Posterior ankle impingement-an underdiagnosed cause of ankle pain in pediatric patients
2019-10-21IndranilKushareKristenKastanSachinAllahabadi
Indranil Kushare, Kristen Kastan, Sachin Allahabadi
lndranil Kushare, Kristen Kastan, Department of Orthopaedics, Texas Children’s hospital, The Woodlands, TX 77384, United States
Sachin Allahabadi, Department of Orthopaedics, University of California, San Francisco, CA 94143, United States
Abstract
Key words: Ankle impingement; Ankle pain; Os trigonum; Delayed diagnosis; Ankle arthroscopy; Pediatric
INTRODUCTION
Posterior ankle impingement syndrome (PAIS) is a common cause of posterior ankle pain that has been classically described in ballet dancers and soccer players[1-4]. It is caused by mechanical pinching of bony or soft tissue structures during terminal plantar-flexion in the posterior part of the ankle[1-5]. Even though it can present acutely, PAIS more commonly presents with chronic pain secondary to repetitive stresses in the posterior ankle with forced plantar-flexion activities. With several causes (soft tissue, bony, or both) and heterogenous pathological anatomic features,the diagnosis was coined as posterior ankle impingement “syndrome”[2,6]. This diagnosis is primarily made based on an accurate history and detailed clinical exam[2,3,7-9]. To our knowledge, there has not been any prior literature that highlights the delay in making this diagnosis in the pediatric and adolescent population. The aim of our study was to identify any delay in diagnosis and further characterize the misdiagnosed cases of posterior ankle impingement exclusively in the pediatric and adolescent population.
MATERIALS AND METHODS
Patient selection
This was a descriptive prospective study conducted at a tertiary children’s hospital after approval from the Institutional Review Board. The study included patients 18 years and younger from 2016 to 2019 who presented with posterior ankle pain, were diagnosed with posterior ankle impingement, and underwent arthroscopic debridement due to failure of conservative treatment. Informed written consent was obtained from all patients prior to enrollment in the study.
Collected data
Collected data included the following: Age, gender, previous diagnoses and treatment received, prior specialists seen for ankle pain, time to diagnosis from initial presentation, and radiologic imaging obtained-including plain radiographs and magnetic resonance imaging (MRI). Diagnosis of PAIS was made based on history and clinical exam (posterior joint line tenderness, pain on forced plantar flexion)supplemented by radiographic imaging. Delay in diagnosis was defined as the time between initial presentation to a medical provider with ankle pain until the diagnosis of PAIS was made. Indication for arthroscopic debridement was failure of conservative treatment which included rest and immobilization, with or without physical therapy. Visual Analogue scale (VAS) for pain and American Orthopedic Foot Ankle Society (AOFAS) ankle-hindfoot scores at presentation pre-operatively and post-operative follow-up visits were compared using the pairedtor Wilcoxon signed-rank tests with statistical significance set atP< 0.05. Descriptive statistical analyses were conducted and summarized as means with range values or frequencies with corresponding percentages.
RESULTS
Treatment outcome and statistical analysis
Prospective data was collected in 35 patients (16 males, 19 females). A total of 46 ankles were included with a mean patient age of 13 years (range 8.6-17.9). 33 (94%)patients had a delay in the diagnosis of PAIS from the initial presentation with symptoms to a medical provider, the average delay being 19 mo (range 0-60). 22/35(62%) patients were athletes, the most common sports included American football (4 patients), soccer and gymnastics (3 patients each). 25 (71%) patients had previously seen multiple health care professionals and specialists and were given multiple other diagnoses as a cause of their ankle pain (Table1). All 46 (100%) ankles had specific tenderness to palpation over the posterior ankle joint which was located between the peroneal tendons and Achilles tendon. 42 (91%) ankles had at least one preoperative radiograph obtained (Figure1), and 15 (43%) patients had multiple radiographs prior to actual diagnosis. The radiographs were reported “normal” with no significant findings by local radiologist in 31 (74%) exams. 30 (86%) patients (32 ankles) had an MRI study done, the most common findings of which were os trigonum (47%) (Figure2) or Stieda process (47%). 22 of the 32 ankles (69%) with an MRI performed had osseous edema indicative of the inflammation seen in PAIS.
Conservative treatment
All 35 (100%) patients had attempted and failed prolonged and exhaustive conservative management for several months. Conservative treatment included rest from sports and physical activities (including physical education at school),immobilization with boot, brace or cast, and/or physical therapy. One patient had a prior ankle corticosteroid injection. Pain typically subsided temporarily with conservative treatment but recurred with return to activity/sports. All 46 (100%)ankles had exquisite tenderness to palpation over posterior ankle joint, anterior to the Achilles tendon.
Surgical treatment
All 46 ankles had PAIS pathology, either soft tissue, bony, or a combination of both,confirmed during arthroscopic treatment, including os trigonum (Figure3), Stieda process, hypertrophic ligaments and synovium-these three were the most common findings seen in majority (42/46) of the ankles. Uncommon findings were cysts of the flexor hallucis longus tendonitis (FHL) (2 cases), and a low-lying FHL muscle belly (2 cases). At an average follow-up of 13.1 mo, there was significant improvement of mean VAS pain scale (pre-op 7.0 to post-op 1.2,P< 0.001) and mean AOFAS ankle scores (pre-op 65.1 to post-op 94,P< 0.001). Three patients had inadequate documentation; the remaining 32 (91%) patients returned to their previous level of activity/sports at average 7.8 wk after treatment. None of the patients had recurrence of symptoms at their last follow-up which supports our diagnosis of PAIS.
DISCUSSION
Posterior ankle impingement syndrome has been well-described in the literature,particularly in dancers and soccer players[1,2,4]. PAIS is due to the mechanical pinching of structures in the posterior ankle, which may be secondary to bony or soft tissue causes, or a combination of both[1,2]. An average delay of over one and a half years (19mo) from the time of initial symptomatic presentation to making the diagnosis in a high percentage (94%) of patients indicates that PAIS is usually not on the radar of physicians treating ankle pain in the pediatric and adolescent population.
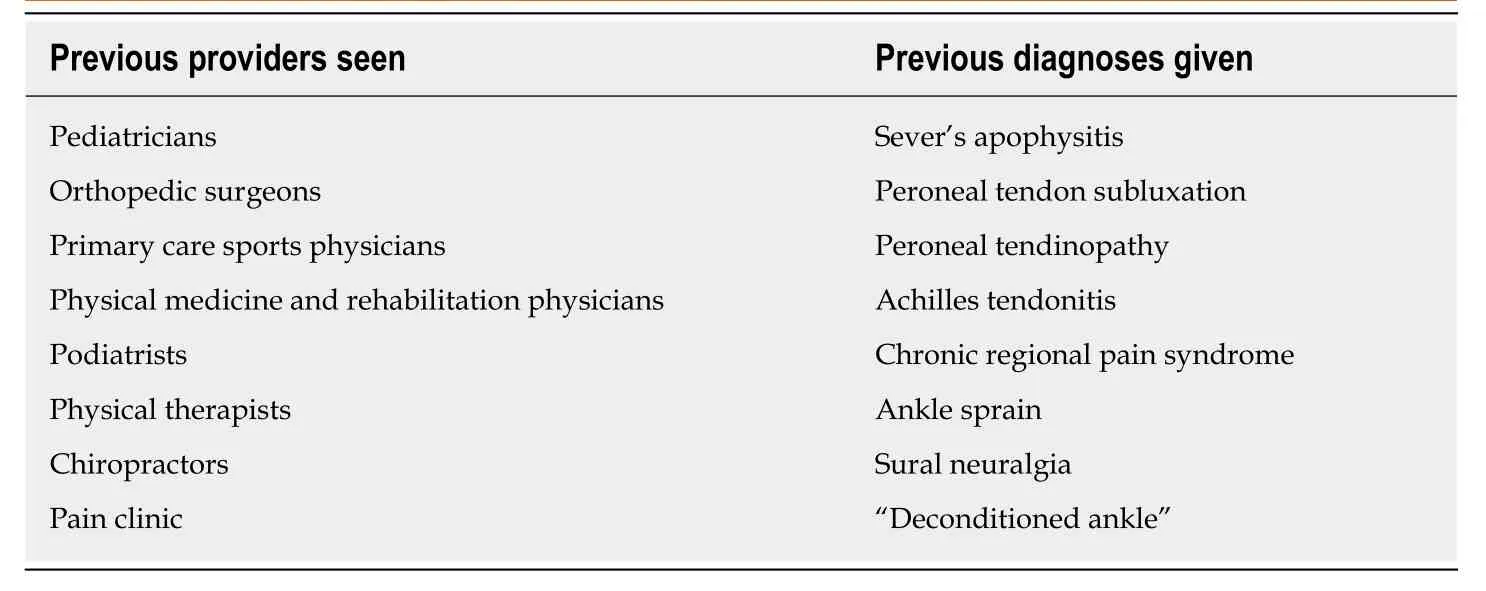
Table1 Spectrum of providers seen and list of prior diagnoses before the diagnosis of posterior ankle impingement syndrome was assigned
The diagnosis of PAIS is primarily based on an accurate history and clinical examination[1-3]. The classic etiologic activities that have been described are dance(especially ballet), soccer, downhill running, and additional forced plantar-flexion activities[1-4]. The pain is aggravated by the aforementioned activities and is typically relieved by rest. The ankle pain is described as consistent, sharp, dull and deep; it is usually difficult for patients to indicate the exact location of the pain in the hindfoot[10,11]. On examination there is posterior joint line tenderness, and more specifically it is typically between the Achilles and peroneal tendons[2,4], which is important to help differentiate it from other causes of posterior foot and ankle pain such as Sever’s apophysitis and ankle sprain. The clinical exam finding of posterior joint line tenderness was seen in all of the ankles in our study; we suggest that this examination should be included in the evaluation of all patients presenting with ankle pain so that the diagnosis of posterior ankle impingement is not missed. A diagnostic local infiltration may also be performed to confirm the diagnosis, which can be guided by ultrasound[2].
History and clinical examination are most important in diagnosing PAIS and they can be supported by imaging findings. Standard lateral plain radiographs can identify bony pathology in the form of os trigonum (Figure1) or Stieda process[12]. However, in young patients with open physes, os trigonum can very well be small or cartilaginous[4]and radiographs could often be reported as “normal”. Entrapment,hypertrophy and inflammation of soft tissues, FHL are common pathologies seen in posterior ankle impingement, but the fact that these are not well-visualized on radiographs can lead to delay in treatment and more expensive imaging[13]. Many of our patients had multiple radiographic imaging procedures performed of the painful ankle; and normal reported radiographs which likely contributed to the delayed diagnosis of PAIS. MRI is considered a useful diagnostic modality for assessment of the pathology in ankle impingement[6,14]. However, MRI has been shown to be an insensitive modality for ankle imaging in the pediatric population[15]. The most common MRI findings in our study included the presence of an os trigonum or Stieda process, with associated osseous and soft tissue edema which is similar to what prior studies in the literature have reported[6,12,14,16].
The most common treatment for posterior ankle impingement is conservative management which includes rest and immobilization of the ankle (with brace/boot/cast) to aid in decreasing the inflammation. This can be supplemented with physical therapy. Corticosteroid injections in the ankle have been described in literature, and are more typically used in athletes to help them complete a season[5].Prolonged conservative treatment for several months was already attempted in all our patients, which lead to temporary pain relief but persisted/recurred with return to activity/sports. Persistent pain with activity despite conservative management was likely the reason why a high percentage (71%) of our patients saw multiple medical providers for treatment. Return of ankle pain with activity is commonly seen in ankle impingement as the pinching of structures in the hindfoot typically occurs with plantar flexion of the ankle causing recurrence of inflammation and pain[3,9,17,18].

Figure1 Fifteen-year old male with posterior ankle pain with os trigonum seen on lateral ankle radiograph.
The indication of arthroscopy in our patient population was persistent symptoms despite prolonged conservative management as mentioned above. Arthroscopic treatment is now an established modality of treatment for patients who fail conservative management[19-21]. Arthroscopic visualization of the ankle and hindfoot during surgery is also a reliable way to confirm the correct diagnosis[22]. Various pathologies which have already been well-described as sources of bony and/or soft tissue causes of posterior ankle impingement were encountered during arthroscopic treatment of our cohort, including os trigonum, Stieda process, hypertrophic ligaments and synovium, cysts of the FHL, and a low-lying FHL muscle belly[2,6,16,18,22-24]. The pain relief after treatment as indicated by improvement in VAS and AOFAS scores, along with return to prior level of sports and activity in our patient cohort supports the clinical diagnosis of posterior ankle impingement.
Weaknesses of our study include data collected at a single institution, small sample size, and no comparative non-operative cohort. The patients referred to a tertiary center like ours may not be representative of the whole population, and the referral could possibly increase the delay. The mean follow-up of 13.1 mo is relatively short;however, the focus of this study is on the delay in clinical diagnosis of PAIS, and not on the surgical outcomes. We have included the arthroscopic findings and treatment outcomes primarily to supplement our clinical diagnosis of PAIS. The strength of our study is the prospective nature of data collection and consecutive enrollment of pediatric patients, both of which help minimize biases that could result from a retrospective study. Collecting long-term multi-center data and including nonoperatively treated patients for comparison are recommended for future studies. To conclude, posterior ankle impingement syndrome can be misdiagnosed in young patients presenting with posterior ankle pain, thus leading to a delay in diagnosis.This prospective study in the pediatric population is the first study which highlights the need for increased awareness about this condition and its clinical diagnosis amongst pediatric orthopedic surgeons, pediatricians, primary care sports doctors,and other physicians involved in treating young athletes to avoid delay in treatment.

Figure2 Magnetic resonance imaging-sagittal image demonstrating edema-like signal intensity adjacent to the os trigonum in the previously mentioned 15-year-old patient in Figure1.

Figure3 Arthroscopic appearance of the os trigonum of the same patient in Figures 1 and 2 before excision.
ARTICLE HIGHLIGHTS
Research background
Posterior ankle impingement is a known cause of ankle pain which has been well described in adults but not as much in the pediatric literature.
Research motivation
The diagnosis of posterior ankle impingement syndrome (PAIS) is made based on detailed history and clinical findings. We came across patients with missed diagnosis of PAIS in clinic and realized that without adequate awareness, this diagnosis can possibly be missed in pediatric and adolescent patients.
Research objectives
The purpose of our study was to identify and characterize the delay in making the diagnosis of PAIS in the young patient population.
Research methods
We started a prospective study to enroll patients under 18 years of age who were diagnosed with PAIS and underwent arthroscopic treatment after failed conservative management. Data collection was done to try and identify any delay in making this diagnosis by the previous treating medical providers. Pre and post treatment pain and American Orthopedic Foot Ankle Society (AOFAS) scores were also noted and compared.
Research results
35 patients (46 ankles) with average age of 13 years had an average 19 mo (range 0-60 mo) delay in diagnosis from initial presentation to a medical provider. 25 (71%) patients had previously seen multiple medical providers. All 46 (100%) ankles had tenderness to palpation over the posterior ankle joint. Radiographs were reported normal in 31/42 (72%) exams. In 32 ankles who underwent MRI, the most common findings included os trigonum (47%)/Stieda process (47%).At an average follow-up of 13.1 mo after treatment, there was significant improvement of VAS(pre-op 7.0 to post-op 1.2) and AOFAS scores (pre-op 65.1 to post-op 93.4) (P< 0.001).
Research conclusions
The study concludes that PAIS is a misdiagnosed condition in the pediatric population.
It was shown that a variety of medical providers (pediatricians, orthopedic surgeons, sports physicians,etc.) missed this diagnosis. There needs to be increased awareness about this condition among medical providers treating young patients.
Research perspectives
The study makes us aware about the delayed diagnosis if PAIS which can be prevented by detailed history taking and examination. This research can be potentially improved in the future by collecting multi-center data to include larger cohort of patients.
杂志排行

World Journal of Orthopedics的其它文章
- Two-stage revision arthroplasty for coagulase-negative staphylococcal periprosthetic joint infection of the hip and knee
- Advanced septic arthritis of the shoulder treated by a two-stage arthroplasty
- Low-velocity simultaneous bilateral femoral neck fracture following long-term antiepileptic therapy: A case report