雷贝拉唑联合胃复春片用于消化性溃疡的临床效果及对血清VEGF、LPO、SOD、NO的影响
2019-09-10季文媛卫佳琪刘炜
季文媛 卫佳琪 刘炜
通訊作者:刘炜,首都医科大学附属北京世纪坛医院药剂科。
摘要:目的:研究雷贝拉唑联合胃复春片用于消化性溃疡的临床效果及对血清血管内皮生长因子(VEGF)、过氧化脂质(LPO)、超氧化物歧化酶(SOD)、一氧化氮(NO)的影响。方法:选取2015年9月至2016年8月我院收治的62例消化性溃疡患者,根据患者入院顺序分为观察组和对照组,31例每组。对照组使用雷贝拉唑钠肠溶片完成治疗,观察组加以胃复春片完成治疗。比较两组临床疗效,血清VEGF、LPO、SOD、NO水平,临床症状评分。结果:治疗后,观察组临床总有效率显著高于对照组[90.32%(28/31)比64.52%(20/31)](P<0.05)。 治疗前,两组患者呃逆暖气、畏寒肢体、倦怠乏力、便溏、纳呆食少、脘腹胀满、胃脘痛临床症状评分比较无显著差异(P>0.05),治疗后,两组患者呃逆暖气、畏寒肢体、倦怠乏力、便溏、纳呆食少、脘腹胀满、胃脘痛临床症状评分较治疗前显著降低(P<0.05),和对照组相比,观察组的呃逆暖气、畏寒肢体、倦怠乏力、便溏、纳呆食少、脘腹胀满、胃脘痛临床症状评分较低(P<0.05)。治疗前,两组患者血清VEGF、LPO、SOD、NO水平比较无显著差异(P>0.05),治疗后,和治疗前相比,两组患者血清LPO水平显著降低(P<0.05),VEGF、SOD、NO水平显著上升(P<0.05),和对照组相比,观察组的血清LPO水平较低(P<0.05),VEGF、SOD、NO水平较高(P<0.05)。结论:雷贝拉唑联合胃复春片用于消化性溃疡,能有效降低患者LPO水平,升高VEGF、SOD、NO水平,临床疗效良好。
关键词:雷贝拉唑;胃复春片;消化性溃疡
Abstract: Objective: To study the clinical effect of rabeprazole combined with Weifuchun tablet on peptic ulcer and the effect of serum vascular endothelial growth factor (VEGF), lipid peroxidation (LPO), superoxide dismutase (SOD) , Nitric oxide (NO). Methods: Sixty - two patients with peptic ulcer were selected in our hospital from September 2015 to August 2016, those patients were divided into observation group and control group according to the order of admission. In the control group, rabeprazole sodium enteric-coated tablets were used to complete the treatment, the observation group was treated with Weifuchun Tablet on the basis of control group. The clinical efficacy, serum VEGF, LPO, SOD, NO levels and clinical symptom scores were compared between the two groups. Results: After treatment, the total effective rate of the observation group was significantly higher than that of the control group [90.32% (28/31) vs 64.52% (20/31)] (P <0.05). Before treatment, there were no significant differences in hiccup heating, deflated limbs, fatigue, fatigue, loose stools, eat less appetizers, abdominal distention, epigastric pain clinical symptoms between the two groups (P> 0.05). After treatment, the clinical symptoms of hiccup heating, deflated limbs, fatigue, fatigue, loose stools, eat less appetizers, abdominal distention, epigastric pain between the two groups were significantly lower than those before treatment (P <0.05). compared with control group, the clinical symptoms of hiccup heating, deflated limbs, fatigue, fatigue, loose stools, eat less appetizers, abdominal distention, epigastric pain in the observation group were significantly lower (P <0.05). There were no significant differences in serum VEGF, LPO, SOD and NO between the two groups before treatment (P> 0.05), after treatment, compared with before treatment, the levels of serum LPO were significantly decreased (P <0.05), and the levels of VEGF, SOD and NO were significantly increased (P <0.05), compared with the control group, the levels of serum LPO in the observation group were lower (P <0.05), and the levels of VEGF, SOD and NO were higher (P <0.05). Conclusion: Rabeprazole combined with Weifuchun tablet is used to digest peptic ulcer, which can reduce the level of LPO, increase the level of VEGF, SOD and NO, and have good clinical curative effect.
Key words: Rabeprazole; stomach rejuvenation tablets; peptic ulcer
一、前言
消化性溃疡在临床中属于较为常见的一种多发性慢性病,其中强力抑酸治疗溃疡或根除幽门螺杆菌能有效缓解消化性溃疡[1]。然而依然有部分消化性溃疡经常规治疗其疗效不甚理想,难以有效治疗溃疡,一旦停止治疗后,溃疡极易复发[2]。但消化性溃疡的复发问题为临床治疗造成了极大的压力。消化性溃疡愈合主要体现为多种细胞因子的参与作用,进而上皮组织得以修复,溃疡愈合的质量很大程度上和溃疡复发情况有关[3-4]。血管内皮生长因子(VEGF)、过氧化脂质(LPO)、超氧化物歧化酶(SOD)、一氧化氮(NO)等指标在消化性溃疡的临床诊断中发挥着极其重要的作用。为给临床在治疗消化性溃疡方面提供可借鉴之处,本文就雷贝拉唑联合胃复春片用于消化性溃疡的临床效果及对血清VEGF、LPO、SOD、NO的影响进行分析,报道如下。
二、资料与方法
(一)临床资料
选取2015年9月至2016年8月我院收治的62例消化性溃疡患者。纳入标准:① 所有患者均通过病理和胃镜检查被确诊为消化性溃疡;② 在开展治疗前1个月,未进行过铋剂抗生素治疗;③ 依从性较好者,能配合医护人员完成本次研究;④ 胃肠手术及幽门梗阻史。排除标准:① 对本次研究中的药物具有过敏现象;② 肾脏功能不全者;③ 吻合口溃疡、巨大溃疡等特殊类型溃疡;④ 对多种药物过敏或过敏体质者。本次研究已取得我院伦理委员会批准,及得到患者及家属同意。
根据患者入院顺序分为观察组和对照组,31例每组。观察组中男性18例,女性13例;年龄为28~62岁,平均(43.28±5.18)岁;溃疡类型:11例为十二指肠溃疡,13例属于胃溃疡,7例属于混合型溃疡。对照组男性16例,女性15例;年龄为30~63岁,平均(43.31±5.21)岁;溃疡类型:13例为十二指肠溃疡,12例属于胃溃疡,6例属于混合型溃疡。两组患者性别、年龄等方面比较无明显差异(P>0.05)。
(二)方法
对照组使用雷贝拉唑钠肠溶片(生产厂家:山东新华制药股份有限公司,规格:10mg8s,生产批号:20150204)完成治疗,20mg/次,2次/天,早晚服用,连续治疗8周。观察组在此基础上加以胃复春片(生产厂家:杭州胡庆余堂药业有限公司,规格:0.36g60片/瓶/盒,生产批号:20150312)完成治疗,4片/次,3次/天,中药和西药使用时间间隔为30min,连续治疗8周。
(三)观察指标
评判两组患者临床疗效,显效:经胃镜检查,患者临床症状及溃疡处的瘢痕均消失;有效:临床症状已得到有效缓解;无效:在治疗之前,患者的临床症状并未获得改变,同时存在加重的情况[5]。总有效=显效+有效。
分别在治疗前后抽取两组患者5mL的空腹静脉血,转速3000r/min,离心15min,分离血清后,提取血清液,采取酶联免疫吸附检测VEGF水平;使用上海越研生物科技有限公司提供的人过氧化脂质酶联免疫试剂盒检测LPO水平;使用酶联免疫吸附法检测SOD水平,试剂盒由厦门慧嘉生物科技有限公司提供;由上海继锦化学科技有限公司所提供的一氧化氮检测试剂盒检测NO水平。
分析两组患者治疗前后临床症状评分,评价项目包括呃逆嗳气、畏寒肢冷、倦怠乏力、便溏、纳呆食少、脘腹胀满、胃脘痛,分数为0~3分,临床症状越为严重,其分数越高。
(四)统计学处理
选取spss11.5软件包对本次实验数据予以处理,用( ±s)对计量资料进行表示,进行t检验,用[n(%)]对计数资料进行表示,予以χ2检验,等级资料用[n(%)]表示,并进行秩和检验,其P<0.05,提示存在统计学意义。
三、结果
(一)两组患者临床疗效分析
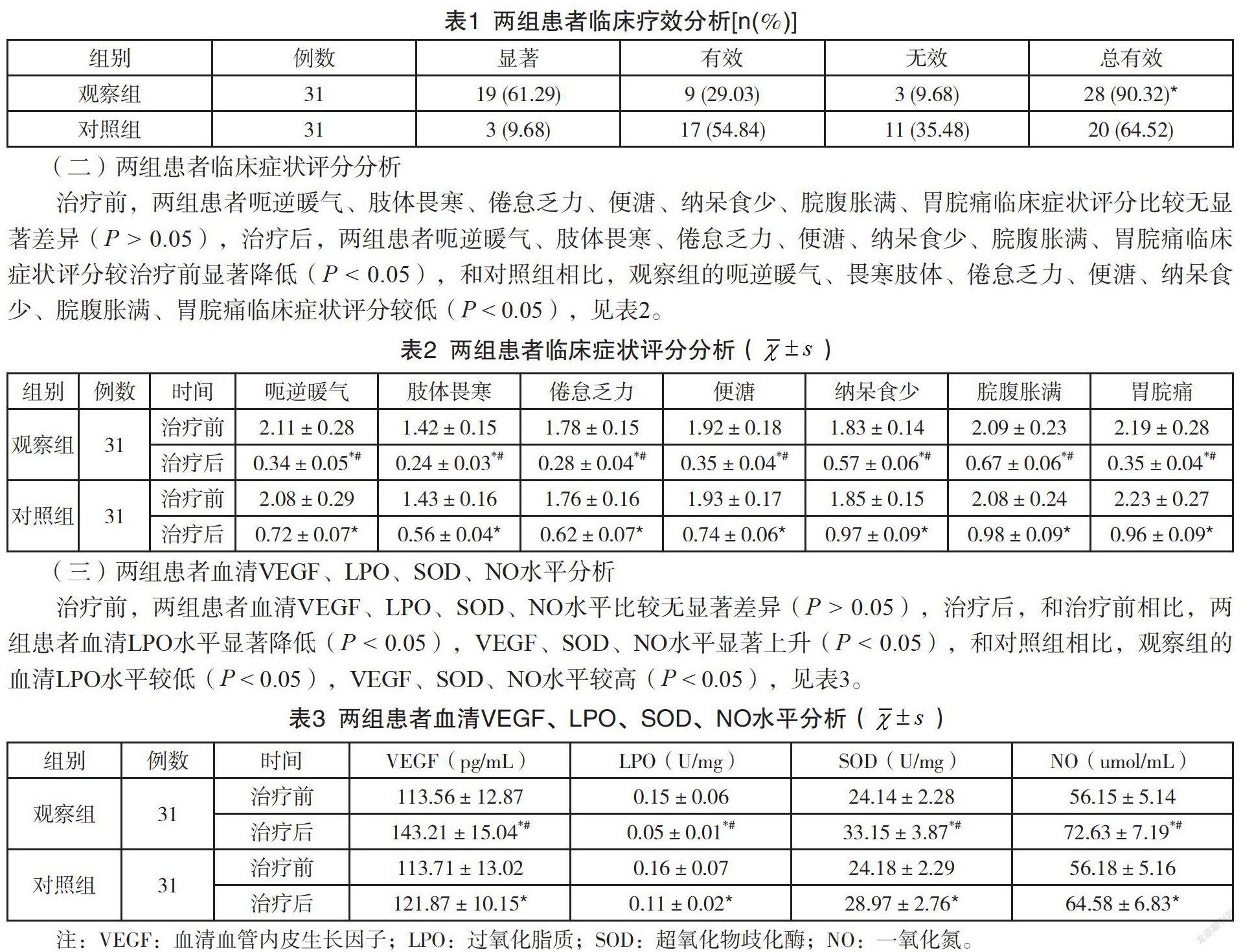
治疗后,观察组临床总有效率显著高于对照组[90.32%(28/31)比64.52%(20/31)](P<0.05),见表1。
(二)两组患者临床症状评分分析
治疗前,两组患者呃逆暖气、肢体畏寒、倦怠乏力、便溏、纳呆食少、脘腹胀满、胃脘痛临床症状评分比较无显著差异(P>0.05),治疗后,两组患者呃逆暖气、肢体畏寒、倦怠乏力、便溏、纳呆食少、脘腹胀满、胃脘痛临床症状评分较治疗前显著降低(P<0.05),和对照组相比,观察组的呃逆暖气、畏寒肢体、倦怠乏力、便溏、纳呆食少、脘腹胀满、胃脘痛临床症状评分较低(P<0.05),见表2。
(三)两组患者血清VEGF、LPO、SOD、NO水平分析
治疗前,两组患者血清VEGF、LPO、SOD、NO水平比较无显著差异(P>0.05),治疗后,和治疗前相比,两组患者血清LPO水平显著降低(P<0.05),VEGF、SOD、NO水平显著上升(P<0.05),和对照组相比,观察组的血清LPO水平较低(P<0.05),VEGF、SOD、NO水平较高(P<0.05),见表3。
四、讨论
消化性溃疡作为一种慢性溃疡,发病部位以胃和十二指肠为主,作为多因素疾病,其中抗幽门螺杆菌感染和胃肠粘膜保护作用的降低作为此病的重要因素,过多的胃酸分泌对溃疡的形成发挥着极其重要的作用[6-7]。消化性溃疡会给人们生活质量造成严重影响,此病的病因和发病機制较为复杂,在目前尚未得到阐明,其中胃黏膜的发生很大程度上和胃黏膜防御因素与损伤因素之间的失衡有关[8]。黏膜血流、细胞再生、碳酸盐、胃黏膜-粘液屏障等均属于胃黏膜防御因素;胆盐、酒精、幽门螺杆菌感染、胃蛋白酶、胃酸等均属于胃黏膜损伤因素[9-10]。当前在治疗消化性溃疡中以保护胃黏膜、阻碍胃酸分泌及根除幽门螺杆菌为主。
雷贝拉唑属于较为新型的一种质子泵抑制剂,雷贝拉唑钠作为此药物的主要成分[11]。雷贝拉唑在非竞争性阻碍H+-K+-ATP酶的作用下能抑制胃酸分泌,相对于传统质子泵抑制剂,雷贝拉唑不但能有效阻碍幽门螺杆菌,同时具备安全性高、个体差异小、持续作用稳定、阻碍胃酸分泌强、较长的作用时间、起效快等优势[12-14]。在临床中使用雷贝拉唑能有效缓解消化性溃疡患者上腹不适、腹痛等临床症状,然而依然有部分患者的临床疗效不甚理想。
在中医学看来,消化性溃疡病位在胃,牵涉到肝脾两脏,脾胃虚弱为本,溃疡发病和转归很大程度上和脾虚有关,同时脾虚也会影响溃疡的愈合和复发[15-17]。脾虚主要体现为气血生化乏源,一旦机体抗病能力降低,极有可能患病;脾胃虚弱生湿化热,也易产生痰饮、食滞、血淤等病理产物[18-19]。但溃疡日久,病情反复发作,淤血阻络,久病入络,因此虚、淤为本病的主要特点,因此消化性溃疡属于本虚标实之证,可见,在治疗消化性溃疡方面应以化瘀生新、活血止痛、健脾益气为主[20-21]。
胃复春片主要由炒枳壳、香茶菜、红参等组合而成,具备活血解毒、健脾益气的作用,在功能性消化不良、萎缩性胃炎、慢性浅表性胃炎等疾病中已获得广泛应用[22-23]。相关研究显示,在消化性溃疡中经雷贝拉唑联合胃复春片治疗,能促进溃疡愈合,增强溃疡质量,同时能消除消化性溃疡的临床症状,有利于增加中医症候和疾病的有效性,近期临床疗效较为显著[24-25]。本次研究结果显示,通过对消化性溃疡患者予以雷贝拉唑联合胃复春片治疗后,发现患者的临床有效性显著高于单纯的雷贝拉唑治疗者,究其原因可能是因为胃复春片在消化性溃疡中能发挥一定抑制作用。除此之外,雷贝拉唑联合胃复春片治疗消化性溃疡能有效改善患者呃逆暖氣、畏寒肢体、倦怠乏力、便溏、纳呆食少等临床症状。
相关研究显示,细胞生长因子的表达水平和消化性溃疡愈合质量存在着密切关联性,在消化性溃疡中VEGF作为关键的细胞生长因子[26]。VEGF对溃疡组织的修复过程起着参与性作用,具备多生物活性的细胞因子,和其它细胞因子相比作用可促使细胞外基质堆积。除此之外,VEGF对细胞外基质的修饰、产生及成分变化起着调节性作用,对细胞间及细胞黏附的相互作用具有重要作用,对血管的再生及组织的修复发挥着极大的促进作用,同时对溃疡的愈合及组织的新生具有明显的促进作用[27-28]。相关研究者提出LPO、SOD、NO等指标在某种程度上能反映消化性溃疡的发展和转归,因此,在临床诊断和治疗中上述指标具有重要的临床指导价值[29-30]。本次研究结果显示,通过对消化性溃疡患者予以雷贝拉唑联合胃复春片治疗后,发现患者的LPO水平显著降低,VEGF、SOD、NO水平显著上升,提示雷贝拉唑联合胃复春片能增加VEGF、SOD、NO表达,降低LPO水平,促使溃疡的愈合,增强了溃疡的愈合质量。
总之,雷贝拉唑联合胃复春片用于消化性溃疡,能有效降低患者LPO水平,升高VEGF、SOD、NO水平,临床疗效良好。
参考文献
[1] Xiao X, Lau JY. Over-the-scope clip treatment of refractory peptic ulcer bleeding[J]. Gastrointestinal endoscopy, 2016,83(2):458-459.
[2] Vester-Andersen M, Lundstrøm LH, Buck DL, et al. Association between surgical delay and survival in high-risk emergency abdominal surgery. A population-based Danish cohort study[J]. Scandinavian journal of gastroenterology, 2016,51(1):121-128.
[3]Kärkkäinen JM, Miilunpohja S, Rantanen T, et al. Alcohol Abuse Increases Rebleeding Risk and Mortality in Patients with Non-variceal Upper Gastrointestinal Bleeding[J]. Digestive diseases and sciences, 2015,60(12):3707-3715.
[4]Desai V, Gonda D, Ryan SL, et al. The effect of weekend and after-hours surgery on morbidity and mortality rates in pediatric neurosurgery patients[J]. Pediatrics, 2015,16(6):726-731.
[5]Realo A, Teras A, Kööts-Ausmees L, et al. The relationship between the Five-Factor Model personality traits and peptic ulcer disease in a large population-based adult sample[J]. Scandinavian journal of psychology, 2015,56(6):693-699.
[6]Chang SS, Hu HY. Helicobacter pylori: Effect of coexisting diseases and update on treatment regimens[J]. World journal of gastrointestinal pharmacology and therapeutics, 2015,6(4):127-136.
[7]Alimadadi M, Seyyedmajidi M, Amirkhanlou S,et al. Impact of Creatinine Clearance on Helicobacter Pylori Eradication Rate in Patients With Peptic Ulcer Disease[J]. Iranian journal of kidney diseases, 2015,9(6):427-432.
[8]Murata A, Mayumi T, Muramatsu K, et al. Effect of dementia on outcomes of elderly patients with hemorrhagic peptic ulcer disease based on a national administrative database[J]. Aging clinical and experimental research, 2015,27(5):717-725.
[9]Paudel MS, Kc S, Mandal AK, et al. Acute Upper Gastrointestinal Bleeding in a Tertiary Care Centre of Nepal[J]. JNMA J Nepal Med Assoc, 2017,56(206):211-216.
[10]Minalyan A, Gabrielyan L, Scott D,et al. The Gastric and Intestinal Microbiome: Role of Proton Pump Inhibitors[J]. Curr Gastroenterol Rep, 2017,19(8):42.
[11]Li H, Yang T, Liao T, et al. Insights from the redefinition of Helicobacter pylori lipopolysaccharide O-antigen and core-oligosaccharide domains[J]. Microb Cell, 2017,4(5):175-178.
[12]Triantos C, Kalafateli M, Spantidea PI,et al. Bacterial load and cytokine profile in patients with cirrhosis following therapy with proton pump inhibitors: a prospective cohort study[J]. Ann Gastroenterol, 2017,30(4):450-456.
[13]Ghosh CK, Khan MR, Alam F, et al. Peptic Ulcer Disease in Bangladesh: A Multi-centre Study[J]. Mymensingh Med J, 2017,26(1):141-144.
[14]Jang JY. Recent Developments in the Endoscopic Treatment of Patients with Peptic Ulcer Bleeding[J]. Clin Endosc, 2016,49(5):417-420.
[15]Chen H, Olatunji OJ, Zhou Y. Anti-oxidative, anti-secretory and anti-inflammatory activities of the extract from the root bark of Lycium chinense (Cortex Lycii) against gastric ulcer in mice[J]. J Nat Med, 2016,70(3):610-619.
[16]Li LF, Chan RL, Lu L, et al. Cigarette smoking and gastrointestinal diseases: the causal relationship and underlying molecular mechanisms (review)[J]. Int J Mol Med, 2014,34(2):372-380.
[17]Song DU, Jang MS, Kim HW, et al. Gastroprotective Effects of Glutinous Rice Extract against Ethanol-, Indomethacin-, and Stress-induced Ulcers in Rats[J]. Chonnam Med J, 2014,50(1):6-14.
[18]Sachs G, Shin JM, Munson K, et al. Gastric acid-dependent diseases: a twentieth-century revolution[J]. Dig Dis Sci, 2014,59(7):1358-1369.
[19]Machado-Alba JE, Castrillón-Spitia JD, Londoño-Builes MJ, et al. An economic analysis of inadequate prescription of antiulcer medications for in-hospital patients at a third level institution in Colombia[J]. Rev Esp Enferm Dig, 2014,106(2):77-85.
[20]Carr WR, Mahawar KK, Balupuri S, et al. An evidence-based algorithm for the management of marginal ulcers following Roux-en-Y gastric bypass[J]. Obes Surg, 2014,24(9):1520-1527.
[21]Bercovich E, Keinan-Boker L, Shasha SM. Long-term health effects in adults born during the Holocaust[J]. Isr Med Assoc J, 2014,16(4):203-207.
[22]Graham DY. History of Helicobacter pylori, duodenal ulcer, gastric ulcer and gastric cancer[J]. World J Gastroenterol, 2014,20(18):5191-5204.
[23]Chey WD, Leontiadis GI, Howden CW, et al. ACG Clinical Guideline: Treatment of Helicobacter pylori Infection[J]. Am J Gastroenterol, 2017,112(2):212-239.
[24]Dorajoo SR, See V, Chan CT, et al. Identifying Potentially Avoidable Readmissions: A Medication-Based 15-Day Readmission Risk Stratification Algorithm[J]. Pharmacotherapy, 2017,37(3):268-277.
[25]Amouei A, Ehsani F, Zarch MB, et al. Peritonitis Following Duodenal Ulcer Perforation in a Newborn: A Case Report[J]. J Clin Diagn Res, 2016,10(11):PD10-PD11.
[26]Ha X, Peng J, Zhao H, et al. Enhancement of Gastric Ulcer Healing and Angiogenesis by Hepatocyte Growth Factor Gene Mediated by Attenuated Salmonella in Rats[J]. J Korean Med Sci, 2017,32(2):186-194.
[27]Goyal R, Debi U, Dey P, et al. Zollinger-Ellison syndrome: an unusual case of chronic diarrhoea in a child[J]. Malays J Pathol, 2016,38(3):321-325.
[28]Zhou LY, Song ZQ, Xue Y, et al. Recurrence of Helicobacter pylori infection and the affecting factors: A follow-up study[J]. J Dig Dis, 2017,18(1):47-55.
[29]Kwiecien S, Magierowska K, Magierowski M, et al. Role of sensory afferent nerves, lipid peroxidation and antioxidative enzymes in the carbon monoxide-induced gastroprotection against stress ulcerogenesis[J]. J Physiol Pharmacol, 2016,67(5):717-729.
[30]Lee S, Jeong S, Kim W,et al. Rebamipide induces the gastric mucosal protective factor, cyclooxygenase-2, via activation of 5'-AMP-activated protein kinase[J]. Biochem Biophys Res Commun, 2017,483(1):449-455.
