Abnormal liver function tests associated with severe rhabdomyolysis
2020-03-23AndyKHLim
Andy KH Lim
Abstract Rhabdomyolysis is a syndrome of skeletal muscle injury with release of cellular constituents such as potassium, phosphate, urate and intracellular proteins such as myoglobin into the circulation, which may cause complications including acute kidney injury, electrolyte disturbance and cardiac instability. Abnormal liver function tests are frequently observed in cases of severe rhabdomyolysis.Typically, there is an increase in serum aminotransferases, namely aspartate aminotransferase and alanine aminotransferase. This raises the question of liver injury and often triggers a pathway of investigation which may lead to a liver biopsy. However, muscle can also be a source of the increased aminotransferase activity. This review discusses the dilemma of finding abnormal liver function tests in the setting of muscle injury and the potential implications of such an association. It delves into some of the clinical and experimental evidence for correlating muscle injury to raised aminotransferases, and discusses pathophysiological mechanisms such as oxidative stress which may cause actual liver injury. Serum aminotransferases lack tissue specificity to allow clinicians to distinguish primary liver injury from muscle injury. This review also explores potential approaches to improve the accuracy of our diagnostic tools, so that excessive or unnecessary liver investigations can be avoided.
Key words: Rhabdomyolysis; Muscle; Creatine kinase; Liver function tests; Alanine aminotransferase; Aspartate aminotransferase; Aminotransferases
INTRODUCTION
Rhabdomyolysis is defined as muscle injury which is significant enough to result in release of potentially toxic cellular contents into the circulation. These cellular contents include metabolites such as potassium, phosphate and urate, enzymes such as creatine kinase (CK) and lactate dehydrogenase (LDH), and intracellular proteins such as myoglobin[1]. Serum CK is used to diagnose rhabdomyolysis and most studies use a cut-off of five times the upper limit of normal, or equivalent to 1000 U/L[1].Symptoms of rhabdomyolysis are typically myalgias, weakness and dark urine due to myoglobinuria. Severe cases may result in compartment syndrome, electrolyte disturbance which may cause arrhythmia or cardiac instability, acute kidney injury(AKI) and disseminated intravascular coagulation[1-4]. Rhabdomyolysis was first recognised in war injuries and crush syndrome but many causes are now appreciated.The discussion of causes and treatment are beyond the scope of this review and are covered elsewhere[1-4]. The main aim of this review is to discuss the association between rhabdomyolysis and abnormal liver function tests.
ABNORMAL LIVER FUNCTION IN RHABDOMYOLYSIS
The usual liver panel tests include bilirubin, alkaline phosphatase (ALP), aspartate aminotransferase (AST), alanine aminotransferase (ALT) and γ-glutamyl transferase(GGT). The aminotransferases (AST and ALT) are involved in liver gluconeogenesis and are good biomarkers for liver cell injury. AST is present in cytosolic and mitochondrial isoenzymes and is found in the liver, cardiac muscle, skeletal muscle,kidneys, brain, pancreas, lungs, leucocytes, and red cells. It is less sensitive and specific for the liver. On the other hand, ALT is a cytosolic enzyme which is more specific to the liver due to the high concentration in liver tissue. ALT is also found in skeletal muscle but in much lower concentrations[5].
Abnormal liver function tests are frequently observed in patients with severe rhabdomyolysis but compared to electrolyte derangements, this is a much less appreciated phenomenon that is still shrouded in uncertainty. An example of such a case is shown in Figure 1.
The quandary facing the clinician is determining the source of the elevated aminotransaminases in rhabdomyolysis, as the difference in aminotransferases between liver and muscle is quantitative rather than qualitative. At the first instance,the other liver markers may be useful for differentiating a muscle or liver source of AST or ALT[6]. GGT is not found in muscle and would suggest liver injury if elevated.Similarly, elevation in bilirubin would not be expected in isolated muscle injury. The association between serum CK and liver biochemistry is demonstrated in Figure 2.The uncertainty arises in patients with elevated CK and isolated increase in aminotransferases. Is it liver, muscle or both?
POTENTIAL IMPLICATIONS
Why is the association between rhabdomyolysis and abnormal liver function tests important to recognise? Abnormalities of liver function tests are relatively common and liver injury is frequently associated with many commonly used medications. On the other hand, rhabdomyolysis is uncommon, and symptoms may be relatively mild.

Figure 1 Case example of elevated alanine aminotransferase level in a 25 year old male admitted to hospital with exertional rhabdomyolysis managed with intravenous normal saline for 48 h, showing the typicalconcurrent rise and fall of serum creatine kinase and alanine aminotransferase levels.
Unnecessary testing or missed diagnosis
When there is no history of muscle disease or injury, clinicians may erroneously attribute elevated aminotransferases to liver injury. Even with known rhabdomyolysis, additional tests for liver disease (biochemistry, serology and molecular) have mostly been negative, and 30%-50% of hepatobiliary imaging(sonography and computed tomography) were normal with most abnormalities consistent with hepatic steatosis[6]. Consequently, this may result in unnecessary liver tests, including invasive tests such as a liver biopsy, which mostly reveals no abnormalities[7]. As a corollary of over-investigating for liver disease, there could be a failure to recognise and investigate muscle disease. For example, a 27-year old man endured seven years of investigations for abnormal aminotransferases and had two liver biopsies, before the identification of an elevated CK led to a final diagnosis of muscular dystrophy[8].
Implications for clinical trials and critical medicines
The finding of abnormal liver function tests is of significant concern in clinical trials of investigational products and may potentially see novel drug development falter. For example, in vaccine trials, vigorous physical activity have been known to confound results and interpretation of liver function tests, where increased CK and aminotransferases were noted[9,10]. Recognising the association could also prevent unnecessary avoidance of useful or critical treatments which are potentially hepatotoxic[11].
Association with mortality
There are studies suggesting that abnormal liver function tests in patients with muscle injury is associated with higher mortality in some clinical contexts. In critically ill patients with rhabdomyolysis, patients who had a AST or ALT over 1000 U/L had a higher mortality than those with levels below 1000 U/L (61%vs15%)[12]. In another rhabdomyolysis study, a higher CK/ALT ratio was associated with lower mortality,even after adjusting for age, AKI and sepsis[6]. In the general population, abnormal liver function is associated with increased all-cause mortality. Where ALT is concerned, there is geographical variation and Asian populations seem to have a higher risk than North American populations[13]. The reason for the association with mortality is not clear and should be investigated.
EVIDENCE FOR MUSCLE DERIVED ALT IN RHABDOMYOLYSIS
Is there data to demonstrate that muscle is the source of elevated aminotransferases?If we subscribe to this theory, a few basic facts need to be demonstrated. Firstly,aminotransferases can be localised to muscle at a cellular level. Secondly, we can increase serum aminotransferases by inducing muscle injury. Thirdly, we can show that the elevated aminotransferases normalise with resolution of muscle injury.Ideally, we should be able to demonstrate that no other evidence of liver injury exists.
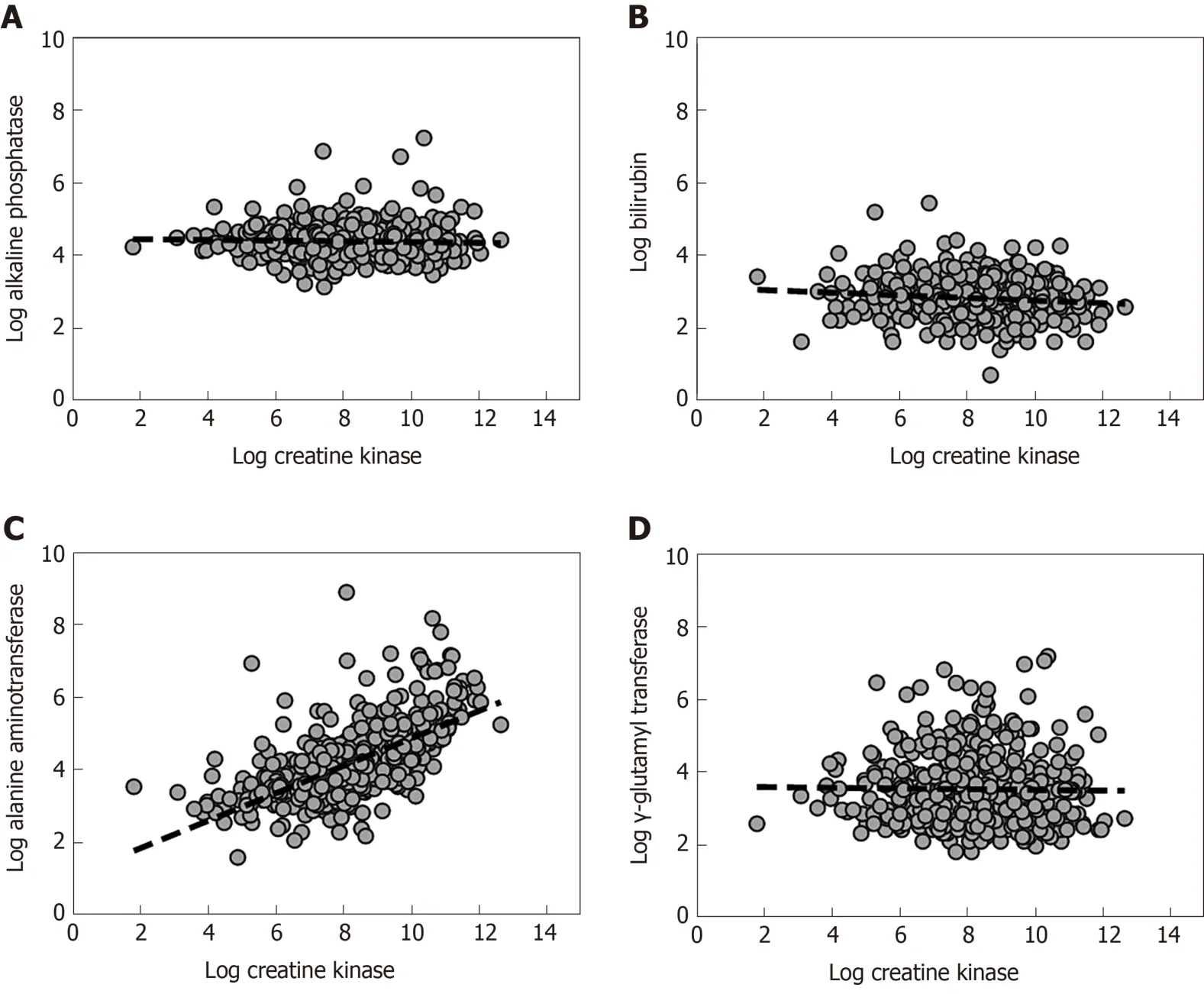
Figure 2 The association between serum creatine kinase and liver biochemistry. Cross-sectional data (n = 528) show a clear association between serumcreatine kinase level as a marker of rhabdomyolysis and the serum alanine aminotransferase levels (C), but there is no correlation between serum creatine kinase and alkaline phosphatase (A), bilirubin (B) or γ-glutamyl transferase (D) (Figure adapted from Lim et al[6]).
Cellular localisation
In diverse animal species, ALT, AST and LDH can be found in multiple tissues,including kidney, liver and muscle[14,15]. Yanget al[16]used molecular methods to quantify the distribution of ALT1 and ALT2 mRNA in rats, and showed that ALT1 is mainly expressed (from high to low) in the intestines, liver, fat, colon, muscle and heart. ALT2 mRNA is more limited in distribution, to liver, muscle, brain and white adipose tissue. ALT1 is mostly intracytoplasmic while the more abundant ALT2 is localised to mitochondria. In humans, ALT is more specific for the liver than AST but it is known to exist in red blood cells, kidney, brain, heart and skeletal muscle[17].However, there is paucity of data on the quantitative differences between tissues.Wroblewski[17]reported that ALT was 10 times more abundant in the liver than muscle. Apple and Rogers suggested that the ratio of the amount of ALT between an equivalent weight of muscle and liver was 1:4[18]. The differences between studies may reflect the method of measurement, and a more detailed analysis may be more revealing.
Clinical studies of muscle injury
There are a few human studies which provided proof of concept for the association between muscle injury and elevated aminotransferases. Petterssonet al[19]subjected 15 fit young men aged 18-45 years to a one-hour weightlifting session. They demonstrated that AST, ALT, LDH, CK and myoglobin were significantly increased after the activity, and it took at least 7 d to normalise, while the bilirubin, ALP and GGT remained normal. In a study by Palet al[20], 44 post-pubertal boys and girls underwent intensive treadmill exercise. They also demonstrated that serum ALT and AST increased significantly at 24 and 48 h in association with a raised CK and LDH.The effects were more pronounce in boys compared to girls. These prospective clinical studies provide better evidence than case reports because they were performed in otherwise healthy individuals with normal baseline biochemistry. There is also less risk of confounding by concurrent illness and medication use.
In a histological study, Apple and Rogers examined the serum and muscle activity of ALT in 30 marathon runners for acute changes. The investigators performed gastrocnemius muscle biopsies at 9 wk and 48 h prior to the marathon, and at 24 h after. They showed that serum ALT was significantly elevated at 24 h after the race compared to pre-race levels. ALT levels remained elevated at 96 h. The investigators noted that the muscle content of ALT did not significantly increase after the race and believed that the elevated serum ALT was more likely due to hepatic release[18]. It is difficult to support the conclusion of Apple and Rogers. They also showed that the ALT activity per wet tissue weight of muscle was around 20% that of the liver (12 U/gvs50 U/g). The fallacy in their argument lies in the fact that absolute skeletal muscle mass far exceeds liver mass, being estimated at 21 kg in women and 33 kg in men, on average[21]. Trivial changes in one gram of muscle tissue may be significant when amplified 20000 times.
Pattern and trajectory of CK and aminotransferases
As shown in our case example, the temporal changes in CK and ALT is fairly typical in observational data of rhabdomyolysis as well as in human experimental data[19,22]. A significant rise in CK is usually detectable within 24 h after the inciting injury, peaks around 72 h, and declines over a period of 7 to 12 d. A significant rise in AST is usually detectable at 24 h when ALT may still be in the normal range until 48 h. The AST tends to peak around 3 to 4 d and the ALT peaks later at 4 to 5 d post injury. The AST tends to be higher than ALT such that the AST/ALT ratio is usually greater than one. In the case report of exertional rhabdomyolysis, the average AST/ALT ratio in the first seven days of admission was 3.0 (range, 1.24 to 4.72)[22]. The peak AST/ALT tends to occur at the same time as peak AST, on day 3 from onset of injury[19]. With severe rhabdomyolysis, the aminotransferases may remain abnormal for 2 to 3 wk.There may be a period when CK has normalised but aminotransferases remain elevated.
Mathuret al[11]conducted an observational study of inflammatory myopathy patients and demonstrated that abnormal serum aminotransferases follow the CK levels. In 85 patients with inflammatory myopathy and a mean CK of over 5000 U/L,the peak CK level was strongly correlated with the AST (r= 0.87) and ALT (r= 0.84).At the peak CK level, the mean ± SD for the AST was 215 ± 227 U/L, and the mean ±SD for ALT was 137 ± 137 U/L. More importantly, aminotransferases normalised in 85% of patients at the time of CK normalisation after treatment[11].
In observational studies, the timing of the inciting injury relative to presentation or admission cannot always be accurately determined, and the biomarkers associated with rhabdomyolysis may be either rising or falling. Treatment with intravenous fluids often accelerates CK decline with little effect on aminotransferases, as CK is predominantly cleared by the kidneys but ALT is cleared by the liver itself.
EVIDENCE FOR LIVER DERIVED ALT IN RHABDOMYOLYSIS
So far, we assumed aminotransferases are released from injured muscle but there may be other mechanisms which cause liver injury. An earlier report suggested that proteases are released after rhabdomyolysis[23]. There have been other hypotheses but good evidence is not available. For an indirect mechanism to have a role, injured muscles should release mediators which exert a systemic effect. The best candidate is probably oxidative stress.
Oxidative stress and inflammation
In rats, Plotnikovet al[24]found that myoglobin released from muscle causes lipid peroxidation of mitochondrial membranes, mitochondrial dysfunction and oxidative stress in renal tubular cells. Oxidative stress and lipid peroxidation of fatty acids may be responsible for increased F2-isoprostanes, which promote inflammation,endothelial dysfunction, vasoconstriction, and apoptosis[25]. In experimental rhabdomyolysis, Okuboet al[26]demonstrated that heme-activated platelets released from necrotic muscle promoted release of macrophage extracellular traps. The role of innate immune cells in inflammation and apoptosis is further supported by Kimet al[27], noting macrophage depletion is protective against AKI. In humans, Pereiraet al[28]supported the concept of systemic inflammation in a case report of a soldier who presented with exertional rhabdomyolysis. Investigations showed elevated levels of proinflammatory cytokines (interleukin-1 and interleukin-6) and microvascular dysfunction which persisted for one week.
There is paucity of basic science research in the liver context, particularly for a direct role of myoglobin in inciting liver injury. There are limited studies implicating oxidative stress in the liver related to rhabdomyolysis. Palet al[20]examined the effects of intense exercise in post-pubertal boys and girls, and demonstrated elevated serum CK and aminotransferases at 24 h and 48 h post-exertion. As evidence of oxidative stress, they showed that serum catalase activity and thiobarbituric acid-reactive substances (a marker of lipid peroxidation) were increased above baseline[20].Georgakouliet al[29]also reported similar findings of increased aminotransferases,catalase and total antioxidant capacity in heavy alcohol drinkers after moderate intensity exercise.
CLINICAL QUESTIONS AND NOVEL APPROACHES
In the setting of rhabdomyolysis, what is an expected level of ALT rise given the degree of muscle injury? In other words, is there a threshold for concern to justify further tests for liver disease? Alternatively, can we use other markers to help clinical decision making?
Adjusted analysis of traditional biomarkers
One simple idea is to adjust the aminotransferase level for other markers concurrently released by injured muscles but not liver. The most relevant in rhabdomyolysis is the CK/ALT ratio. Wanget al[30]examined the CK/ALT and CK/AST ratios in an experimental model of dystrophinopathy associated with acute liver injury, and in humans with dystrophinopathy. The authors reported that the CK/ALT ratio can differentiate between normal liver, acute liver injury and dystrophinopathy with or without liver injury, in their mouse model. In their patients, the CK/ALT ratio showed promise as it was less affected by age and other factors associated with muscle injury. Radkeet al[31]demonstrated a significantly higher CK/ALT and CK/AST ratios in patients with rhabdomyolysis compared to patients who overdose on acetaminophen. The median CK/ALT ratio was 37.1 with rhabdomyolysis compared to 5.8 with acetaminophen overdose. At a cut-off CK/ALT ratio of 15, the sensitivity was 67% and specificity was 77%[31]. To differentiate liver from muscle injury, a high specificity is desirable, thus the CK/ALT ratio is far from ideal but an improvement on ALT alone. Given the non-linear correlation between CK and ALT,the utility of the ratio of the log-transformed CK to log-transformed ALT should be further studied[6].
Novel biomarkers
Looking beyond CK and aminotransferases, plasma microRNAs (miRNAs) show promise. MicroRNAs are small, endogenous non-coding RNA molecules of around 22 nucleotides, which serves as gene regulators. Some microRNAs are cell and tissuespecific, and generally remain stable in plasma. They can be measured with sensitive molecular methods. In animal experiments, Laterzaet al[32]examined miR-122 and miR-133a for liver and muscle injury, respectively. miR-122 was elevated in liver but not muscle injury, and miR-133a was elevated in muscle but not liver injury. Baileyet al[33]conducted an extensive evaluation of miRNAs with the goal of utilising them in clinical trials to distinguish liver from muscle injury. Among the promising candidates were miR-1, miR-133a, miR-133b and miR-206 for muscle, and miR-122 and miR-192 for liver. In animal experiments, these biomarkers showed superior specificity to CK and aminotransferases for muscle and liver injury respectively[33].
Goldstein[34]reported on work of the Predictive Safety Testing Consortium, which included a muscle injury biomarker panel. The biomarkers were CK (mass assay),fatty acid-binding protein 3, skeletal troponin I and myosin light chain 3.Experimentally, the accuracy of these biomarkers was assessed in tetramethyl-pphenylenediamine induced skeletal muscle injury and acetaminophen-induced liver injury. AST levels could not be used to distinguish liver from muscle injury but the novel biomarkers showed higher specificity and correctly determined which tissue was injured histologically[34].
Quantitative analysis and potential confounders
Some studies suggest that the relationship between serum CK and aminotransferases is approximately linear. In muscular dystrophy, Wanget al[30]showed a positive linear correlation between CK and ALT (r= 0.75), and between CK and AST (r= 0.79). The levels of CK and aminotransferases were dependent on age but this variability was diminished with the CK/ALT ratio. However, data from Weibrechtet al[35]suggested that neither ALT nor peak CK is normally distributed in rhabdomyolysis. Limet al[6]confirmed this, and showed by linear and polynomial regression that the best functional form of this association is a linear relationship between the log-transformed CK and log-transformed ALT. The log-transformed CK, AKI stage, chronic liver disease and age together accounted for 46% of the observed variance in ALT. It is also possible to predict the ALT based on a regression model with these factors. In the worst case scenario, it was not common (< 5% chance) for the predicted serum ALT to exceed 500 U/L (for peak CK up to 160000 U/L), on average[6]. Even extrapolating to a peak CK of 400000 U/L, it was unlikely (< 1% chance) for it to exceed 800 U/L.
In such quantitative studies, consideration of confounding is important. One important factor is kidney function. Aminotransferases are much higher in patients with rhabdomyolysis and AKI compared to those without AKI[6,36]. On the other hand,there is an ordinal relationship between chronic kidney disease (CKD) and baseline aminotransferase levels. Compared to healthy individuals, patients with pre-dialysis CKD have lower aminotransferase levels, while patients on dialysis have the lowest levels[37,38]. Serum aminotransferases are also affected by age. In patients with rhabdomyolysis, Lau-Hing Yimet al[39]noted that peak CK showed a negative linear correlation with age (r= -0.42). However, AST tends to be more stable and as a result,the AST/ALT ratio increases with age[40,41]. Elinavet al[42]proposed an inverted Ushaped relationship between age and ALT. In their analysis, they included patients with a wide age range and showed that ALT peaked at 40-55 years. In multiple regression, age-squared and sex showed a statistically significant association with ALT activity[42]. Finally, there may be a sex difference as well, with some studies indicating that females have a lower baseline aminotransferase and CK levels than men[42,43], while the post-exercise rise in CK was lower in females[19]. In addition to age and sex, paediatric studies have also showed that body mass index and pubertal stage influenced ALT levels[44].
CONCLUSION
In patients with an isolated rise in aminotransferases, rhabdomyolysis should be considered in the differential diagnosis but current diagnostic tools do not have adequate specificity to differentiate liver injury from isolated muscle injury. Further research is required to meet this clinical need, and novel approaches and biomarkers may prove useful. The predicted ALT from regression modelling and the biochemical pattern and trajectory may be useful adjuncts to guide decision making whether more extensive or invasive tests for liver disease is warranted in patients with rhabdomyolysis.
ACKNOWLEDGEMENTS
I would like to thank Marcus Robertson, my gastroenterology colleague, for his insightful comments on this topic.
杂志排行
World Journal of Gastroenterology的其它文章
- Is aggressive intravenous fluid resuscitation beneficial in acute pancreatitis? A meta-analysis of randomized control trials and cohort studies
- Technetium-99m-labeled macroaggregated albumin lung perfusion scan for diagnosis of hepatopulmonary syndrome: A prospective study comparing brain uptake and whole-body uptake
- Predictors of outcomes of endoscopic balloon dilatation in strictures after esophageal atresia repair: A retrospective study
- Serum N-glycan markers for diagnosing liver fibrosis induced by hepatitis B virus
- Double-balloon endoscopic retrograde cholangiopancreatography for patients who underwent liver operation: A retrospective study
- Prognostic factors and predictors of postoperative adjuvant transcatheter arterial chemoembolization benefit in patients with resected hepatocellular carcinoma