra and subsequent avascular necrosis may lead to grade 3-4 ABL.
Heoet al[25]considered that the stress shielding effects played an important role in ABL. They observed a complete cortical bone margin of the ABL area based on computed tomography scans, and did not find any radiolucent osteolytic lesion adjacent to the implants. This opinion was consistent with that of Kimet al[24].
Kimet al[24]also speculated that the wear debris of artificial discs might induce the inflammatory response, and the inflammatory factors would recruit pre-osteoclasts and initiate the bone remodeling process.
Hackeret al[23]believed that low virulence bacterial infection of the endplate may account for the ABL in their case. They evaluated the tissue samples around the implant and did not find any pathological agent or culture except for macrophages.
In contrast, Renet al[22]thought that ABL did not look like a low-grade infection.They hypothesized that micromovement would cause mechanical damage to the adjacent vertebra and subsequent bone loss.
DISCUSSION
Peri-implant bone loss has been widely reported in large joint arthroplasty[29-31].However, studies on bone loss after CDR are lacking. By reviewing the literature, we classified the mechanism of ABL into three major hypotheses: stress shielding,micromovement, and injury to nutrient vessels.
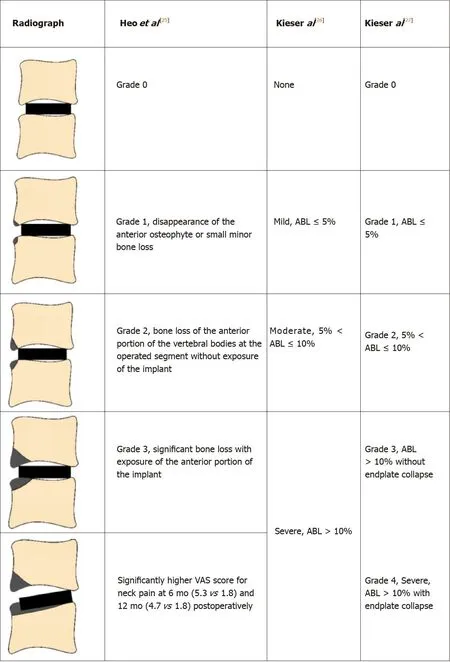
Figure 2 Summarized grading systems of the included studies. ABL: Anterior bone loss, colored in gray; VAS: Visual analogue score; NDI: Neck disability index.
The stress shielding effect has been documented as one of the factors of bone loss in hip and knee replacement[29]. In CDR, this term may be more accurately named as stress concentration. Physiologically, the axial loads transfer evenly and gently from one vertebra to the intervertebral disc, then to another vertebra. However, this mechanical system is altered after disc arthroplasty; the axial loads would transfer through the implant. Therefore, the stress would concentrate on where the implant is located. On the one hand, some artificial discs show obvious stress concentration in the anterior part of the endplates[32,33]. The hyper-pressure in the anterior region can activate the process of bone resorption[34]. On the other hand, the artificial disc does not cover the endplate sufficiently[35,36]. For the non-keel designed artificial disc, for instance, Discocerv and Baguera-C, the anterior part of the endplates cannot be covered, which may lead to hypo-pressure in this region. Based on Wolff’s law, the anterior vertebral hypo-pressure from the artificial disc would initiate bone resorption.Consistent with this hypothesis, previous finite element studies showed that stress was distributed in the covered area of the endplates at the surgical level[37,38]. In addition, Wanget al[21]noted that patients with ABL showed a significantly more lordotic disc angle (which may shift the axial load posteriorly), compared with those who developed anterior HO. Accordingly, stress concentration may be one major reason for the development of ABL.
Micromovement of the implant into the vertebra may induce mechanical damage to the peri-implant bone and subsequent bone loss[22,23]. On the other hand, micromotion may cause artificial discs to produce friction and wear debris, which may induce an inflammatory response and peri-implant bone loss[29,39,40]. Basic studies have proved that the wear debris can initiate bone lossviathe RANK/RANKL/OPG pathway, and the inhibition of inflammation or RANK/RANKL pathway has protective effects on peri-implant osteolysis[41-43]. In addition, debris can also induce innervation and pain factor production[42].
Although wear debris-induced osteolysis is widely accepted in large joint arthroplasty, this hypothesis is flawed with regard to two aspects in CDR. First, bone loss caused by wear debris is not confined to the anterior portion of the vertebra, but is around the surface of the implant. For instance, Devinet al[44]reported wear debrisinduced bone loss after lumbar disc replacement. Massive osteolysis was noted in the central and posterior region of the vertebral body, and debris was scattered in the adjacent bones. Veruvaet al[45]described the presence of osteolytic cysts distributed around artificial lumbar discs caused by the debris. These findings suggest that wear debris-induced bone loss is different to ABL in phenotype. Second, ABL was observed within 3 mo in most cases, and had a self-limited course. In contrast, debris-induced osteolysis may be evident on radiographs after a longer time and may be progressive,which was reported by Tumialánet al[46]. They described bone loss which was noted 9 mo after Prodisc-C implantation. The osteolytic process did not stop until the implant was removed. To sum up, wear debris is not a likely cause of ABL.
The third major hypothesis of ABL is the injury to nutrient vessels of the anterior vertebrae. The anatomic study by Dunbaret al[47]demonstrated the abundant nutrient blood supply in the anterior part of the cervical spine[48]. These vessels pass over the longus colli, and penetrate vertebrae mainly on the anterior surface of the cervical vertebrae. Usually, these nutrient vessels are coagulated to reduce intraoperative bleeding, and this may cause avascular necrosis of the anterior part of the endplate.The anterior nutrient foraminae are mainly located in the superior third of the vertebrae, leaving the inferior portion hypo-vascular. Therefore, theoretically, the inferior portion of vertebrae would be at a higher risk of avascular necrosis, and this is consistent with the clinical findings of Kieseret al[27]. Consequently, ABL may be related to avascular necrosis caused by injury to nutrient vessels.
Kieseret al[26]showed that the more levels operated, the higher the risk of developing ABL. A possible explanation for this might be that multilevel surgery would change the biomechanical properties of the cervical spine leading to hyper- or hypo-pressure in the anterior region of the vertebrae, as described earlier.Additionally, we believe the design of artificial discs is another risk factor in the development of ABL. The prevalence of ABL was different among artificial discs, and this could be attributed to the discrepancy in stress distribution of the endplates of different types of artificial discs.
Some authors consider that heat necrosis due to the burring and milling process could inactivate osteocytes of the anterior vertebra, and result in a direct osteolytic insult. However, the findings of Heoet al[25]and Kieseret al[26,27]do not support this assumption. Even though the anterior cortex of the vertebra was carefully preserved during surgery, ABL still occurred. In addition, Wanget al[21]found that the anterior milling ratio and milling angle were comparable between patients with ABL or anterior bone formation. Therefore, heat necrosis may not be the most important risk factor for ABL.
Usually, patients with ABL do not have clear clinical and radiological effects, while severe ABL may produce segmental kyphosis and local pain[23-25]. Due to the selflimited process, most cases do not require intervention. However, we hold the view that early interventions including rehabilitation exercise and pain relief are necessary for these patients. In our center, we have seen patients with ABL complain of persistent neck pain for one year after surgery. Early interventions can improve the satisfaction of surgery and quality of life. In addition, the impacts of ABL on the adjacent segments remain unknown. Further studies with long-term follow-up are needed to clarify the relationship between ABL and adjacent segment degeneration.
Currently, ABL is observed on lateral radiographs. Notwithstanding this method is simple and easy, but it may increase the false positive rate of ABL. Occasionally, the inappropriate irradiation direction of X-rays may give us a false impression that ABL has occurred. For this reason, computed tomography scans are better in evaluating the prevalence of ABL[25]. Moreover, to prevent and identify ABL early, further studies on the mechanism and risk factors of ABL after CDR are needed.
There are several limitations in our study. The major limitation is the small sample size of each included study. Studies with large sample size are needed to determine the precise prevalence of ABL. As diverse evaluation systems for ABL were used in the included studies, it is difficult to make accurate assessments on the impacts of ABL. In addition, most studies only used non-keeled artificial discs; thus, ABL in keeled artificial discs, such as Prodisc-C and Prestige-LP, is unknown. Finally, we focused on prospective and retrospective studies, and may have missed a wider discussion on the underlying mechanism of ABL in some case reports or case series.Further studies are required to elucidate these limitations.
CONCLUSION
ABL is common in CDR. ABL occurs within 3-6 mo, and stops 12 mo after surgery.Several cases were noted to have a self-healing process. ABL does not have obvious clinical or radiological effects in most patients, while severe ABL may result in segmental kyphosis and persistent pain. ABL may be related to HO; however further studies are required to confirm this. Multilevel surgery is recognized as a potential risk factor for ABL, and the underlying mechanisms include stress concentration and injury to nutrient vessels. ABL should be considered a complication after CDR as it was associated with neck pain, implant subsidence, and HO.
ARTICLE HIGHLIGHTS
Research background
Anterior bone loss (ABL) after cervical disc replacement (CDR) has attracted considerable concern in recent years. Whether ABL is a radiological anomaly or a complication remains unknown.
Research motivation
Several studies have reported the prevalence, impacts, and outcomes of ABL.However, an overall understanding of ABL is lacking.
Research objectives
This study aimed to comprehensively evaluate ABL after CDR.
Research methods
A systematic review was performed according to the preferred reporting items for systematic reviews guideline.
Research results
The prevalence of ABL ranges from 3.13% to 91.89%, and multilevel surgery may be one of the risk factors for ABL. ABL occurred within 6 mo postoperatively and stopped after 1 year. Severe cases may result in kyphosis, implant subsidence, and neck pain.
Research conclusions
ABL is a common condition after CDR. ABL should be considered a complication after CDR due to its clinical impacts.
Research perspectives
Further studies should clarify the relationship between ABL and adjacent segment degeneration. Further studies on the mechanism and risk factors for ABL are needed.The method used to measure ABL should be improved.
ACKNOWLEDGEMENTS
We wish to thank Dr. Ying-Jun Guo and Dr. Jun-Bo He for advice on the discussion.
杂志排行

World Journal of Clinical Cases的其它文章
- Strategies and challenges in the treatment of chronic venous leg ulcers
- Peripheral nerve tumors of the hand: Clinical features, diagnosis,and treatment
- Treatment strategies for gastric cancer during the COVID-19 pandemic
- Oncological impact of different distal ureter managements during radical nephroureterectomy for primary upper urinary tract urothelial carcinoma
- Clinical characteristics and survival of patients with normal-sized ovarian carcinoma syndrome: Retrospective analysis of a single institution 10-year experiment
- Assessment of load-sharing thoracolumbar injury: A modified scoring system