Epidemiology of syndactyly in New York State
2019-11-14IshaanSwarupYiZhangHuongDoAaronDaluiski
Ishaan Swarup,Yi Zhang,Huong Do,Aaron Daluiski
lshaan Swarup,Aaron Daluiski,Department of Orthopaedic Surgery,Hospital for Special Surgery,New York,NY 10021,United States
Yi Zhang,Huong Do,Healthcare Research Institute,Hospital for Special Surgery,New York,NY 10021,United States
Abstract
Key words:Congenital hand anomaly;Epidemiology;Incidence;Syndactyly
INTRODUCTION
Syndactyly is a congenital anomaly characterized by an abnormal connection between adjacent digits[1].Syndactyly is considered to be one of the most common hand malformations[2];however,there is limited epidemiologic data in the literature[3].The incidence of syndactyly is most commonly reported to be as low as 2 per 10000 live births,but it has also been reported to be as high as 1 per 2000 to 3000 live births[4-9].However,the majority of these studies have been hospital-based or extrapolated from clinic visits[10].A study using Swedish national registries found the incidence of differentiation anomalies to be 10.5 per 1000010,and a study from Western Australia reported the incidence of all upper extremity anomalies to be 1 in 506 with failure of differentiation being the most common anomaly[11].However,syndactyly was not specifically identified as a subgroup in either study.A recent study found the prevalence of syndactyly to be 1.3 per 10000 in New York State;however,this study focused on disease prevalence and used a congenital malformations registry that is susceptible to underreporting[12].
Surgical management for syndactyly may be performed as early as 6 mo of age,but it is frequently performed between 12 to 18 mo of age[13].Surgery is not recommended in children under the age of 6 mo due to the inherent anesthetic risk,but it should not be performed too late due to the potential risk of abnormal development of cerebral cortex patterns and the effect on adjacent digits[2,13,14].While acceptable results have been reported with delaying surgery until age 4 or 5[13],surgical management is typically recommended between 2 and 3 years of age for optimal outcomes[2].Outcomes are satisfactory in the majority of cases[15,16].However,an increase in complications and re-operation rates has been previously associated with age,other ipsilateral hand anomalies,and split-thickness skin grafting[2,4,15].Given the importance of timely surgical management,issues relating to access of care such as insurance status,geographic factors,and availability of specialized hand surgeons may influence patient outcomes,but these factors have not been previously studied.Several barriers to care for congenital conditions have been described in other specialties including patient education level,accessibility,and socioeconomic factors[17].In addition,insurance status and distance to care are known to be important barriers to care in pediatric surgical care[18-20].
As a whole,there is a paucity of epidemiologic studies using modern,populationbased databases.Furthermore,it is not known when these children are undergoing operative management and whether social or demographic factors limit access to care.In this study,we use a state database to describe the incidence of syndactyly in the state of New York.We also describe the age at which children are undergoing surgery,and whether insurance status or access to care is associated with operative management.We hypothesize that the disease incidence will be low and the majority of children will have surgery before age two.In addition,we hypothesize that insurance status and access to care are potential barriers to care in patients with syndactyly.
MATERIALS AND METHODS
A retrospective study was conducted using the New York Statewide Planning and Research Cooperative System (SPARCS) database.SPARCS is a comprehensive data reporting system established in 1979 that collects patient level data for each inpatient stay,ambulatory surgery procedure,and emergency department admission from nonfederal healthcare facilities in New York State.
Newborn admissions from 1997 to 2014 with an International Classification of Diseases,Ninth Revision,Clinical Modification (ICD-9-CM) diagnosis code for syndactyly (755.1X) were identified.We included patients with simple and complicated syndactyly,and excluded patients with unknown sex or non-NY residence.Data regarding patient sex and insurance status were obtained from the newborn admission record.Annual incidence for the overall study period and each year individually was calculated by dividing the number of newborns with syndactyly by the total number of live births in New York State each year.Annual live birth counts for 1997 to 2014 were obtained from the New York State Department of Health Vital Statistics website.
Current pocedural terminology (CPT) codes (26560,26561,26562,28280,28345) and ICD-9-CM procedure codes (86.85) were used to determine whether the identified newborns had a subsequent syndactyly-related procedure.Variables obtained from the surgery visit were age at time of surgery,additional procedures performed,surgeon license number,and hospital identifier.We used CPT codes (14301,15120,15200,15240,15241,15760) and ICD-9-CM procedure codes (86.61,86.62,86.63,86.69,86.70,86.72,86.73,86.89) to determine whether patients having syndactyly surgery had concomitant skin grafting procedures.In addition,surgeon license number was used to obtain surgeon specialty information by querying state and public databases or the professional and personal websites for the surgeon.Hospital identifier was used to obtain information on residency accreditation for the institution from the American Hospital Association Annual Survey database.Hospitals with residency accreditation were classified as teaching hospitals.
Univariate comparisons between syndactyly patients with and without surgical treatment were performed using the Chi-Square test.A geographic heat map of syndactyly procedure frequency was generated with SAS PROC GMAP.Data analysis were performed using SAS 9.4 (SAS Institute,Inc.,Cary,NC,United States).Significance level was set at 0.05.
RESULTS
From 1997 to 2014 there were 3306 cases of syndactyly in New York State (Table1).The annual incidence ranged from 0.062% to 0.085% with an overall incidence of 0.074% (1 per 1350 live births) (Figure1).There were 1164 females (35%) and 2142 males (65%) in the cohort.
Of these patients,178 patients (5%) had a syndactyly procedure in New York State.Approximately 67% of these patients were male (119 cases) and 33% were female (59 cases).Forty-four percent of these patients had a syndactyly surgery before age one(78 cases);35% had surgery at age one (63 cases);and 21% at or after age two (37 cases).There was an equal mix of Medicaid and private insurance (47% each).
Almost all surgeries (183) were performed in New York County (Manhattan),Monroe County (Rochester),Albany County (Albany),Westchester County,Erie County (Buffalo),Bronx,and Kings County (Brooklyn) (Figure2).Approximately,87% of cases were performed at teaching hospitals,and slightly more than half of syndactyly releases were performed by plastic surgeons (52%) followed by orthopaedic surgeons (42%).In addition to syndactyly release,skin grafting procedures were also performed in 35 cases (15%).
Some significant differences were noted between patients that did and did not undergo surgery in New York State (Table1).Patients having surgery in New York State were more likely to have Medicaid insurance compared to patients who did not have surgical treatment in New York (47%vs37%,P= 0.02).However,there were no significant differences in sex between patients that did or did not have surgery in New York State (P= 0.55).
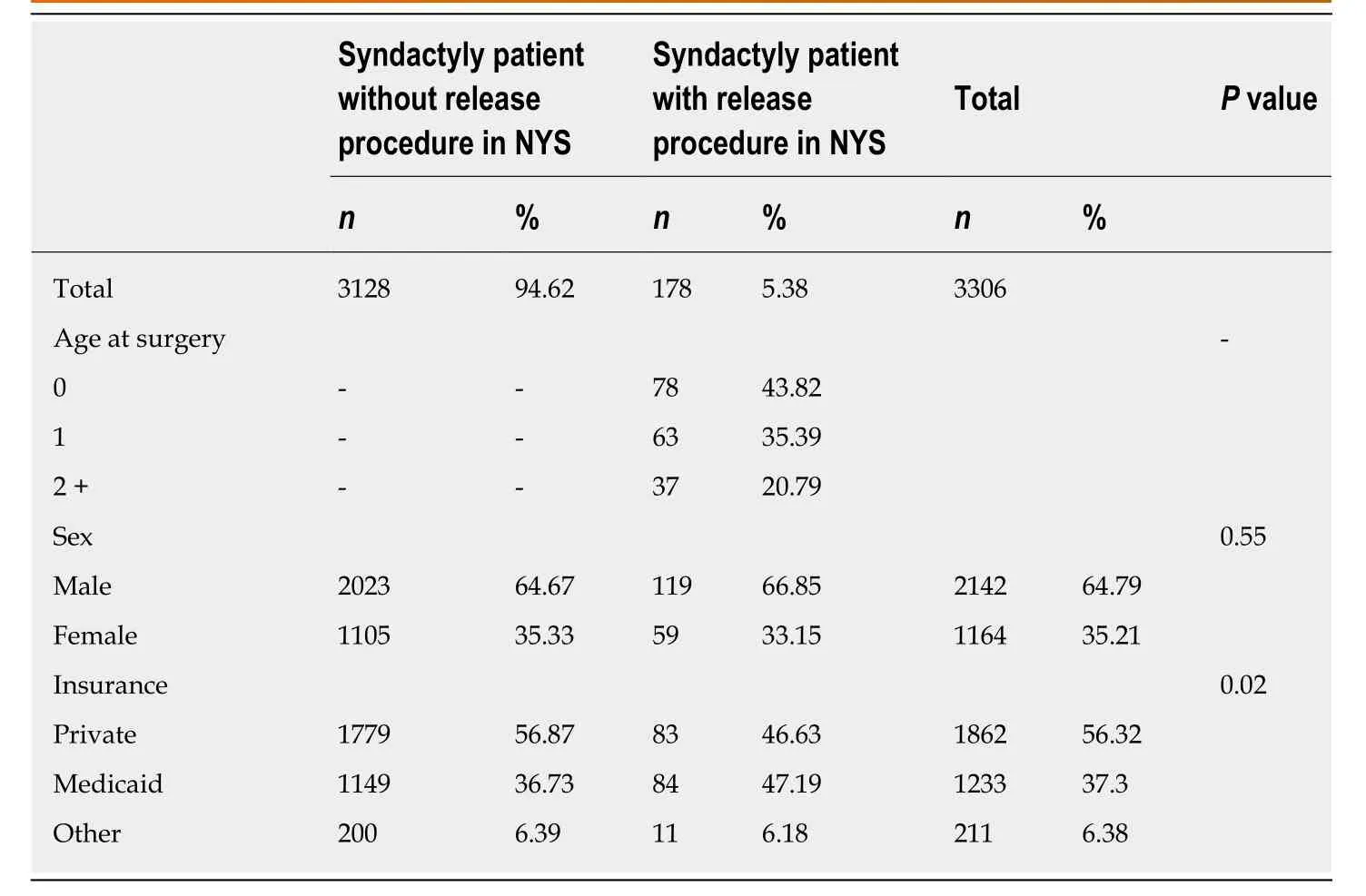
Table1 Patient demographic information of those with and without syndactyly procedures
DISCUSSION
Syndactyly occurs in 7 per 10000 live births in New York State.The reported incidence in this study is higher than some previous reports[4-8],and the higher incidence in New York State may reflect an increasing incidence,population differences,or increase in reporting of this condition.There are varying reports of syndactyly incidence in the literature ranging from 2 to 10 per 10000 live births[4-8,10,11],and this study provides an estimate of incidence in an American population.
Only 5.4% of patients had syndactyly surgery in New York State.Among the surgical patients,most of the operations were performed before the age of two,and a minority of patients needed skin grafting.While surgical release is the recommended treatment for syndactyly and re-operation rates are well-published[21-24],there is limited data on the rates of surgery.Due to the paucity of studies on rates of surgery,we are unable to compare our surgical rates to other populations.
The vast majority of patients with a diagnosis of syndactyly in New York State did not have surgery in the state.This finding suggests that patients are either not undergoing surgical repair or,more likely,they are traveling out of state for care.There are several factors that may affect access to care,including the availability of specialized hand surgeons;proximity to urban medical centers and teaching hospitals;as well as socioeconomic factors and insurance coverage.More specifically,the majority of syndactyly surgeries in New York State are performed by plastic surgeons in urban,teaching hospitals.
Furthermore,payer data shows that patients having surgery in New York State were more likely to have Medicaid insurance compared to patients not having surgery.One possible reason for this might be that patients with private insurance and possibly higher socioeconomic status may be leaving the state to receive care at specialized centers.This finding underscores the need for greater availability of surgical care for the treatment of congenital hand differences in New York State.
This study has several strengths.Firstly,it is a large study that includes all patients in New York State with a diagnosis of syndactyly at birth.This data provides an epidemiologic assessment of incidence and surgical management,and to our knowledge,this is the first study focusing specifically on the incidence of syndactyly in an American population.Recently,Goldfarbet al[12]reported the prevalence of congenital hand anomalies using the New York Congenital Malformations Registry,however,their study focused solely on disease prevalence;used a database that does not require confirmation of diagnosis;and they specifically note the potential for underreporting of syndactyly in their database.Furthermore,we are able to describe the surgical management for patients with syndactyly in our study,as well as explore factors that may affect management.Several of these factors have not been previously investigated,and our findings can be used to generate additional studies focusing on surgical management and access to care.

Figure1 Syndactyly incidence over time.
However,this study has several weaknesses as well.First of all,our study is limited by the limitations of any study utilizing an administrative database.For example,our results are susceptible to errors in reporting and coding,and the available data is less granular in nature and limited to care provided in New York State.Similarly,we used syndactyly-specific CPT codes and ICD-9-CM procedure codes to identify surgical treatment,and it is possible that we did not capture all procedures for syndactyly if they were performed in conjunction with other procedures or having more procedures than are retained in the record.In addition,we do not have access to any clinical or patient-reported outcome measures to determine outcomes after surgery.However,several previous studies have investigated re-operation rates and complications associated with surgical management[22-24].Lastly,these results are specific to patients residing in New York State and it is unclear whether these results are generalizable to other populations.However,our study provides useful information on the cohort of patients with syndactyly that were managed with surgery in New York State.
In conclusion,this study shows that the incidence of syndactyly is relatively high at 7 per 10000 live births.Most patients who underwent surgical treatment in New York State were under age two at the time of surgery;however,the majority of patients from New York State likely receive care elsewhere.The low rates of surgical management in New York State may be due to barriers to care including the availability of pediatric hand surgeons,proximity to urban medical centers and teaching hospitals,and insurance status.These factors underscore the need for specialized surgical care in New York State,and they should be considered by healthcare officials for resource management and planning.Additional research is needed to specifically understand the low rates of surgical management in New York State,as well as determine the outcomes of surgery in this population.
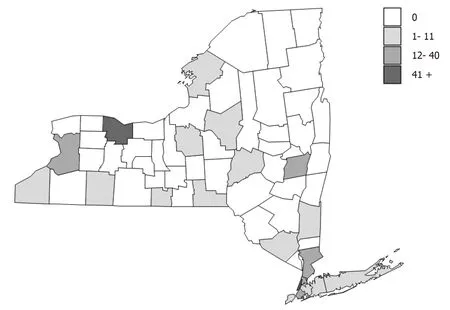
Figure2 Geographic distribution of syndactyly procedures in New York State.
ARTICLE HIGHLIGHTS
Research background
There is paucity of literature focusing on the incidence and surgical management of syndactyly.In addition,very few epidemiologic studies have used modern,statewide databases to understand the incidence of disease in the United States.
Research motivation
It is important to understand the incidence and surgical management of an important congenital hand anomaly.It is also important to understand rates of surgical management and potential barriers to care.
Research objectives
In this study,we describe the incidence and surgical management of patients with syndactyly in New York State using a statewide database.This study helps to identify the incidence of disease,rates of surgical management,and potential barriers to care.
Research methods
We conducted a retrospective study using the New York State Statewide Planning and Research Cooperative System database.We identified newborn records with a diagnosis of syndactyly to determine annual incidence,and searched subsequent records to determine rates of surgical management.Descriptive statistics and univariate analyses were performed on demographic and surgical information contained in the database.
Research results
We identified 3306 cases of syndactyly between 1997 and 2014 in New York State.The overall incidence was 0.074% or 7 cases per 10000 live births.In total,178 patients underwent surgical management in New York State and 79% of patients were under the age of two at the time of surgery.Approximately,87% of surgeries were performed at teaching hospitals,and 52% of procedures were performed by plastic surgeons.Patients having surgery in New York State were more likely to have Medicaid insurance compared to patients not having surgery.
Research conclusions
Syndactyly occurs in approximately 7 per 10000 live births,and the majority of patients undergoing surgical correction are treated before age two.There may be several barriers to care including the availability of specialized hand surgeons,access to teaching hospitals,and insurance status.
Research perspectives
Additional research is needed to determine the incidence of syndactyly in other populations,understand the low rates of surgical management in New York State,and describe the outcomes of surgery in this population.Statewide databases are well-suited for these types of studies.
