Surgical outcome of laparoscopic sleeve gastrectomy and Roux-en-Y gastric bypass for resolution of type 2 diabetes mellitus: A systematic review and meta-analysis
2020-03-12SalmanYousufGurayaTimStrate
Salman Yousuf Guraya, Tim Strate
Abstract BACKGROUND Bariatric procedures are considered superior to medical therapies in managing type 2 diabetes mellitus (T2DM). Laparoscopic Roux-en-Y gastric bypass(LRYGB) and laparoscopic sleeve gastrectomy (LSG) are the most commonly used procedures for weight loss and comorbidity resolution worldwide.However, it is not yet known whether the degree of T2DM is influenced by the choice of bariatric procedure.AIM To quantitatively compare T2DM resolution over 1-5 years follow-up by LRYGB and LSG in morbidly obese patients.METHODS We searched the selected databases for full-text English language clinical studies that compared the effectiveness of LRYGB and LSG for T2DM resolution. Review manager 5.3 was used for data analysis, and the overall effect summary was represented in a forest plot.RESULTS From 1,650 titles retrieved by an initial search, we selected nine studies for this research. We found insignificant differences for T2DM resolution by LRYGB and LSG, with an odds ratio of 0.93 (95%CI: 0.64-1.35, Z statistics = 0.38, P = 0.71).Additionally, subset analyses for T2DM resolution showed insignificant differences after 24 mo (χ2 = 1.24, df = 4, P = 0.87, overall Z effect = 0.23), 36 mo (χ2= 0.41, df = 2, P = 0.81, overall Z effect = 0.51), and 60 mo (χ2 = 4.75, df = 3, P =0.19, overall Z effect = 1.20) by LRYGB and LSG. This study reports a T2DM remission rate of 82.3% by LRYGB and 80.7% by LSG.CONCLUSION This study reports similar T2DM resolution rates by both LRYGB and LSG during 1-5 years of follow-up. However, long-term follow-up of 10 years is needed to further substantiate these findings.
Key words: Morbid obesity; Type 2 diabetes mellitus; Laparoscopic sleeve gastrectomy;Laparoscopic Roux-en-Y gastric bypass
INTRODUCTION
Bariatric surgery is effective in treating morbid obesity, and in the resolution of its associated co-morbidities including metabolic syndrome, hyperlipidemia, type 2 diabetes mellitus (T2DM), sleep apnea, osteoarthritis, and psychological disorders[1].Out of a host of surgical remedies for morbid obesity, laparoscopic Roux-en-Y gastric bypass (LRYGB) and laparoscopic sleeve gastrectomy (LSG) remain the most commonly performed bariatric surgery procedures worldwide[2]. Both LRYGB and LSG have been shown to be safe, feasible and effective in accomplishing excess weight loss and resolution of co-morbidities[3,4]. Literature has shown a rapid escalation in the prevalence of T2DM and its associate complications, particularly cardiovascular[5],gallstones[6], peripheral arterial system and foot ulcers[7,8], stroke[9], and colorectal cancer[10]. In this perspective, bariatric procedures such as LRYGB and LSG have been successfully used for the resolution of T2DM and its comorbidities[11].
The mechanisms of T2DM resolution by LRYGB and LSG are largely unknown. It has been postulated that changes in gastrointestinal hormone secretions following LRYGB account for the resolution of T2DM, as the duodenum and upper jejunum are bypassed for direct delivery of nutrients to the midgut[12]. In contrast, weight loss induced by LSG is mediated by a primarily restrictive mechanism that leads to the simultaneous resolution of T2DM.
Literature has reported a T2DM resolution rate of 81.2% by LRYGB and 80.9% by LSG[13]. However, the selection of weight loss procedure is influenced by a wealth of factors. Praveenrai et al[14]proposed that the choice of bariatric surgery procedure is primarily driven by therapy goals (weight loss or glycemic control), associated gastroesophageal reflux or nutritional deficiencies, patient preferences and expertise of the surgeon. Generally, LRYGB is recommended for patients with long-standing,refractory T2DM with low serum C peptides, and LSG for other patients with morbid obesity. Interestingly, the majority of patients prefer LSG over LRYGB for the weight loss and resolution of associated metabolic disorders. In a double blind randomized clinical trial by Lee et al[15], the authors investigated T2DM resolution by LRYGB and LSG (fasting glucose 126 mg/dL and HbA1c 6.5% without anti-glycemic treatment)[15].The study concluded that the patients in the LRYGB group had greater weight loss, a lower waist circumference, and had rapid T2DM regression and lipid control compared to LSG. On the other hand, Vidal et al[16]showed that LSG was as effective as LRYGB in securing the resolution of T2DM and metabolic syndrome at a 12-mo follow-up after surgery. Similarly, in a systematic review of randomized clinical trials by Osland et al[17], the authors reported significant remission of T2DM by both LRYGB as well as by LSG across all stages of follow-up.
There seems to be no standard consensus about the superiority of LRYGB or LSG in achieving the resolution of T2DM. The available data are scarce, and very few studies have rigorously compared the outcome of LRYGB and LSG for attaining remission of T2DM in obese patients. This systematic review and meta-analysis provides quantitative comparison of the effectiveness of LRYGB and LSG for the resolution of T2DM in morbidly obese patients.
MATERIALS AND METHODS
Literature search
In January 2019, this systematic review and meta-analysis was performed using the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)[18]. The Medical Subject Headings (MeSH) terms used for systematic review included: Morbid obesity, type 2 diabetes mellitus, laparoscopic sleeve gastrectomy, laparoscopic Roux-en-Y gastric bypass, and fasting blood glucose.The databases of PubMed, Ovid, Wiley online library, Cochrane library, CINAHL, ISI Web of knowledge, ScienceDirect, and EBSCO were searched for full-text English original clinical studies published from Jan 2013 to Jan 2018. The original studies that compared the effectiveness of LSG and LRYG for the resolution of T2DM in morbidly obese patients during 1-5 years of follow-up were included in this search. The remission of T2DM was considered when HbA1c < 6.0% without anti-diabetic therapy was achieved by bariatric procedures[19]. As defined by review articles, editorials,expert opinions, commentaries, and short communications were excluded. The original studies with incomplete data as mean ± SD (for continuous outcome),number, percentage (for dichotomous outcome) or an average follow-up of less than one year were excluded. In addition, research articles that attempted to determine surgical outcomes of LSG and LRYGB in patients with a body BMI < 27 kg/m2or <18- or > 65-years-old were excluded. The indicators of glycemic control were HbA1C and fasting blood glucose levels. Finally, research showing combined data of revision or conversion bariatric procedures was not included in this study.
Data extraction and synthesis
During two rounds of searches in the selected databases, 1650 studies were retrieved.Review of the searched titles showed 496 duplicate and 960 irrelevant titles that were excluded from further literature review. At the next stage of analysis of the 194 titles,another 125 articles were excluded, as the contents and study outcomes did not match our systematic review primary outcomes. As many as 69 articles were found to be relevant, as they compared the effectiveness of LSG and LRYGB for T2DM resolution.However, during full text review of these 69 articles, 60 studies were further excluded, as they contained incomplete data and inconsistent findings. Finally, a total of nine relevant studies were selected in this meta-analysis (Figure 1).
Quality assurance
Two independent researchers (Salman Yousuf Guraya and Tim Strate) searched,analyzed, reviewed the retrieved titles and full-text articles for suitability and study representativeness. Using the Cochrane Collaboration tool, we found some element of selection bias that was reflected by the blinding of participants and personnel preferences (performance bias)[10,20]. The risk of bias and conflict of interest were eliminated by discussions and by reaching a general consensus.
Quantitative analysis of data
Review Manger 5.3 software, developed by Cochrane Library, was used for the quantitative analysis of data from the selected studies in this meta-analysis[21]. The findings of the meta-analysis were graphed on a forest plot, which quantitatively demonstrates the consistency and reliability of results. In a forest plot, the effect size of each study is computed as an outcome measure, and pooled effect summary is calculated to determine heterogeneity across sleeted studies. Statistically, Q tests reflect heterogeneity in the selected studies using the null hypothesis that all studies are identical. In this meta-analysis, the I squared (I2) statistical analysis was used to validate heterogeneity in percentage terms[20]. In the case of low heterogeneity (P >0.10, I2< 50%), a fixed effects model is recommended. On the other hand, a random effects model is employed in the case of higher heterogeneity (P < 0.10 or I2> 50%).The Tau squared (Tau2) test is applied to estimate variance in the calculated data using the random effects model. We estimated publication bias by visual inspection of the funnel plot, and the level of significance in this study was considered as 5% (P < 0.05).

Figure 1 Schematic algorithm for selection of studies in the meta-analysis for comparison of effectiveness of type 2 diabetes mellitus resolution by laparoscopic sleeve gastrectomy and Roux-en-Y gastric bypass.
RESULTS
A close comparative analysis of the resolution of T2DM by LSG and LRYGB is illustrated in Figure 2. We found that the Cochrane Q (χ2= 154.43) test was significant at 5% (P < 0.05). This rejected the null hypothesis that all studies were identical. Due to substantial heterogeneity (I2= 88%), a random effect model was deemed necessary.In our meta-analysis, the forest plot generated by Review Manager 5.3 for the comparison of resolution of T2DM by LSG and LRYGB showed insignificant differences for T2DM resolution by LSG and LRYGB, with an odds ratio of 0.93(95%CI: 0.64-1.35, Z statistics = 0.38, P = 0.71), as shown in Figure 3. Figure 4 includes a forest plot that compares the resolution of T2DM by LSG and LRYGB after 24, 36 and 60 mo. Insignificant differences are reported between the two weight loss surgical procedures. The scientific evidence of symmetry and homogeneity of the selected articles for effectiveness of LSG and LRYGB in resolution of T2DM is demonstrated in the funnel plot in Figure 5. The remission rate of T2DM by LRYGB and LSG is estimated to be 82.3% and 80.7%, respectively. Characteristics of the selected studies,including the complete citation of articles, study design, number of patients at the time of surgery, and key outcomes by both LSG and LRYGB are shown in Table 1.
DISCUSSION
Our systematic review and meta-analysis showed insignificant differences in T2DM resolution by LSG and LRYGB. Additionally, a deeper analysis of subgroups also demonstrated insignificant differences after 24 mo (χ2= 1.24, df = 4, P = 0.87, overall Z effect = 0.23), 36 mo (χ2= 0.41, df = 2, P = 0.81, overall Z effect = 0.51), and 60 mo (χ2=4.75, df = 3, P = 0.19, overall Z effect = 1.20) in T2DM resolution by LSG and LRYGB.In the absence of a clear consensus about the superiority of LRYGB over LSG for T2DM resolution, the findings of our study provide landmark evidence for the management of morbid obesity and its comorbidities.
In the clinical trial by Yang et al[22], the researchers followed up with patients after LRYGB and LSG for 3 years, and have reported similar T2DM remission rates. Similar results have been reported elsewhere[23,24]. In the same study, complete T2DM resolution rates, as defined by HbA1c < 6.0% without anti-diabetic therapy, were 78.6% in the LSG group and 85.2% in the LRYGB group. These findings are in agreement with the previously published prospective clinical studies on patients with a BMI > 35 kg/m2[25,26]. However, in the randomized controlled trial by Lee et al[15], the investigators argued that LRYGB was superior in achieving better blood glucose control than LSG at 1 and 5 years after surgery on patients with a BMI of 25-35 kg/m2.Nonetheless, our systematic review and meta-analysis could not find superiority of LRYGB or LSG in T2DM throughout 1-5 years of follow-up.
In the study by Perrone et al[27], the authors compared long-term results on weightloss and comorbidity resolution for LRYGB and LSG on a cohort of 304 consecutive patients. Though LSG was more effective in the percentage of excess weight loss at 180 d and at 1 year of follow-up, however, LRYGB and LSG showed similar results at 5 years of follow-up; 72.34 vs 70.26, respectively. Generally, LRYGB was shown to be more effective in T2DM remission than LSG. These findings reflect the lack of a gold standard bariatric procedure that can help achieve excess weight loss and comorbidity resolution[28]. The study by Wallenius et al[29]compared early weight-independent and later weight-dependent influence by LRYGB and LSG on glycemic control. Initially,there was a similar drop in fasting blood glucose levels in both the LRYGB and LSG groups; 8.1 ± 0.6 mmol/L vs 8.2 ± 0.4 mmol/L, 2 d; 7.8 ± 0.5 mmol/L vs 7.4 ± 0.3 mmol/L, 21 d; 6.6 ± 0.4 mmol/L vs 6.6 ± 0.3 mmol/L, respectively. This study reported similar effects on glycemic controls by both surgical procedures. On the other hand, the study by Gray et al[30]reported a greater improvement in T2DM,hypertension, hyperlipidemia, and gastroesophageal reflux disease by LRYGB over LSG during a median follow-up of 39 mo. From a different perspective, some investigators have recommended LRYGB as a gold standard for effective weight loss and resolution of comorbidities, and to keep LSG as an attractive substitute[31,32].Unfortunately, as of today, the literature is divided on this argument, and we need more concrete evidence to validate these observations.
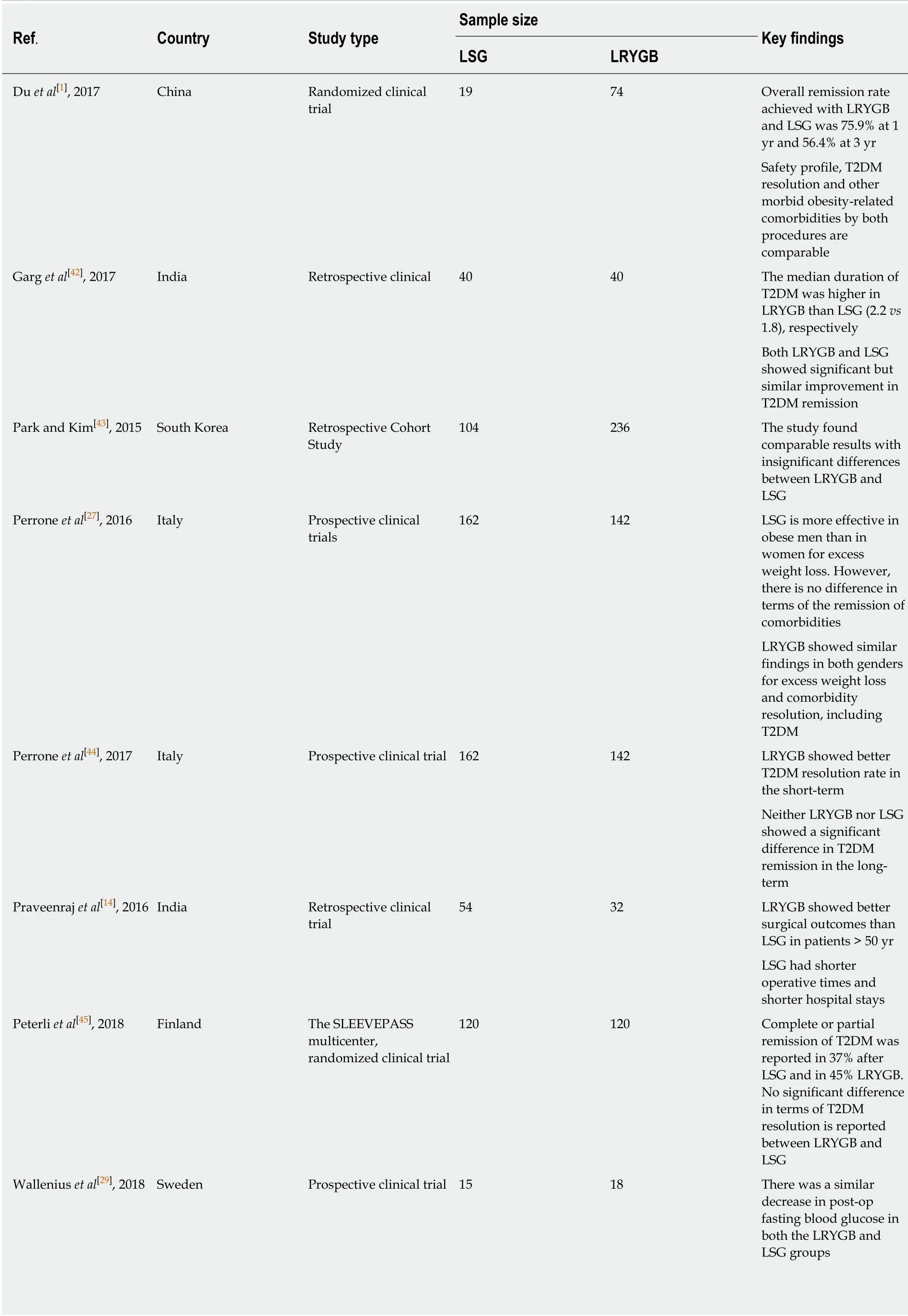
Table 1 Characteristics of the nine selected studies comparing type 2 diabetes mellitus resolution by laparoscopic sleeve gastrectomy and Roux-en-Y gastric bypass in this study

LSG: Laparoscopic sleeve gastric bypass; LRYGB: Laparoscopic Roux-en-Y gastric bypass; T2DM: Type 2 diabetes mellitus.
By and large, the mechanisms of T2DM remission by LRYGB and LSG are unclear,although several hypotheses exist. The literature has shown a greater inclination toward LSG as an anti-diabetic surgical remedy, which induces early glucose homeostasis similar to that of LRYGB[33]. In an interesting study by Nannipier et al[34],the authors investigated the mechanism for T2DM remission by GI hormones, and found similar results from LRYGB and LSG. The study concluded that glucagon-like peptide (GLP-1) and polypeptide YY (PYY) were the key predators of glucose homeostasis in the post-operative follow-up. Though the exact mechanisms underlying better glucose homeostasis following LSG is uncertain, a fall in ghrelin levels and unexpected changes in serum levels of distal intestinal hormones (GLP-1,GLP-2 and PYY) are considered to play some role. Furthermore, insulin resistance is decreased and incretin hormones levels are substantially elevated. On the other hand,since LRYGB bypasses the proximal intestine, a host of neurohormonal changes ensue, particularly low insulin resistance, as well as changes in ghrelin, GLP-1, GLP-2 and PYY level[35]. On a similar note, Peterli et al[36]found that 1 year after operation,post-prandial serum cholecystokinin levels increased less in the LRYGB than in the LSG group. The authors have argued that bypassing the foregut is not the sole underlying reason for improved glucose homeostasis.
LSG has several advantages over LRYGB: Easier to perform, preserves pylorus and antrum with less chance of dumping syndrome, no risk of internal herniation, and decreased risk of nutritional deficiencies[37,38]. In terms of its shorter learning curve,LSG is gaining popularity over LRYGB among bariatric surgeons. The results of our meta-analysis would further strengthen the value of LSG in achieving weight loss and remission of comorbidities, particularly T2DM due to its comparable profile with LRYGB. Additionally, improving surgeons skills[39]and adhering to professional codes tend to lead to better surgical outcomes[40].
In conclusion, this study reports similar T2DM resolution rates by both LRYGB and LSG during 1 to 5 years of follow-up. However, long-term follow-up of 10 years is needed to further endorse these findings.
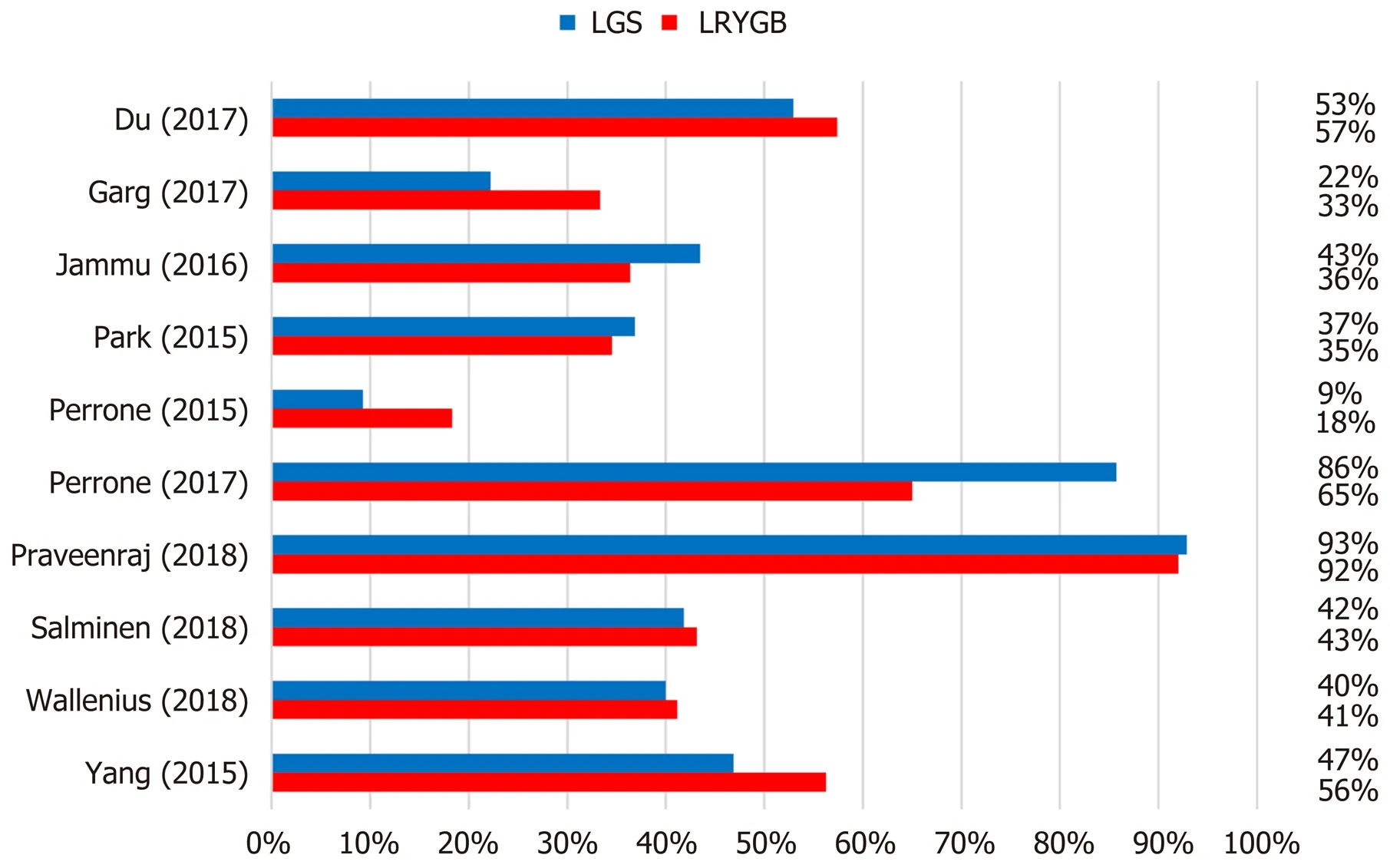
Figure 2 Comparison of the resolution of type 2 diabetes mellitus between laparoscopic sleeve gastrectomy and laparoscopic Roux-en-Y gastric bypass.

Figure 3 Forest plot comparing the resolution of type 2 diabetes mellitus by laparoscopic sleeve gastrectomy and laparoscopic Roux-en-Y gastric bypass.

Figure 4 Forest plots comparing the resolution of type 2 diabetes mellitus by laparoscopic sleeve gastrectomy and Roux-en-Y gastric bypass after 24 mo(A), 36 mo (B), and 60 mo (C). LSG: Laparoscopic sleeve gastrectomy; LRYGB: Laparoscopic Roux-en-Y gastric bypass; T2DM: Type 2 diabetes mellitus.

Figure 5 Funnel plot illustrating the symmetry of selected studies for type 2 diabetes mellitus resolution by laparoscopic sleeve gastrectomy and Roux-en-Y gastric bypass. LSG: Laparoscopic sleeve gastrectomy; LRYGB: Laparoscopic Roux-en-Y gastric bypass; T2DM: Type 2 diabetes mellitus.
ARTICLE HIGHLIGHTS
Research background
There is a staggering rise in the incidence of obesity worldwide. A sedentary lifestyle, unhealthy food, and multiple comorbidities such as Type 2 diabetes mellitus (T2DM), hypertension and hyperlipidemia are major risk factors for obesity. In order to curtail the epidemic of obesity, a host of treatment strategies are offered, including lifestyle change, dietary consultations,medications, as well as surgical therapies. Of these, surgical remedies carry great promise in achieving effective weight loss and the resolution of comorbidities. Generally, bariatric procedures are considered superior to medical therapies in treating obesity-related T2DM.Though Laparoscopic Roux-en-Y gastric bypass (LRYGB) and Laparoscopic sleeve gastric bypass(LSG) are the most popular bariatric surgical procedures worldwide, there is no consensus about the superiority of one procedure over the other in terms of the resolution of obesity-related T2DM.
Research motivation
This study determines the effectiveness of LSG and LRYGB for treating obesity-related T2DM.Short-, mid- and long-term follow-up results after bariatric surgery were analyzed. The literature is divided about the estimated outcomes by various bariatric surgical procedures in achieving excess percentage weight loss and T2DM. This study quantitatively compares the resolution of T2DM by LSG and LRYGB.
Research objectives
We conducted the current study to quantitatively compare the impact of LSG and LRYGB in T2DM resolution over 1 to 5 years post-surgery follow-up.
Research methods
We conducted a literature search by using selected keywords in pre-defined databases for fulltext English language clinical studies. This study compared short-, mid- and long-term outcomes of T2DM resolution by LRYGB and LSG. The data from all selected studies were analyzed by Review Manager®5.3. Forest plots were generated for overall effect summaries. The homogeneity of the selected studies was determined by funnel plots and, finally, the findings were interpreted and compared with published reports.
Research results
A total of 1650 titles were retrieved from the selected databases. Using PRISMA guidelines, both investigators shortlisted and then finally selected nine studies for further analysis. We report a T2DM remission rate of 82.3% by LRYGB and 80.7% by LSG. This study shows insignificant differences for T2DM resolution by LRYGB and LSG, with an odds ratio of 0.93 (95%CI: 0.64-1.35, Z statistics = 0.38, P = 0.71). Deeper analysis of subsets for T2DM resolution for short-, midand long-term follow-up showed similar results at 24 mo (χ2= 1.24, df = 4, P = 0.87, overall Z effect = 0.23), 36 mo (χ2= 0.41, df = 2, P = 0.81, overall Z effect = 0.51), and 60 mo (χ2= 4.75, df = 3,P = 0.19, overall Z effect = 1.20).
Research conclusions
This study provides comparative quantitative evidence regarding the role of LSG and LRYGB in treating obesity-related T2DM. Technically, compared to LRYGB, LSG is much easier to perform,and takes significantly shorter operative time. Being a relatively easier bariatric surgical procedure, LSG may be favored in achieving T2DM resolution. However, before we can reach a consensus, the results of long-term follow-up over 10 years should be quantitatively analyzed.By and large, this study implies a comparable achievement in T2DM resolution by both procedures up to 5 years follow-up.
Research perspectives
LSG and LRYGB, although quite different bariatric surgical procedures, achieve similar T2DM resolution up to 5 years post-surgery. Future research should investigate different neurohormonal mechanisms that lead to a common goal of T2DM resolution by both surgical procedures.
ACKNOWLEDGEMENTS
We acknowledge the support in literature review and meta-analysis provided by Mr B Bilal, Associate Professor Hubei Centre for Accounting Development Research School of Accountancy Hubei University of Economics, Wuhan, China.
杂志排行

World Journal of Gastroenterology的其它文章
- Diagnosis and management of a solitary colorectal juvenile polyp in an adult during follow-up for ulcerative colitis: A case report
- Diverting colostomy is an effective and reversible option for severe hemorrhagic radiation proctopathy
- Prognostic value of preoperative weight loss-adjusted body mass index on survival after esophagectomy for esophageal squamous cell carcinoma
- Haemoglobin, albumin, lymphocyte and platelet predicts postoperative survival in pancreatic cancer
- Neoadjuvant chemotherapy vs upfront surgery for gastric signet ring cell carcinoma: A retrospective,propensity score-matched study
- Downregulation of orosomucoid 2 acts as a prognostic factor associated with cancer-promoting pathways in liver cancer