Common iliac artery occlusion with small intestinal transection caused by blunt abdominal trauma: A case report and review of the literature
2019-08-14YouXinZhouYongJiJingChenXinYangQingZhouJianLv
You-Xin Zhou,Yong Ji,Jing Chen,Xin Yang,Qing Zhou,Jian Lv
Abstract
Key words: Common iliac artery occlusion; Transection of the small intestine; Blunt abdominal trauma; Case report; Percutaneous transluminal angioplasty; Anastomosis of the intestine
INTRODUCTION
Penetrating rather than blunt trauma causes the greatest majority of vascular injuries.As a subset of arterial blunt trauma,the percentage of iliac arterial injury is small.The largest review of these cases in the literature was published by Tuechet al[1],who reviewed 9 patients with common iliac artery occlusion in blunt trauma.We add to these rare cases in the literature by reporting a new case here.Furthermore,we review 7 cases reported between the years of 2001 and 2018,and discuss the mechanism of injury,clinical presentation and signs,diagnosis,surgical modalities,and outcome.
CASE PRESENTATION
Chief complaints
A 56-year-old male steel worker's lower abdomen had been compressed between two forklifts.He was admitted to the People’s Hospital of Jingjiang with pain and numbness in the left lower extremity and severe pain throughout the entire abdomen,especially in the lower abdomen.
History of past illness
The patient had no significant medical history.
Family history
The patient had no significant family history.
Physical examination
The patient showed clear consciousness upon presentation.Physical examination showed stable vital signs,including blood pressure of 136/68 mmHg (normal range:90-140/60-90 mmHg),pulse rate of 95/min (normal range:60/min-100/min),respiratory rate of 16/min (normal range:16/min-20/min),and temperature of 37.0°C (normal range:36.1°C-37°C).No obvious contusion of the abdominal wall or the left lower limb was noted.He had total abdomen tenderness,with evidence of peritoneal irritation and obvious board-like rigidity of the abdomen.The left lower extremity had good mobility but it was painful and numb,and skin temperature was significantly decreased.Pulsation of the left dorsal pedal artery had disappeared.
对典型的500 kV交流双回路输电线路进行研究,建立了耐张塔及三塔四档的塔-线体系有限元模型,对其分别作了振动特性分析,得出如下结论:
Laboratory examination
Laboratory examination revealed a hemoglobin level of 152 g/L (normal range:130-175 g/L),white blood cell count of 13.2 × 109/L (normal range:3.5 × 109/L to 9.5 ×109/L),and neutrophil percentage of 94.6% (normal range:40%-75%).
Imaging examination
Pre-hospitalization abdominal computed tomography examination had revealed a perforation of the digestive tract.Abdominal computed tomography angiography showed occlusion of the left common iliac artery (Figure 1) and atherosclerosis of the abdominal aorta,bilateral iliac artery,and lower right femoral artery.
FINAL DIAGNOSIS
Common iliac artery occlusion with transection of the small intestine caused by blunt abdominal trauma.
TREATMENT
The patient underwent laparotomy under general anesthesia.Surgical findings included transection of the small intestine at about 2 m away from the ileocecus,without bleeding in the mesentery.About 200 mL of pus was found in the pelvic and abdominal cavity.We performed a partial small bowel resection and then a side-toside small bowel anastomosis using a linear cutting closer (Figure 2A).
The abdominal symptoms of discomfort were completely relieved after the operation; however,the symptom of discomfort in the left leg became more prominent.The patient was immediately transferred to a superior hospital,where arteriography of the left lower extremity was performed,followed by percutaneous transluminal angioplasty with stenting at 4 d later.Unfortunately,the details of those operations were not available.
OUTCOME AND FOLLOW-UP
The postoperative course was uneventful.Physical examination revealed a warm left leg with restoration of pulse and normal sensation.Re-examination by abdominal computed tomography showed good position of the left common iliac artery stent(Figure 2B).The patient was followed for more than 11 mo after the operation and recovered well.
DISCUSSION
Injury to the common iliac artery secondary to blunt trauma is rare[2-6].The reported rates of incidence of iliac artery injuries from trauma range from 0.4% to 7.1%[2,7].The rare nature of this injury is largely due to the vessel’s position in the retroperitoneal location,where it is protected by the bony pelvic girdle[5,6].A total of only 8 cases,including our case reported herein,are present in the literature[8-14].We have summarized the data from these cases on age,sex,causes of injury,location,clinical presentation and signs,findings of auxiliary examination,and associated injuries in Table 1.The data on operative delay time,procedure,fasciotomy,and outcomes are summarized in Table 2.The total 8 patients include 7 males and 1 female,with a mean age of 40 years old (range:9-74 years).The causes of injury were seatbelt syndrome in 3 of the patients,direct compression injury in 4,and car crash in 1.Common iliac artery occlusion occurred on the left and bilateral sides in 2 cases each and on the right in 4.All 8 cases were diagnosed in time.Except for the youngest case among the total 8 and our case,the other 6 cases were treated immediately after admission.Four cases had a good prognosis.For the other 4 cases,2 died,1 suffered paralysis in the right leg,and 1 became paraplegic.
The most common mechanisms of injury appear to be direct anteroposterior compressions[6,15],traction from displaced bone fragments[16],and shearing forces,possibly accentuated by use of a seatbelt[17].In fact,the mechanism of seatbelt syndrome or deceleration injury can also be understood as a type of abdominal compression.A total of 13 patients have been reported with common iliac artery occlusion due to direct anteroposterior compression[1].We also found 4 cases of direct anteroposterior compression.It would be reasonable to assume then that abdominal compression is the main cause of common iliac artery occlusion.Blunt traumainduced abdominal aortic injuries most frequently result in intimal tearing.Atherosclerotic disease has been postulated as a predisposing factor for aortic intimal tearing because of intimal weakening and loss of both elasticity and compliance[15,18].In our patient,abdominal computed tomography angiography examination showed atherosclerosis of the abdominal aorta,bilateral iliac artery,and lower right femoral artery.We can speculate that the occlusion of the left common iliac artery may also have been caused by atherosclerotic plaque rupture.Endometrial tear,atherosclerotic plaque rupture,and intramural hematoma formation can lead to common iliac artery diameter reduction or even occlusion.If the compression force is strong enough,it may lead to transection of the common iliac artery[19].

Figure 1 Abdominal computed tomography findings of a common iliac artery occlusion.
Because of the low incidence of this injury,its atypical symptoms,and frequent association with other severe injuries,the diagnosis is often missed or delayed.This can cause serious harm to the patients.Therefore,our attention should be focused on proper identification and early diagnosis.The clinical manifestations and signs of acute lower limb ischemia can provide important clues for the diagnosis.It is important to note that acute limb ischemia caused by common iliac artery occlusion from blunt abdominal trauma is rare[2,5]and clinical presentation may be delayed for months or years[6,17].Tuechet al[1]reported the median operative delay time to be 15 d,ranging from 3 d to 36 years.All of the 8 cases we reviewed (including our own)presented acute lower limb ischemia.This may be the main reason why they were able to receive timely diagnosis and treatment.Except for the youngest patient and our patient among these 8 total cases,the other 6 patients were diagnosed and treated shortly after admission.The youngest and our patient were also diagnosed shortly after admission but the surgery was performed 4 d later.For the former,given the patient's young age and incomplete occlusion with severe multiple injuries,a conservative initial approach was decided.For the latter,we delayed operation due to the incomplete occlusion allowing for a longer observation period.
Most patients present with other injuries,such as traumatic intestinal perforation,pelvic fracture,liver and spleen injury,bladder rupture,and contusion of the thoracoabdominal wall,among others.Treating clinicians should be especially careful with these patients because the signs and symptoms of vascular injury may be obscured by the signs and symptoms of other injury,especially in those patients who do not show acute lower limb ischemia.It is very important to inquire about the patient's detailed medical history and to perform a meticulous physical examination.In addition,it is also necessary to go to the bedside frequently,to observe any changes in the patient’s condition because changes in emergency patients are dynamic.
Angiography is the gold standard for diagnosis and should be performed when there is a clinical doubt.The development of abdominal computed tomography angiography has allowed for three-dimensional reconstruction of the blood vessels and a clearer assessment of the location and extent of damage,which can help surgeons in deciding on the correct treatment strategies.The precondition of angiography is the hemodynamic stability of the patient.It is generally contraindicated in a hemodynamically unstable patient with multisystem injury; for these patients,duplex ultrasonography may be helpful.Among the total 8 cases discussed herein,6 underwent angiography,3 of which were given the abdominal computed tomography angiography; the 2 other patients did not undergo any blood vessel examination.

Figure 2 Abdominal computed tomography findings after partial small intestine resection and stentimplantation.
Once injury to the common iliac artery has been determined,operative repair is generally indicated.The surgical procedure includes both open and endovascular approaches.Ligation of the iliac artery results in an unacceptable amputation rate of up to 50%[7].Major vessels should be ligated only when the procedure is considered to be life-saving or in the presence of gross contamination,where subsequent extraanatomical grafting is possible[2].The loss of 1.5 cm of vessel is the maximum length that can be dealt with by mobilization and end-to-end anastomosis[2,13].Furthermore,the vascular wall must be normal before anastomosis and the anastomotic site must be free of tension.Long segment injury may require substitution of a vascular conduit[20].
Autologous vein grafts and synthetic grafts are available.At present it is still debatable which is better - an autologous vein graft or a synthetic graft.Autologous grafting with the hypogastric artery or saphenous vein on injured iliac arteries may give rise to the problems of size discrepancies and time consumption in harvest,making these grafts unfavorable[1,5].Synthetic grafts are more favorable as they are available in various sizes,but they are not ideal in cases of peritoneal contamination from concomitant bowel perforation.Several articles have provided evidence that polytetrafluoroethylene grafts may be used in the face of substantial contamination and may be resistant to subsequent infection[21,22].
Extra-anatomic bypass and femorofemoral or axillofemoral bypass are alternatives.Endovascular techniques have been used to treat a variety of endovascular diseases[23-26].The endovascular approach offers benefits in terms of easier access to the target lesion,reduction in blood transfusion requirement,and obviation of the potential need for systemic heparinization[13].Among the total 8 patients discussed herein,5 underwent endovascular stenting and the remaining 3 underwent open surgery.Jovanovicet al[11]consider that reinforcement of the posterior aortic wall to the anterior longitudinal ligament should be added to the armamentarium of aortic injury treatment.In our case,the final choice of endovascular therapy may have resulted from consideration of the patient’s hemodynamic stability,absence of vessel rupture,and severe abdominal cavity contamination.
Considering that most patients with this injury present with multiple other severe injuries,it is important to remember that the primary purpose of treatment is to save the patient’s life.Therefore,the principles of simplicity and efficiency must be satisfied when choosing the therapeutic method.Endovascular therapy has the advantages of being minimally invasive,having little effect on the patient,and producing clear effect,all of which conform to the above two principles.Among the total 8 patients discussed herein,2 did not receive surgery until 4 d after the diagnosis and neither experienced serious repercussions.
Taking into account the information presented in previous literature reviews of this injury,we noted the consequence of short-term ischemic necrosis of the affected limb to be infrequent.Therefore,within the time allowed,the most serious injury endangering the patient’s life should be addressed first,followed by the compression injury of the lower abdomen when the patient's general condition has stabilized.It is important to avoid multi-organ surgery and long anesthesia time associated with a one-stage operation,especially for patients who are elderly,have underlying basic diseases,or are seriously injured.This is consistent with the current damage control theory; however,the premise is to closely observe changes in the patient’s condition.Once the limb is found to have the tendency of ischemic necrosis,immediate surgical intervention should be initiated.
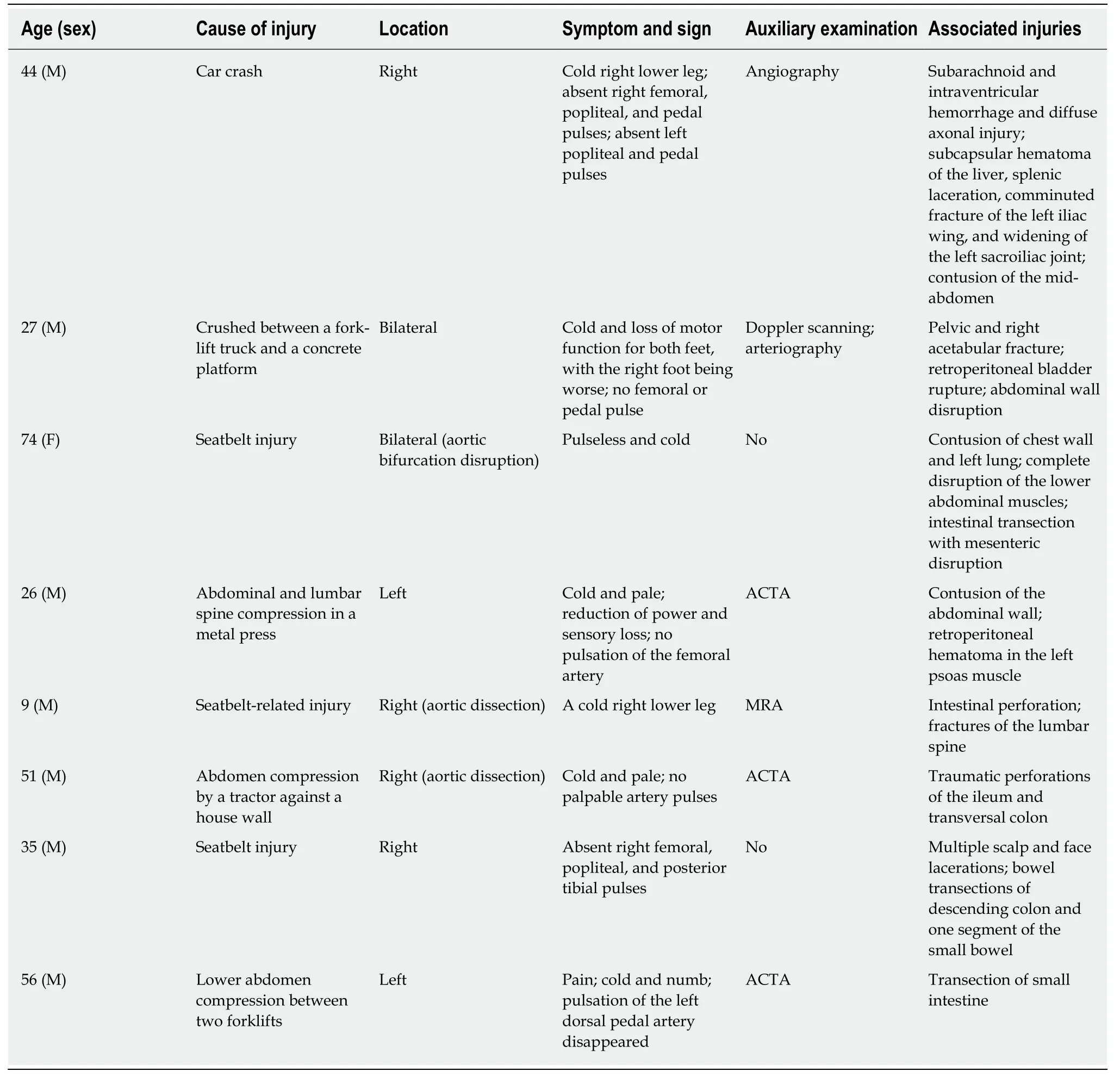
Table 1 Demographic and clinical profile of the cases of compression injury of the lower abdomen in the literature
Compartment syndrome should be anticipated after revascularization.Postoperative increase in pain in the distal limb,any evidence of decreased perfusion,increasing neurological signs,or limb swelling warrant fasciotomy without delay[2].Among the total 8 patients discussed herein,delayed fasciotomy occurred in 3.Certainly,close observation and judicious clinical judgment are necessary in every case.
CONCLUSION
All patients with abdominal trauma should be suspected of having major vascular injury,especially those with compression injury of the lower abdomen.Taking detailed medical history and performing a meticulous physical examination are necessary.In addition,the patient should be carefully observed to detect any changes in the overall condition.It is especially important to consider the most simple and effective methods first,to minimize the risk of death.Ultimately,however,individualized treatment strategies based on each patient's condition are needed and will improve outcomes.

Table 2 Treatment details and prognosis of the 8 cases
猜你喜欢
杂志排行
World Journal of Clinical Cases的其它文章
- Percutaneous coronary intervention for ostial lesions of the left main stem in a patient with congenital single left coronary artery: A case report
- c.753_754delAG,a novel CFTR mutation found in a Chinese patient with cystic fibrosis: A case report and review of the literature
- Fever and neck pain after pacemaker lead extraction: A case report
- Endometriosis of the duplex appendix: A case report and review of the literature
- Gastric duplication cyst mimicking large cystic lymphangioma in an adult: A rare case report and review of the literature
- Oncogenic osteomalacia caused by a phosphaturic mesenchymal tumor of the femur: A case report