Feasibility of endoscopic treatment and predictors of lymph node metastasis in early gastric cancer
2019-10-11YuNingChuYaNanYuXueJingTaoMaoYunQingChenXiaoBinZhouWenSongXianZhiZhaoZiBinTian
Yu-Ning Chu, Ya-Nan Yu, Xue Jing, Tao Mao, Yun-Qing Chen, Xiao-Bin Zhou, Wen Song, Xian-Zhi Zhao,Zi-Bin Tian
Abstract
Key words: Early gastric cancer; Lymph node metastasis; Predictors; Endoscopic submucosal dissection; Expanded indications
INTRODUCTION
Gastric cancer is currently the fifth most common cancer and the third leading cause of cancer-related death worldwide[1]. Early gastric cancer (EGC) is defined as a tumor that is confined to the mucosa and submucosa of the stomach, irrespective of regional lymph node metastasis (LNM)[2]. Several studies have reported a frequency of LNM ranging from 5%-10% among EGC patients undergoing radical surgery[3], suggesting that over 90% of surgeries could potentially be avoided if curative endoscopic resection (ER) is accurately predicted based on the histopathology of an endoscopicresected specimen.
Endoscopic submucosal dissection (ESD) has notable advantages over conventional surgical resection, as it causes less trauma, minor bleeding, and fewer postoperative complications[4]. The absolute indications for ESD for curative resection in EGC that were proposed by the Japanese Gastric Cancer Association (JGCA) initially include nonulcerated, well-differentiated mucosal lesions ≤ 2 cm in diameter[5]. The absolute indications for ESD, however, are so strict that unnecessary surgeries may be performed. Subsequently, the expanded indications for ESD, which include larger,ulcerated, and undifferentiated mucosal lesions as well as differentiated lesions with slight submucosal invasion, were proposed. A recent meta-analysis involving 12 studies revealed that the incidence of LNM was only 0.2% among patients who met the absolute indications, compared with an LNM incidence of 0.7% among patients who met the expanded indications[6]. Furthermore, several studies have shown that LNM is closely related to an unsatisfactory prognosis in EGC[7-10].
To date, universal preoperative examination methods, such as gastroscopy,endoscopic ultrasonography, computed tomography, and X rays, fail to provide adequate data on the lesion and regional lymph node status before surgery or ER[11].However, evaluating the risk of LNM is critical for determining the best course of management for EGC patients[12]. Unfortunately, the risk factors that have been identified in different studies are diverse, and controversy still exists regarding the expanded indications for ESD. Therefore, in this study, which involved a relatively large number of EGC patients, we aimed to reevaluate and verify the current guidelines for endoscopic treatment of EGC in a Chinese population and to investigate the predictors of EGC with LNM.
MATERIALS AND METHODS
Patients
We retrospectively reviewed all patients who were diagnosed with gastric cancer and underwent gastrectomy with lymphadenectomy between June 2007 and December 2018 at the Affiliated Hospital of Qingdao University. This study was performed in accordance with the Declaration of Helsinki (2000) of the World Medical Association.Our study was also approved by the Institutional Review Board of the Ethics Committee of the Affiliated Hospital of Qingdao University (QYFY WZLL 2019-04-04). In all, 12552 patients were reviewed. Patients were excluded if they had: (1)Advanced-stage gastric cancer (n = 11099); (2) Intestinal metaplasia or intraepithelial neoplasia (n = 72); (3) Metastatic gastric cancer or multiple carcinomas (n = 38); (4)Lymphoma (n = 28); (5) Gastric stump carcinoma (n = 36); and (6) Other lifethreatening diseases (n = 17). Ultimately, 1262 EGC patients were enrolled in this study.
Data collection
The included patients underwent gastrectomy with lymph node dissection. All operations were performed according to the 4th edition of the JGCA treatment guidelines[5]. The specimens were serially sectioned into 3-mm-thick slices, and two experienced pathologists individually examined the histological slides immediately after resection. The diagnostic criterion for LNM is the presence of cancerous tissue inside the lymph node capsule, as shown in Figures 1 and 2. We collected the clinical data, endoscopic features, and pathological characteristics of all enrolled patients.These data included age, sex, incidence of hypertension, heart disease and diabetes mellitus, drinking and smoking history, body mass index (BMI), family history,carcinoembryonic antigen (CEA) level, tumor location, lesion size, macroscopic type,depth of invasion, number of tumors, presence of ulcers, tumor differentiation,Lauren type, presence of lymphovascular invasion (LVI), perineural invasion, and LNM.
Based on the distribution of gastric glands, we classified the tumor locations as cardia, fundus/corpora, or angle/antrum. According to the Paris endoscopic classification, the macroscopic features of EGC were divided into the following five subtypes: Type 0-I (protruded), type 0-IIa (superficial elevated), type 0-IIb (flat), type 0-IIc (superficial depressed), and type 0-III (excavated)[13]. Tumors were also graded as small (≤ 20 mm), medium (20-30 mm), and large (≥ 30 mm) to further analyze the indications for ESD. For invasion depth, submucosal lesions were classified into two groups: SM1 (≤ 500 μm depth of invasion) and SM2 (> 500 μm depth of invasion). In accordance with the JGCA, when multiple lesions were present, the tumor with the most advanced T category (or the largest lesion when the T stages were identical) was classified[2].
Statistical analysis
Statistical analyses were conducted with SPSS software (SPSS, version 23.0, Chicago,IL, United States). Continuous variables, such as age and BMI, were translated into categorical variables. For age, we calculated the mean value (59.25 years) of the patients and set 60 years as the cut-off value. According to the criteria for obesity, the enrolled patients were divided into a nonobesity group (BMI < 28) and an obesity group (BMI ≥ 28). Differences among categorical variables associated with predictors and LNM were assessed using a chi-square test or Fisher’s exact test, and variables that were significant in the univariate analysis were subsequently entered into a multivariate logistic regression model for analysis of independent risk factors for LNM in EGC. The association between variables and LNM was described by an odds ratio (OR) and a 95% confidence interval (CI). P < 0.05 (two-sided) was considered statistically significant.
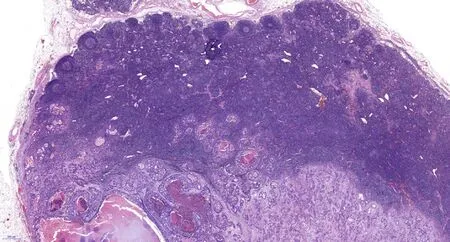
Figure 1 Pathological image of lymph node metastasis (20×).
The statistical methods and analyses of this study were reviewed by professor Xiao-Bin Zhou from the Department of Health Statistics, Qingdao University.
严重药品不良反应/事件(adverse drug reaction/event,ADR/ADE)对人体损伤严重,是不良反应监测工作的重点,也是衡量报告可利用度的重要指标之一[1‐2]。因此,及时发现、处理和分析严重 ADR/ADE并对其进行后续的分析,对不良反应信号的发掘,促进监测工作的开展和临床合理用药具有重要意义。为此,本文对南京市药品不良反应监测中心2017年接收的严重ADR/ADE报告进行统计分析,全面了解南京地区发生严重ADR/ADE的规律和特点,并探讨可能存在的影响因素,为药品不良反应监测工作的开展和临床合理用药提供参考依据。
RESULTS
Clinical characteristics
We assessed 12552 patients who underwent radical gastrectomy with lymph node dissection. A total of 1262 (10.1%) eligible EGC patients with LNM (n = 182) and without LNM (n = 1080) were included in this study. The sex distribution was 899(71.2%) males and 363 (28.8%) females (ratio: 2.48:1), with an average age of 59.25 years (range, 24-90 years). Data on the clinical characteristics are shown in Table 1.Patients with a CEA value that exceeded the normal level were more likely to have LNM, and this association was statistically significant (P = 0.007). However, other clinical parameters, such as age, sex, underlying diseases, lifestyle habits, family history, and Helicobacter pylori (H. pylori) infection, failed to reach statistical significance.
Positive LNM results in EGC according to indications for ESD
According to further analysis, no LNM metastasis was observed in patients who met the absolute indications for ESD (0/90). However, LNM occurred in a few patients(4/311) who met the following expanded indications for ESD: (1) Differentiated mucosal tumors, ≤ 30 mm in size, without LVI, and with ulceration (3/86 cases, 3.5%);(2) Differentiated mucosal tumors, without ulcer and LVI, and of any size (1/32 cases,3.1%); (3) Undifferentiated mucosal tumors without ulcer and LVI, and ≤ 20 mm in size (0/110 cases, 0%); and (4) Differentiated tumors with SM1 invasion, no LVI, and ≤30 mm in size (0/83 cases, 0%). As shown in Table 2, patients who met the surgical indications had a higher risk of LNM (P < 0.001). Table 3 contains more details on the frequency of LNM among EGC patients who met the indications for ESD.
Comparison of endoscopic features
The endoscopic features are shown in Table 4. More EGCs were in the angle/antrum of the stomach (n = 928, 73.5%) than in the cardia (n = 46, 3.6%) and in the fundus/corpora (n = 288, 22.8%). Forty-two (3.3%) patients had multifocal lesions.The univariate analysis revealed that the location and number of tumors were not significantly associated with LNM. Regarding tumor size, LNM occurred significantly more frequently in patients with medium (P = 0.016) or large (P = 0.000) tumors than in patients with small tumors. With regard to macroscopic features, type IIc (n = 486,38.5%) occurred most frequently among the five subtypes, but type III (n = 481, 38.1%)occurred more frequently in patients with LNM (P = 0.001). Ulcerative lesions also occurred more frequently in patients with LNM (P = 0.013).
Analysis of histopathological characteristics

Figure 2 Pathological image of lymph node metastasis (200×).
Among the 1262 EGC patients, 182 (14.4%) had LNM according to the pathological diagnostic criteria, including 123 (67.6%) with stage N1, 39 (21.4%) with stage N2, and 20 (11.0%) with stage N3 LNM according to the 8th edition of the American Joint Committee on Cancer (AJCC) Staging Manual. The mean number of metastatic lymph nodes was 2.8 (range, 1-17). Regarding lesion depth, 596 (47.2%) patients had tumors limited to the mucosal (M) layer, whereas 245 had SM1 (superficial submucosal)tumors (19.4%), and 421 had SM2 (deep submucosal) tumors (33.4%). The percentages of lymph node positivity were 5.2%, 19.6%, and 24.5% for M, SM1, and SM2,respectively. In terms of tumor differentiation, the undifferentiated type (n = 807,63.9%) was the major histologic type of EGC based on the JGCA criteria and was significantly more likely to occur in patients with LNM than the differentiated type (n= 455, 36.1%) (P 0.001). Regarding cell histology, the patients with mucinous adenocarcinoma had a higher risk of LNM than patients with other histologic lesion types (P = 0.019). Based on the Lauren classification, LNM was observed more frequently in diffuse-type (DT) and mixed-type (MT) tumors (P = 0.003) than in intestinal-type (IT) tumors. Moreover, LNM was found significantly more frequently in patients with LVI (P 0.001) and perineural invasion (P 0.001) than in the patient subgroup without invasion. Additional detailed histopathologic features of the enrolled patients are summarized in Table 5.
Univariate analysis
The univariate analysis results showed that 10 out of the 20 factors were significantly associated with a higher risk of LNM. The risk factors included high CEA levels,medium and large lesion sizes, excavated macroscopic type, presence of ulcers, deep submucosal invasion (SM1 and SM2), poor differentiation, LVI, mucinous adenocarcinoma, perineural invasion, and diffuse and mixed Lauren classifications.
Multivariate logistic regression analysis of lymph node metastasis
Based on stepwise multivariate analysis, the significant independent risk factors for LNM in EGC were SM1 invasion (OR = 2.285, P = 0.030), SM2 invasion (OR = 3.230, P< 0.001), LVI (OR = 15.702, P < 0.001), pathological pattern of mucinous adenocarcinoma (OR = 2.823, P = 0.015), and lesion size over 30 mm (OR = 1.900, P =0.006). The independent risk factors are listed in Table 6.
DISCUSSION
Following the introduction of the expanded indications for ESD, many studies have reevaluated the risk of LNM in EGC. A meta-analysis involving 9798 EGC patients showed that among the expanded indications for ESD, the inclusion of mucosal differentiated lesions of any size that were not ulcerated and of differentiated mucosal lesions < 30 mm that were ulcerated can be justified with a minimally increased risk.Nonetheless, the reasonableness of expanding the indications for ESD to include undifferentiated lesions smaller than 20 mm and differentiated lesions with slight submucosal invasion still requires careful investigation[6]. Our study demonstrated that the rate of LNM for patients who met the expanded indications for ESD was 4/311 (1.3%). No LNM occurred in patients who met the absolute indications.Similarly, reassessment of the expanded indications in Korea also showed an LNM rate of 2.4% among patients who met the expanded indications[14], which is inconsistent with the results of a large dataset from Japan that revealed no LNM in patients who met the expanded indications[15]. It is difficult to identify the reasons for this difference. A probable interpretation is that the existing indications are still notsufficiently comprehensive. The JGCA added invasion depth, ulceration, tumor size,differentiation, and LVI to its criteria for ESD. Based on our results, it is necessary to take the cellular histology of tumors into consideration when deciding upon the ESD indications. If ESD is performed in a more selective subgroup, the risk of LNM will likely be reduced. Therefore, predictive factors may be used to optimize the ESD criteria.
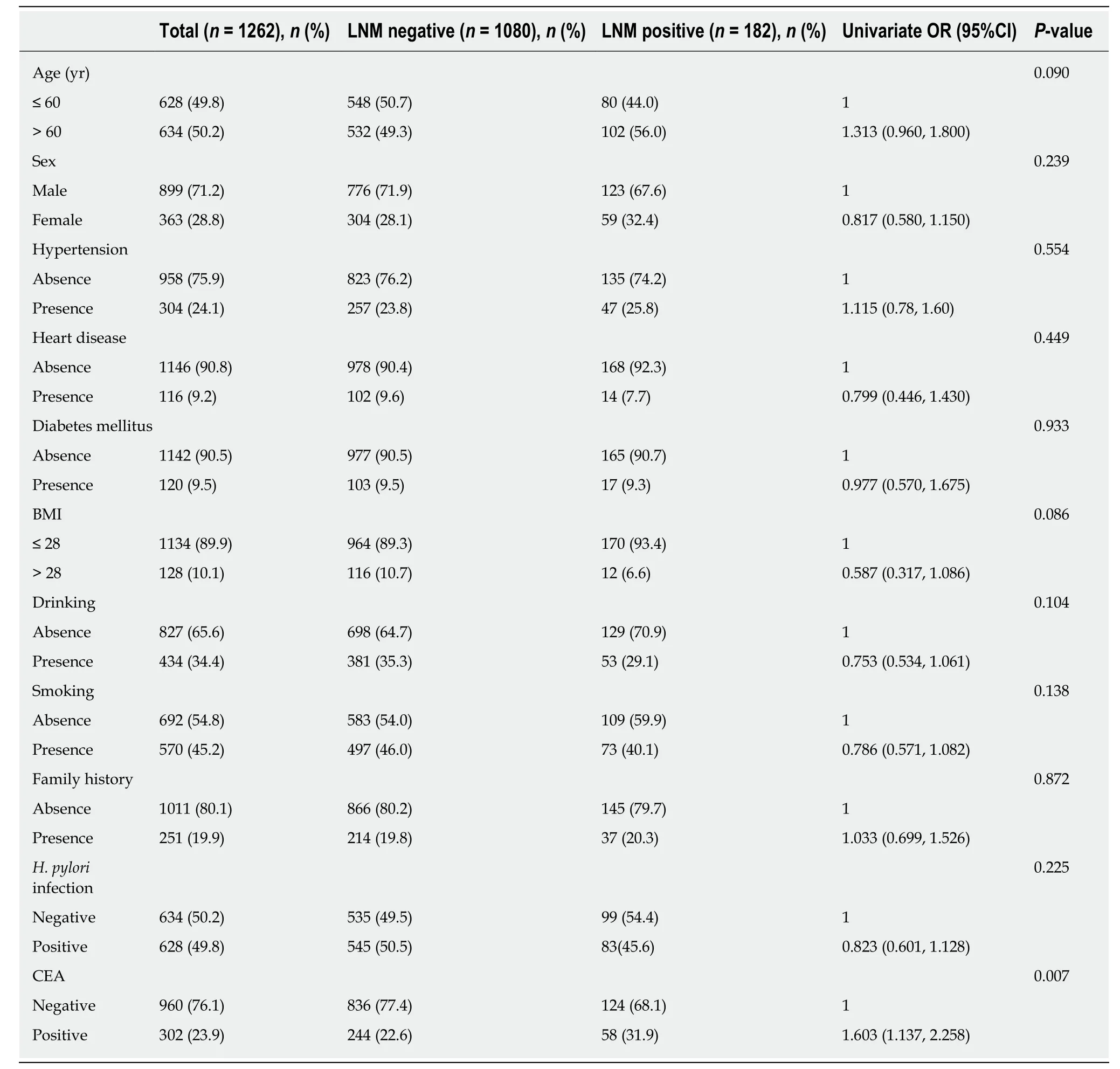
Table 1 Lymph node metastasis risk according to clinical parameters
In line with other relevant studies, our study also concluded that deeper invasion significantly increased LNM risk. Additionally, the measurement of the width of the infiltration could be a useful additional parameter in the indications for supplemental gastrectomy after ESD. Therefore, a detailed measurement of invasion depth is truly necessary during the pathological evaluation of endoscopic-resected specimens[16].Regarding lesion size, we found that larger tumor size was a significant predictor of regional LNM in our patients with EGC, which is similar to the conclusions of many other investigators[7,9,17-19]. However, the cut-off values varied among these studies,which increased the difficulty in determining a uniform standard. Two possible explanations can be identified: First, this parameter is a continuous variable, and the cut-off values are inconsistent in different studies; alternatively, the study subjects are diverse and included individuals with signet ring cell EGC, undifferentiated-typeEGC, and mixed type EGC among others, which may also account for the difference.

Table 2 Lymph node metastasis in early gastric cancer according to therapeutic indications
In the latest gastric cancer treatment guidelines (2014 ver. 4), the JGCA noted that endoscopic dissection should be defined as noncurative if mucinous adenocarcinoma is found in the submucosal layer, regardless of whether the mucinous cells are believed to be derived from a differentiated or undifferentiated-type tumor. We conclude that the histological pattern of mucinous adenocarcinoma is an independent risk factor for LNM based on multivariate analysis, which provided powerful evidence to support this statement. With regard to signet ring cell carcinoma in EGC,it has been reported that the LNM rate of signet ring cell-type tumors is lower than that of other undifferentiated-type carcinomas and is equivalent to that of differentiated-type carcinomas[20], which is in line with our results. This suggests that ESD is more feasible for signet ring cell carcinoma compared with other early undifferentiated-type gastric carcinomas. However, the cellular histology of signet ring cell carcinoma is an important factor for LNM in EGC[21]. Huh et al[22]also stated that EGC with a mixed signet ring cell histology exhibited more aggressive behavior than pure tubular adenocarcinoma or pure signet ring cell carcinoma. Hence, a more accurate application of the classification of signet ring cell carcinoma could improve the ESD criteria.
In a previous study that focused on the prognosis of different types of gastric cancer as classified by the Lauren classification, patients with MT carcinomas were found to be significantly more likely to have LNM than patients with IT and DT carcinomas, which was also confirmed in our study. A possible explanation of this difference is that patients with MT tumors always exhibit severe characteristics,including larger lesion sizes and a higher frequency of spread into local lymphatic and venous vessels or regional lymph nodes[23]. In various clinical and pathological studies, LVI has been reported to be the strongest risk factor for nodal metastasis in EGC[24], and we confirmed this finding by showing that LVI predicted a high risk of LNM in EGC. However, unlike other risk factors that can be observed by endoscopic investigation and other auxiliary examinations, LVI is difficult to detect before the ER specimen is obtained. However, based on the criteria for local treatment, the presence of LVI commonly requires additional extended surgery, which is clinically significant.As shown in Table 3, every histopathological factor included in this study was significantly associated with LNM, which indicates that all of these factors are vitally important for performing an accurate pathological analysis after gastroscopic examination.
Researchers have previously concluded that the overall 3-year survival rate was higher in patients without LNM and that patients with LNM had a higher rate of tumor recurrence[25]. Several factors are associated with an increased rate of LNM. The risk factors varied in some relevant studies, but LVI, submucosal invasion,histological type, and tumor size were found to be significantly related to LNM in almost every study. Consistent with other studies[7,18,26], our study demonstrated that age, sex, tumor location, macroscopic type, presence of ulcers, tumor differentiation,Lauren type, and H. pylori infection were not independent risk factors for LNM,although some of these factors were statistically significant in the univariate analysis.Specifically, we analyzed other clinical features, such as drinking and smoking history, obesity, family history of tumors, and the levels of the tumor marker CEA,which is an innovative aspect of this study. In recent years, biomarkers have begun to play an increasingly important role in the detection and management of patients with gastrointestinal malignancies[27]. Serum CEA is considered a complementary test,although it is insufficient to diagnose EGC and LNM. In this study, a higher than normal CEA value was found to be statistically significant in univariate analysis,which attaches great importance to its preoperative detection. However,inconsistencies were found among the test items of the included patients, which made it difficult to perform an analysis of other less common tumor markers. Buckland et al[28]reported that nicotine and alcohol played an important role in the development of gastric cancer, and therefore, we further analyzed the relationships between drinkingand smoking with LNM. Despite the lack of significant association between the occurrence of LNM and these lifestyle habits in this study, we cannot ignore these factors because the clinical data collected in retrospective studies may be incomplete.Although this research, to the best of our knowledge, involved the largest number of EGC patients in China, the limitation that it was a retrospective study at a single institution should still be noted. Therefore, a well-designed multicentric prospective study is needed.

Table 3 Lymph node metastasis in early gastric cancer according to the endoscopic submucosal dissection indications
In conclusion, the absolute indications for ESD can be applied to Chinese patients,while the feasibility of expanding these indications requires further investigation. The predictive factors for LNM included submucosal invasion depth, LVI, mucinous adenocarcinoma, and large lesion size. Taking the histology of tumors into consideration when deciding upon the ESD indications is therefore of great necessity.
invasion.
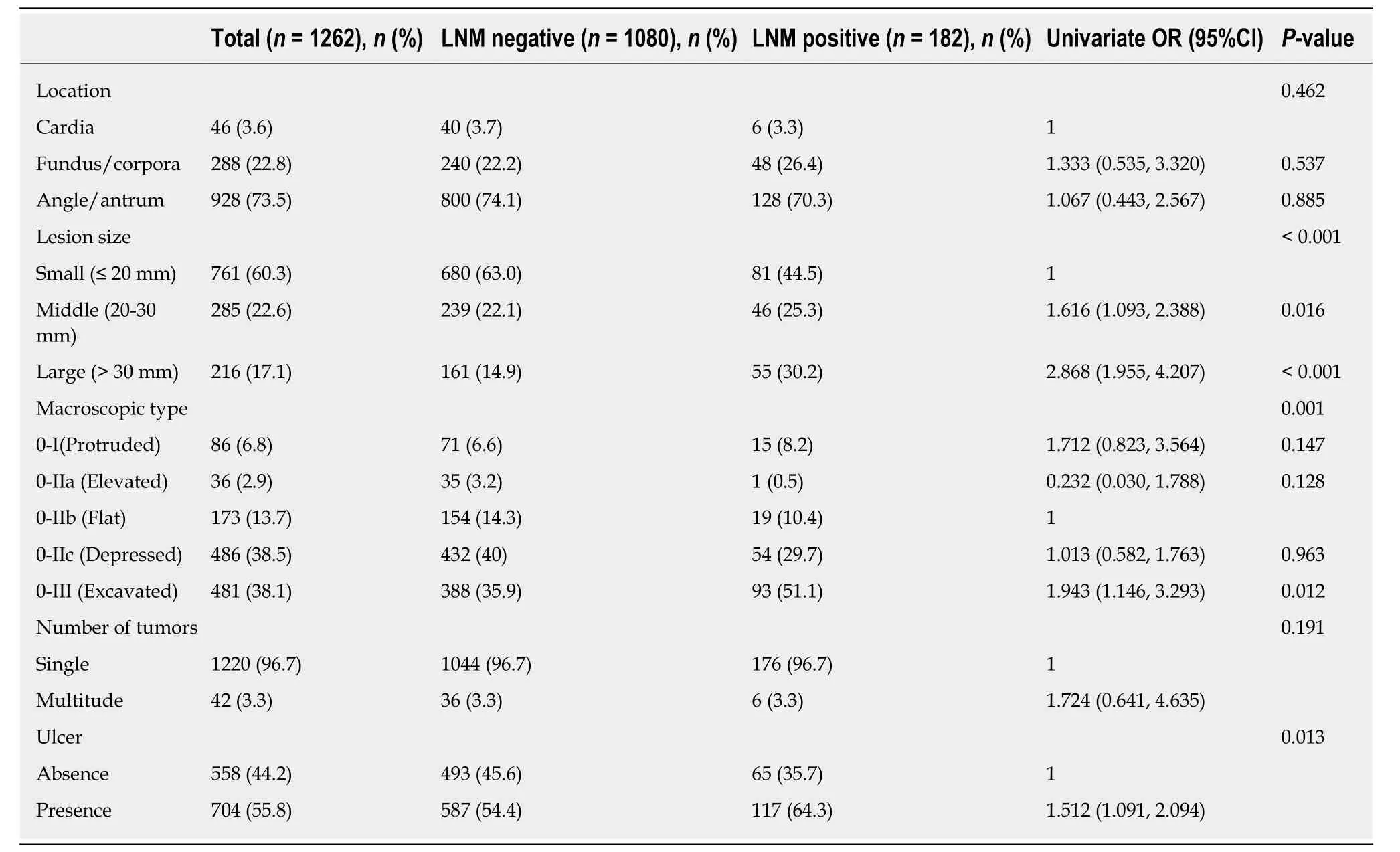
Table 4 Lymph node metastasis risk according to endoscopic features
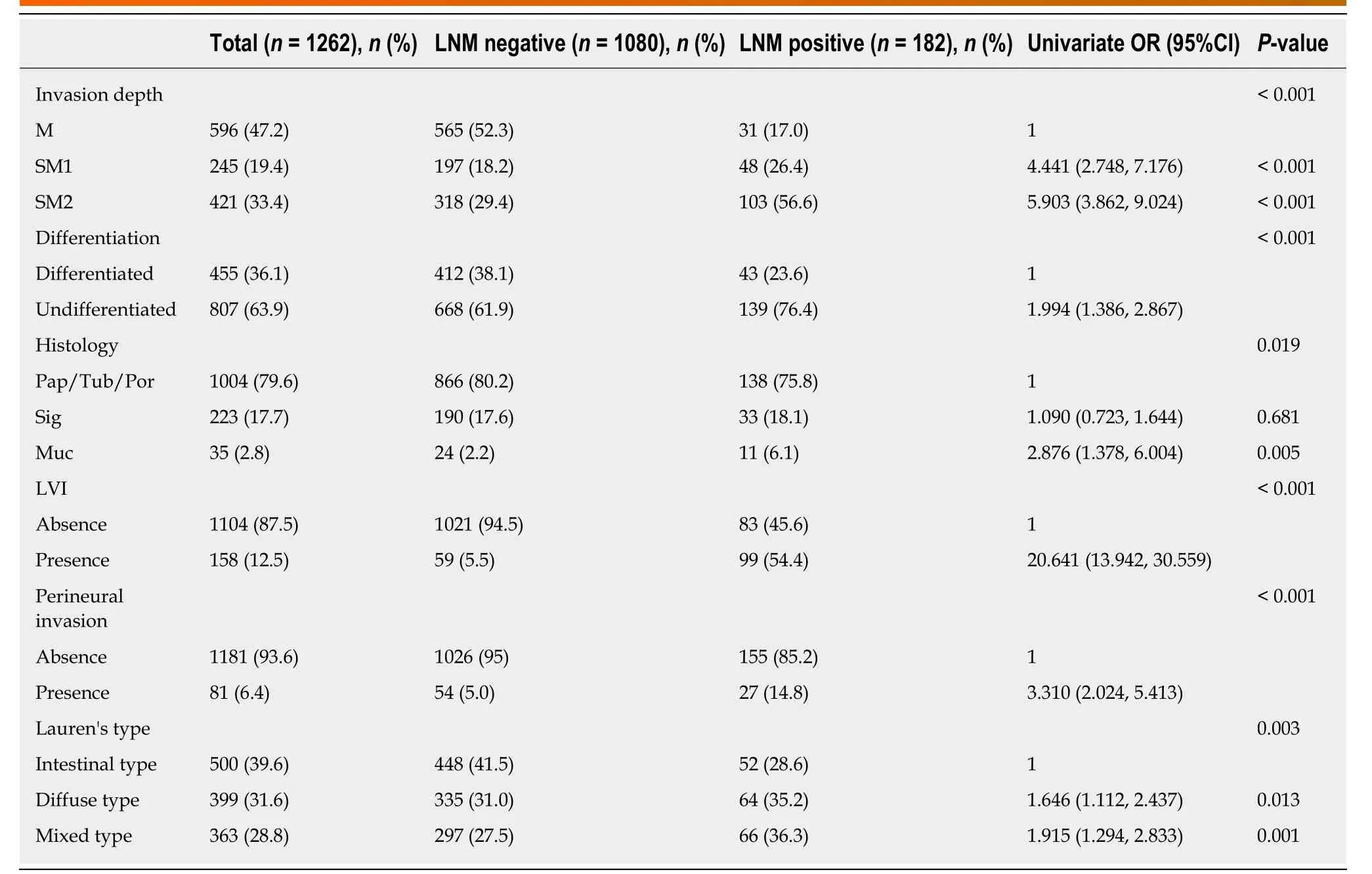
Table 5 Lymph node metastasis risk according to histopathological characteristics

Table 6 Multivariate logistic regression analysis of lymph node metastasis in early gastric cancer
ARTICLE HIGHLIGHTS

Research conclusions
The absolute indications for ESD can be applied to Chinese patients, while the feasibility of expanding these indications requires further investigation. The predictive factors for LNM included submucosal invasion depth, LVI, mucinous adenocarcinoma, and large lesion size. This study provides clinicians with important reference when evaluating the risk of LNM and determining the best course of management for EGC patients.
Research perspectives
Besides invasion depth, LVI, and lesion size, taking the histology of tumors into consideration when deciding upon the ESD indications is vitally important. In addition, preoperative detection of tumor markers is of great necessity. The direction of the future research is to further optimize the ESD indications by analyzing the predictive factors for LNM in EGC. A well-designed multicentric prospective study is the best method for the future research.
猜你喜欢
杂志排行

World Journal of Gastroenterology的其它文章
- How does Helicobacter pylori cause gastric cancer through connexins: An opinion review
- Colorectal cancer: Parametric evaluation of morphological,functional and molecular tomographic imaging
- Sarcopenia and cognitive impairment in liver cirrhosis: A viewpoint on the clinical impact of minimal hepatic encephalopathy
- Significance of tumor-infiltrating immunocytes for predicting prognosis of hepatitis B virus-related hepatocellular carcinoma
- Long non-coding RNA highly up-regulated in liver cancer promotes exosome secretion
- Circular RNA PIP5K1A promotes colon cancer development through inhibiting miR-1273a