Soluble mannose receptor as a predictor of prognosis of hepatitis B virus-related acute-on-chronic liver failure
2019-10-19TaiPingLiShiHeGuanQinWangLiWenChenKaiYangHaoZhang
Tai-Ping Li, Shi-He Guan, Qin Wang, Li-Wen Chen, Kai Yang, Hao Zhang
Abstract BACKGROUND Hepatitis B virus-related acute-on-chronic liver failure (HBV-ACLF) is a syndrome with a high short-term mortality rate, and it is crucial to identify those patients at a high mortality risk clinically.AIM To investigate the clinical value of soluble mannose receptor (sMR) in predicting the 90-day mortality of HBV-ACLF patients.METHODS A total of 43 patients were diagnosed with HBV-ACLF between October 2017 and October 2018 at the Second Hospital of Anhui Medical University, and all of them were enrolled in this retrospective study. Their serum sMR levels were determined using an enzyme-linked immunosorbent assay. Demographic and clinical data, including gender, age, albumin level, total bilirubin (TBIL) level,international normalized ratio, HBV-DNA level, HBV serological markers,procalcitonin level, interleukin-6 level, and model for end-stage liver disease(MELD) score were accessed at the time of diagnosis of HBV-ACLF. A multivariate logistic regression analysis was used to analyze the independent risk factors for mortality.RESULTS Serum sMR level was significantly increased in HBV-ACLF patients compared with chronic hepatitis B patients and healthy controls (P < 0.01). When compared with surviving patients, it was higher in those patients who succumbed to HBVACLF (P < 0.05). Serum sMR level was positively correlated with MELD score (rs= 0.533, P = 0.001), HBV-DNA level (rs = 0.497, P = 0.022), and TBIL level (rs =0.894, P < 0.001). Serum sMR level (odds ratio = 1.007, 95% confidence interval:1.004-1.012, P = 0.001) was an independent risk factor for the 90-day mortality in the HBV-ACLF cases. The patients with HBV-ACLF were stratified into two groups in accordance with their serum sMR levels at the baseline (low risk: <99.84 pg/mL and high risk: ≥ 99.84 pg/mL). The 90-day mortality rates were 27.3% in the low-risk group and 87.5% in the high-risk group. Furthermore, sMR level apparently improved the performance of MELD score for predicting the prognosis of patients with HBV-ACLF.CONCLUSION Serum sMR level may be a predictor of the prognosis of HBV-ACLF patients.
Key words: Acute-on-chronic liver failure; Mannose receptor; Model for end-stage liver disease; Prognosis; Risk factor
INTRODUCTION
Acute-on-chronic liver failure (ACLF) is a clinical syndrome of the acute decompensation of liver function based on chronic liver disease, and it is often accompanied by multiple organ failure[1]. The main cause of ACLF is the acute exacerbation of chronic hepatitis B (CHB), which accounts for more than 80% of all causes in China[2]. ACLF caused by CHB is called hepatitis B-related ACLF (HBVACLF).
The pathogenesis of HBV-ACLF is related to the activation of hepatic macrophages[3]. Macrophages can be rapidly activated under the stimulation of acute and chronic inflammatory reactions, and they are differentiated into Ml and M2 macrophages[4]. Mannose receptor (MR) is expressed mainly on the membrane surfaces of M2 macrophages and dendritic cells[5]. MR can recognize and bind specific carbohydrate molecules through the extracellular domain, which plays an important role in identifying pathogens, presenting antigens, and maintaining the homeostasis of the internal environment[6]. Its soluble form, soluble mannose receptor (sMR), is formed by the matrix metalloproteinase cleavage of MR on the cell membrane, and it is secreted into peripheral serum[7]. Serum sMR level is elevated in critical illnesses,including severe liver disease[8]. In addition, sMR level is associated with liver disease severity in patients with alcoholic hepatitis and chronic viral hepatitis[9-11].
Previous studies have shown that sMR levels gradually increase with ACLF severity, and they are closely related to mortality[12]. Nevertheless, the role of sMR in HBV-ACLF has not been elucidated. Therefore, this research was designed to assess the value of sMR level in predicting the 90-day mortality of HBV-ACLF patients.
MATERIALS AND METHODS
Patients
Forty-three patients with HBV-ACLF and 43 patients with CHB from the Second Hospital of Anhui Medical University were enrolled in this study from October 2017 to October 2018. In addition, 20 healthy controls (HCs) were randomly selected during this time period. The diagnosis of HBV-ACLF was based on the consensus definition of the Asian Pacific Association for the Study of the Liver (2014 version)[13],as follows: Acute hepatic insult manifested as jaundice (serum bilirubin ≥ 5 mg/dL or 85 µmol/L) and coagulopathy [international normalized ratio (INR) > 1.5 or prothrombin activity < 40%], complicated within 4 wk by ascites and/or encephalopathy in a patient with CHB. According to the INR level, they were divided into three subgroups: Early stage (1.5 < INR ≤ 1.9), medium stage (1.9 < INR ≤ 2.6),and late stage (INR ≥ 2.6). Patients with liver failure caused by cirrhosis, other hepatitis virus infections or coinfections, alcoholic liver disease or nonalcoholic fatty liver, or hepatotoxic drugs were excluded from this research. CHB diagnosis was made according to the diagnostic criteria of the Chinese guidelines for the prevention and treatment of CHB (2015 version)[14]. Blood samples (5 mL) were collected at the time of HBV-ACLF or CHB diagnosis, and they were centrifuged at 1000 × g for 15 min and then stored at -80 °C. Demographic and clinical data, including gender, age,albumin (ALB) level, total bilirubin (TBIL) level, INR, HBV-DNA level, HBV serological markers, procalcitonin (PCT) level, and interleukin-6 (IL-6) level, were collected within the first day after HBV-ACLF diagnosis. We followed the patients with HBV-ACLF who met the inclusion criteria: The patients who survived within 90 d made up a survival group, and those who died within 90 d made up a non-survival group (including automatic discharge due to exacerbation).
According to the 1975 Helsinki Declaration, this study was approved by the Ethics Committee of the Second Hospital of Anhui Medical University. Written informed consent was obtained from all of the participants prior to their inclusion in this study.
Serological sMR detection
Serum concentrations of sMR were measured using a commercial enzyme-linked immunosorbent assay (ELISA) kit (GTX, Inc., Los Angeles, CA, United States) in accordance with the instructions. Briefly, we added 50 µL of diluted (1:5) serum samples to the ELISA plates that were pre-coated with a captured sMR antibody, and the absorbance was measured at 450 nm by using an ELISA plate reader (ST-360;Shanghai Kehua Bio-engineering, Ltd., Shanghai, China). A duplicate assay was also performed. The concentration of the standard was set to the abscissa, and the absorbance value was set to the ordinate. A standard curve was drawn, and the absorbance value was substituted into the linear equation in order to calculate the sample concentration.
Scoring system
The model for end-stage liver disease (MELD) score was calculated using the formula as follows: MELD = 11.2 × ln (INR) + 9.6 × ln [creatinine (Cr, mg/dL)] + 3.8 × ln [TBIL(mg/dL)] + 6.4.
Statistical analysis
All of the data were analyzed using IBM SPSS Statistics for Windows version 22.0(IBM Corp., Armonk, NY, United States). The normally distributed data are expressed as the mean ± standard deviation, and the non-normally distributed data are expressed as the median (interquartile range). The differences in the normally distributed data were analyzed using the Student’st-test and analysis of variance. The comparisons of the non-normally distributed data were performed using the Mann-Whitney U test and the Kruskal-Wallis test. Spearman correlation analysis was used to evaluate the correlations between the sMR level and other clinical indicators.Multivariate logistic regression was employed to analyze the independent risk factors for mortality. The best sMR cutoff value for predicting the 90-day mortality was determined by adopting SPSS Modeler 18.0 software (IBM Corp., Armonk, NY,United States). The area under the receiver operating characteristics curve (AUROC)was used to compare the accuracy of the prediction. Survival analysis was performed using the Kaplan-Meier curve. A two-sidedP-value < 0.05 was considered to indicate a statistically significant difference.
RESULTS
Subject characteristics
The demographic and clinical characteristics of all of the subjects in the ACLF, CHB,and HC groups are listed in Table 1. There were no significant differences in the age or sex ratio between the three groups (P> 0.05). The patients with HBV-ACLF had elevated ALB, TBIL, Cr, INR, PCT, IL-6, and HBV-DNA levels when compared with the other two groups (P< 0.05). MELD score was significantly elevated in the HBVACLF patients when compared with CHB patients (P< 0.05). Out of the HBV-ACLF patients, there were 12 patients in the survival group and 31 in the non-survival group. The number of patients with HBV-ACLF in the early stage, medium stage, and late stage groups was 12, 10, and 21, respectively.
Serum sMR expression in HBV-ACLF patients
Serum sMR levels of HBV-ACLF patients, CHB patients, and HCs were 114.94 ± 49.65 pg/mL, 80.75 ± 34.45 pg/mL, and 26.51 ± 8.62 pg/mL, respectively. Serum sMR level of HBV-ACLF patients was significantly higher than those of CHB patients and HCs(P< 0.01; Figure 1A). Serum sMR levels in the early, medium, and late stage groups of HBV-ACLF patients increased gradually (79.42 ± 25.10 pg/mL, 113.56 ± 14.35 pg/mL,and 158.15 ± 59.13 pg/mL, respectively) (P< 0.01; Figure 1B).
Serum sMR levels help to differentiate between survivors and non-survivors
Serum sMR level of non-survivors was significantly increased (131.20 ± 9.40 pg/mL),and it was much higher than that of the survival group (69.89 ± 6.92 pg/mL) (P< 0.05;Figure 2).
Correlations between sMR level and liver injury indicators
To further explore the clinical value of sMR level in developing HBV-ACLF, we analyzed the correlations between serum sMR level and liver injury parameters,including MELD score, HBV-DNA level, and TBIL level. Serum sMR level was positively correlated with MELD score (rs= 0.533,P= 0.001), HBV-DNA level (rs=0.497,P= 0.022), and TBIL level (rs= 0.894,P< 0.001) (Figure 3A-C).
Serum sMR level is an independent risk factor for mortality in HBV-ACLF patients
To determine the potential of serum sMR level to predict the prognosis of HBV-ACLF,univariate and multivariate logistic regression analyses were employed to test the following parameters (see Table 2). MELD score was calculated using the TBIL, Cr,and INR, so these three values were not used in the logistic regression. The multivariate analysis indicated that MELD score [odds ratio (OR) = 1.132, 95%confidence interval (CI): 1.046-1.396,P= 0.001] and sMR level (OR = 1.007, 95%CI:1.004-1.012,P= 0.001) were independent risk factors for the 90-day mortality (Table 2).
Serum sMR level apparently improves performance of MELD score for predicting prognosis of HBV-ACLF patients
Patients with HBV-ACLF were stratified into two groups in accordance with the cutoff value of serum sMR level. The best cutoff value of sMR level was identified using SPSS Modeler 18.0 software (low risk: < 99.84 pg/mL and high risk: ≥ 99.84 pg/mL). The 90-day mortality rates were 27.3% (3/11) for the low-risk group and 87.5% (28/32) for the high-risk group k, and patients with sMR levels ≥ 99.84 pg/mL had poor prognoses (Figure 4). When the optimal cut-off value was 99.84 pg/mL, the sensitivity and specificity of sMR level for predicting the 90-day mortality were 70.6%and 83.3%, respectively. In addition, compared with the single MELD score, the new prognostic model combining MELD with sMR showed a significant advantage in terms of prognostic accuracy (AUROC = 0.903 and 0.717, respectively,P= 0.025)(Figure 5).
DISCUSSION
Our study demonstrated that serum sMR levels in patients with HBV-ACLF were increased significantly, and they helped to distinguish the survivors from nonsurvivors. Serum sMR level was positively correlated with MELD score and HBVDNA and TBIL levels. In addition, the results of this study showed that serum sMR level was an independent risk factor for the prognosis of HBV-ACLF.
As described previously, HBV-ACLF refers to liver failure caused by the acute aggravation of liver injury in CHB patients[1,2]. At present, the pathogenesis of the disease has not been fully clarified, but most researchers believe that immune damage plays a key role in HBV-ACLF. Immunocytes, such as macrophages, are activated in the pathogenesis of HBV-ACLF; they release a large number of inflammatory mediators and cytokines which participate in the inflammatory response of the liver.The expression level of the macrophages is closely related to the development and prognosis of the disease[3,15]. As a macrophage activation marker, MR mediates a series of immune responses that recognize, phagocytose, and clear pathogens[6]. The serum containing sMR can be stored at - 80 °C for 20 mo, and it can be detected by ELISA[8].
This study found that compared with HCs and CHB patients, the expression level of sMR in serum of HBV-ACLF patients was significantly increased. Moreover,sCD163, a marker of macrophage activation, is also significantly elevated in patients with HBV-ACLF[3]. Therefore, we speculate that sMR and sCD163 may play important roles in the immune process of acute liver inflammation. Laursen et al[11]found that the macrophage activation markers sCD163 and sMR were associated with activity and fibrosis in the liver biopsies of patients with CHB. At the same time, we found that the sMR level of CHB patients was significantly higher than that of HCs,suggesting that sMR may also play an important role in the pathogenesis of CHB. We also analyzed the sMR levels in the early, middle, and late stages of HBV-ACLF. The results showed that the sMR expression level increased gradually with the increase in the severity of the disease, indicating that sMR level is closely related to disease severity in HBV-ACLF patients.
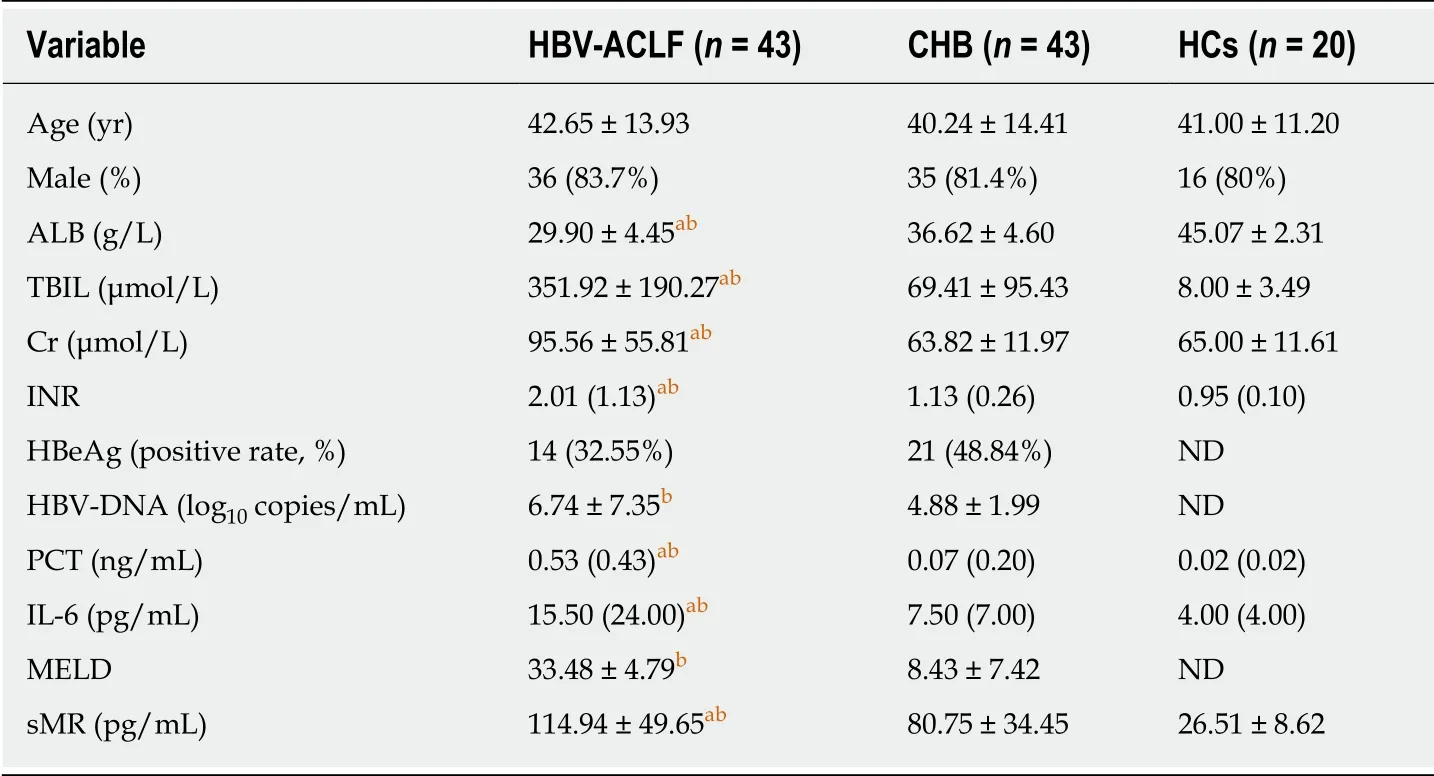
Table 1 Demographic and clinical characteristics of the study subjects
MELD score has been used widely to evaluate the prognosis of HBV-ACLF.Through a correlation analysis, we found that sMR level was positively correlated with MELD score, HBV-DNA level, and TBIL level. When combined with the previous experimental results, we concluded that sMR level was closely related to liver inflammatory injury and disease severity in patients with HBV-ACLF. Previous studies have indicated that sMR may be a potential biomarker for liver diseases and infectious diseases[8]. Moreover, Japanese scholars have found that serum sCD206 was increased in pulmonary tuberculosis (PTB), and that it was associated with the prognosis; therefore, it could be a potential biomarker for PTB[16]. Relster et al showed that the macrophage activation marker sMR holds potential as a new diagnostic and early prognostic biomarker for patients with acute infectious diseases, with or without sepsis[17]. In order to verify whether sMR level could be a predictor of HBV-ACLF prognosis, a multivariate logistic regression analysis was performed, and the results showed that sMR level was an independent risk factor for mortality in HBV-ACLF patients. In addition, it apparently improved the performance of MELD score for predicting HBV-ACLF prognosis.
Our study did have some limitations. First of all, serum sMR level was obviously correlated with HBV-ACLF prognosis, but the mechanisms underlying the role of sMR were not investigated. Second, the dynamic changes in serum sMR should be determined during the progression of HBV-ACLF. Finally, multicenter studies with large sample sizes are also required to confirm the current findings.
In conclusion, serum sMR level is significantly elevated in HBV-ACLF patients, and it is apparently associated with indicators of liver injury and disease severity. In addition, sMR level is an independent risk factor for the prognosis of HBV-ACLF. The present findings collectively suggest that sMR level may be a predictor of the prognosis in patients with HBV-ACLF.
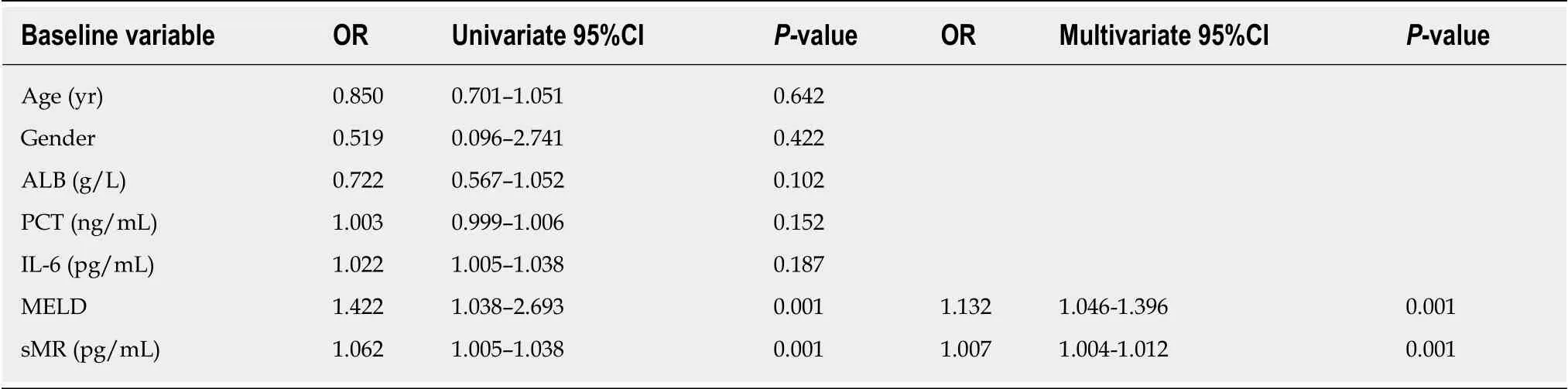
Table 2 Risk factors for 90-d mortality in patients with hepatitis B virus-related acute-on-chronic liver failure
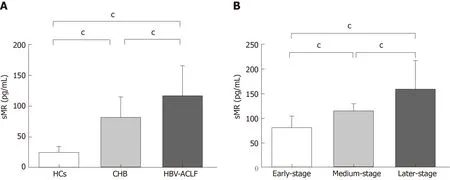
Figure 1 Serum soluble mannose receptor levels in different groups of subjects.

Figure 2 Comparison of soluble mannose receptor levels between non-survivors and survivors.
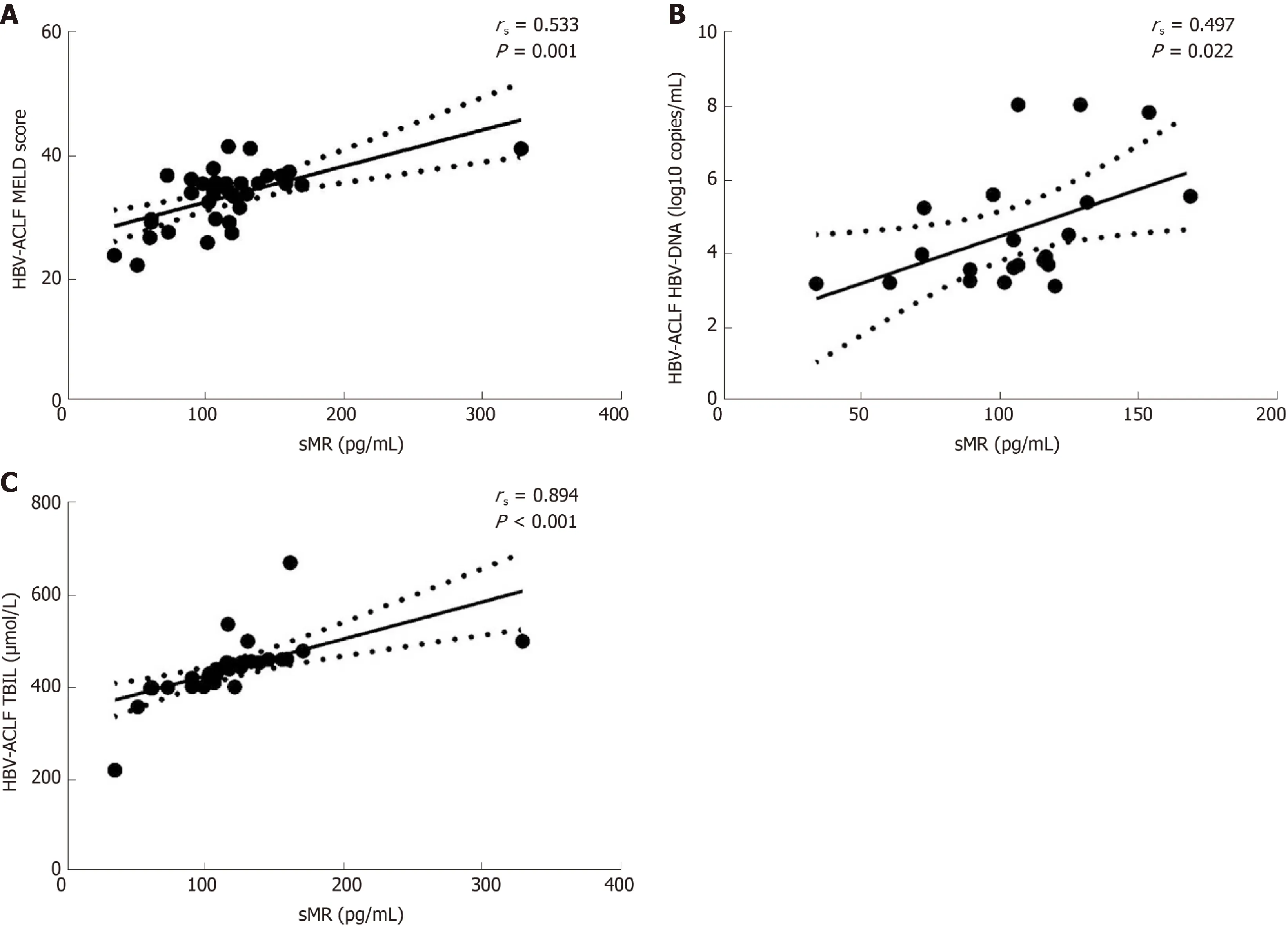
Figure 3 Correlations between serum soluble mannose receptor level and liver injury parameters.
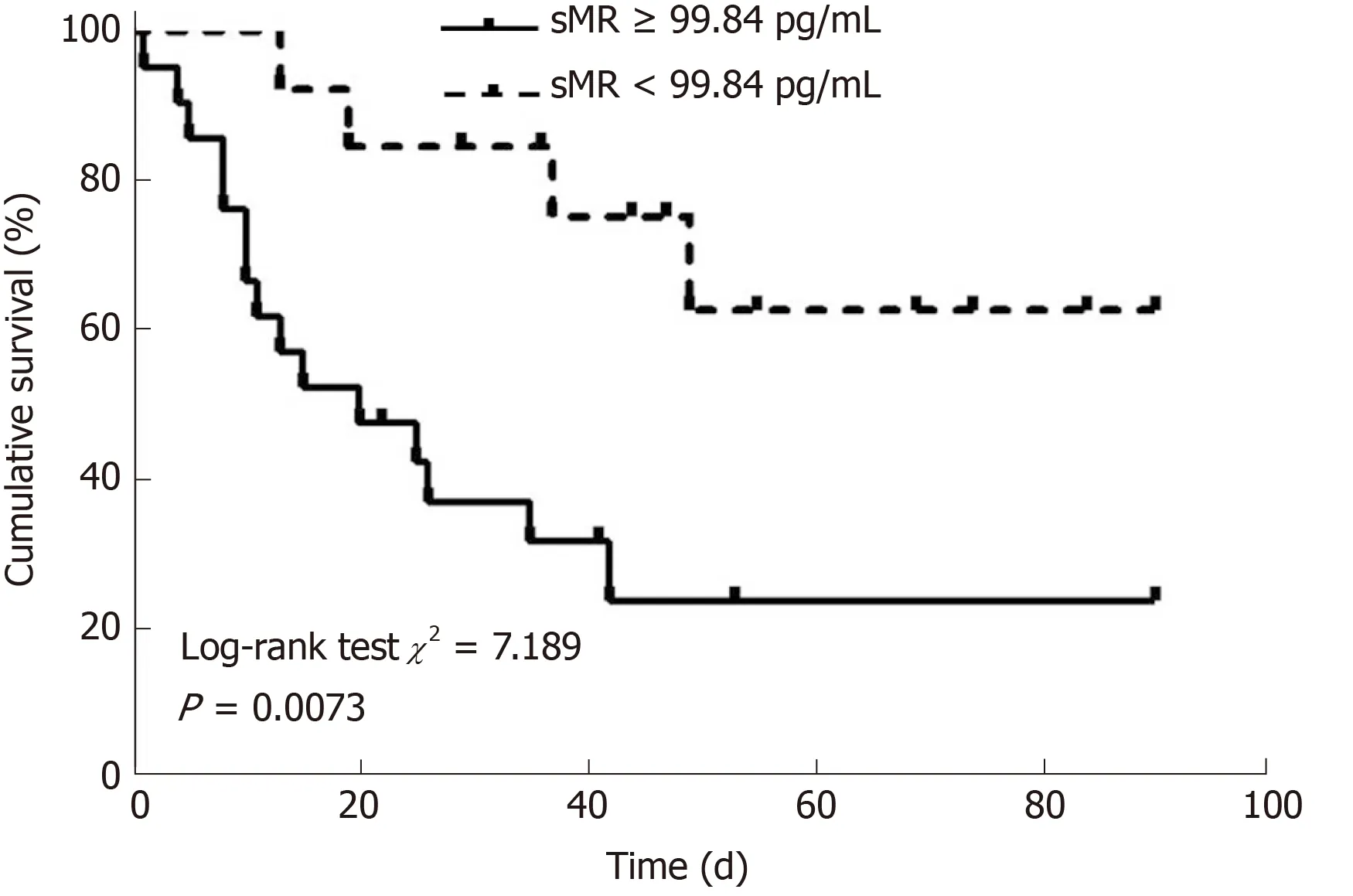
Figure 4 Kaplan-Meier survival curves of soluble mannose receptor levels for predicting 90-day mortality.
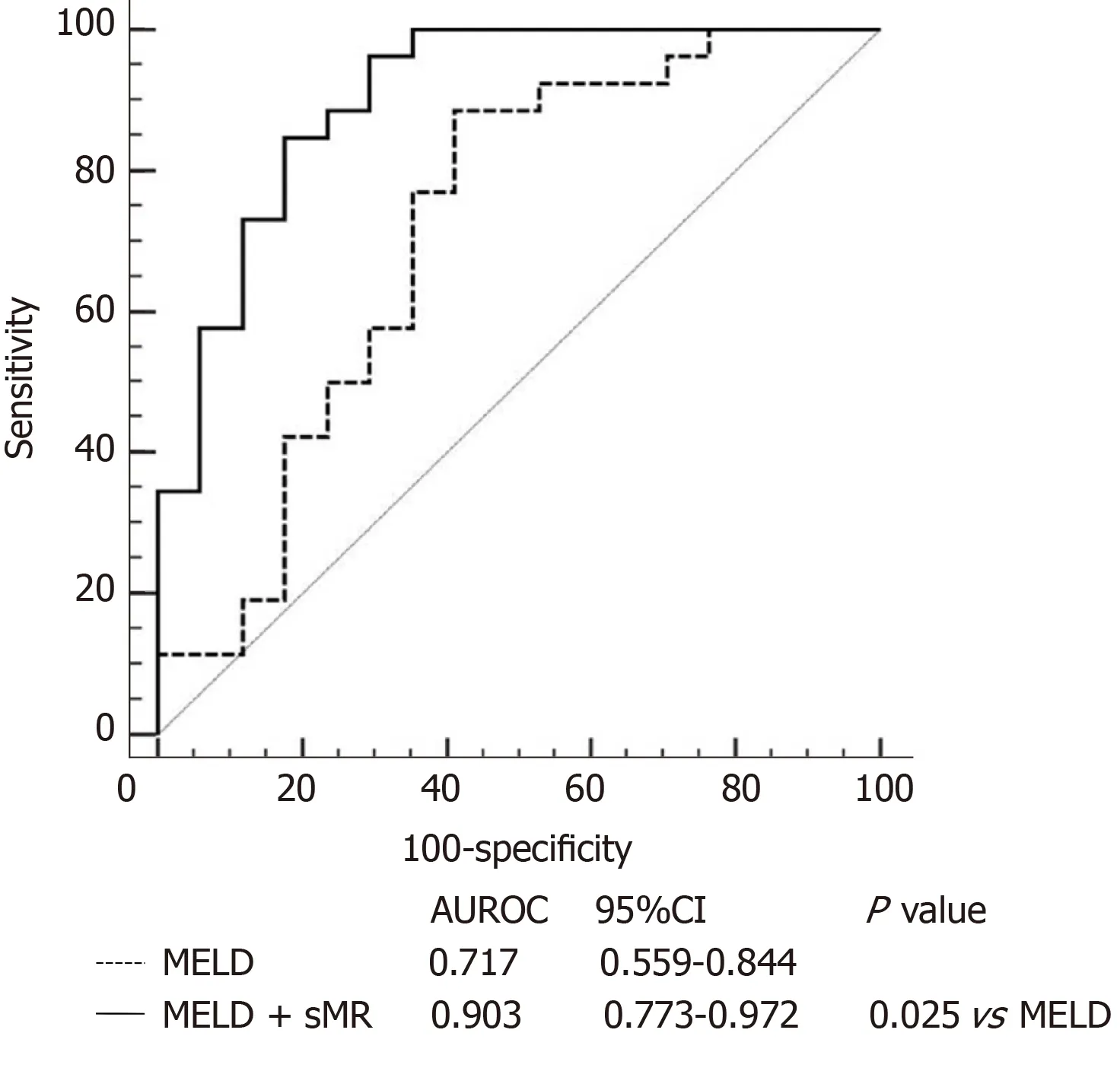
Figure 5 Areas under the receiver operating characteristics curves of model for end-stage liver disease score alone and model for end-stage liver disease score plus serum soluble mannose receptor. AUROC: Area under the receiver operating characteristics curve; CI: Confidence interval; MELD: Model for end-stage liver disease; sMR: Soluble mannose receptor.
ARTICLE HIGHLIGHTS
杂志排行

World Journal of Gastroenterology的其它文章
- Pathogenesis and clinical management of Helicobacter pylori gastric infection
- Oncogenic ADAM28 induces gemcitabine resistance and predicts a poor prognosis in pancreatic cancer
- Correlation of plasma miR-21 and miR-93 with radiotherapy and chemotherapy efficacy and prognosis in patients with esophageal squamous cell carcinoma
- Accuracy of an administrative database for pancreatic cancer by international classification of disease 10th codes: A retrospective large-cohort study
- Post-transplant infection improves outcome of hepatocellular carcinoma patients after orthotopic liver transplantation
- Short-term efficacy of robotic and laparoscopic spleen-preserving splenic hilar lymphadenectomy via Huang's three-step maneuver for advanced upper gastric cancer: Results from a propensity score-matched study