Endometriosis of the duplex appendix: A case report and review of the literature
2019-08-14MingYuanZhuFaMingFeiJingChenZhongChengZhouBinWuYiYuShen
Ming-Yuan Zhu,Fa-Ming Fei,Jing Chen,Zhong-Cheng Zhou,Bin Wu,Yi-Yu Shen
Abstract
Key words: Duplex appendix; Horseshoe appendix; Endometriosis; Appendectomy; Case report
INTRODUCTION
Acute appendicitis is the most common surgical emergency of the abdomen.The overall lifetime risk for acute appendicitis is 6.7% in females and 8.6% in males[1].Duplication of the appendix is extremely rare and is usually incidentally found during surgery.A duplication of the appendix was first reported in the form of a case report in 1892[2].To date,only a total of approximately 100 cases have been reported[3].Endometriosis,as a common disease in women of childbearing age,predominantly occurs in the adnexa and less frequently in the digestive tract,especially in the small intestine and appendix.Here,we report a unique case of duplex appendix with acute appendicitis coexisting with appendiceal endometriosis in an adult female patient.In addition,endometriosis was found in the small intestine and ovary.The most special of the duplex appendix is the horseshoe appendix.To the best of our knowledge,only the abovementioned 14 cases have been reported thus far[4],but there are no reports of horseshoe appendix combined with endometriosis.The classification,symptoms,and radiological appearance of the duplex appendix with endometriosis have been described in the literature and are discussed in this paper.
CASE PRESENTATION
Chief complaints
A 44-year-old Chinese woman was admitted to the Emergency Department of The Second Affiliated Hospital of Jiaxing University (Jiaxing,China) because of migratory lower right quadrant pain for 1 d associated with nausea,vomiting,and anorexia.
History of present illness
She reported a 1-d medical history of migratory lower right quadrant pain that started as epigastric pain and became localized to the lower right abdominal quadrant,especially at McBurney’s point.She also complained about nausea,vomiting,and anorexia.
History of past illness
The patient had an 8-year history of repeated lower abdominal pain that appeared in the first 1-2 d of menstruation and disappeared after the end of menstruation.However,her menstrual cycle was regular,with no menorrhagia or dyspareunia reported.Therefore,she was not regularly seen in the gynecology clinic for several years.
Personal and family history
The last menstrual period ended 5 d before admission.She had a history of caesarean section 18 years ago.No additional family history was presented.
Physical examination upon admission
Her abdominal examination revealed that the abdomen was diffusely soft,nondistended,but presented tenderness,rebound tenderness,and guarding with a voluntary component in the lower right quadrant,and increased pain with coughing at the McBurney’s point,which were consistent with the signs of acute appendicitis.Moreover,Rovsing’s sign was positive.No abdominal mass was palpable,and bowel sounds were normoactive.
Laboratory examinations
Hematological examinations,including serum electrolyte levels,human chorionic gonadotropin,and complete blood count were within normal limits,apart from white blood cell count,carbohydrate antigen 125 (CA125),and C-reactive protein concentrations that were mildly elevated at 10.1 × 109/L (77.8% neutrophils),69.5 U/mL,and 10 mg/L,respectively.
Imaging examinations
A computed tomography (CT) scan of the abdomen showed that the appendix was markedly swollen and thickened and had obvious periappendicular leaking;additionally,two fecaliths were located at the root of the appendix (Figure 1).Simultaneously,the CT scan also showed a cystic mass in the right ovary (Figure 1).The findings from the patient’s abdominal examination and CT scan were consistent with acute fecal appendicitis.
FINAL DIAGNOSIS
Based on the above physical examination features and imaging data,a provisional diagnosis of acute appendicitis and right ovarian cyst was made.
TREATMENT
Laparoscopic examination revealed moderate bloody fluid collections,and the omentum was localized to the right lower abdomen and pelvic cavity.Additionally,a cystic mass with a size of 3.5 cm × 2.5 cm was seen in the right ovary,which was not ruptured and was consistent with the CT scan findings.No evidence of endometrium was found by laparoscopic evaluation of the abdominal and pelvic cavities.Moreover,the appendix appeared unusually atrophic upon itself and measured 3 cm × 2.5 cm at the widest diameter,which was obviously inflamed,hyperemic,and swollen,which agreed with the preoperative diagnosis.However,we found a tight adhesion between the appendix,the lateral abdominal wall,and the posterior peritoneum,resulting in unclear anatomical structures that were difficult to separate.Therefore,a laparotomy was performedviaan extended McBurney’s incision in the lower right abdominal quadrant.After carefully separating the adhesions,an appendix was seen.Then,we attempted to separate the base of the appendix,and we were surprised to find that there were two bases that had their cavities both in contact with the cecum with each other through the appendiceal lumen,or “horseshoe appendix” (Figure 2).The two bases were positioned frontally on the cecum with a central mesoappendix,and the central mesoappendix vessel was fan-shaped.The proximal appendix stump and mesoappendix vessel were divided and ligated,and then the appendix was removed for pathological examination.Unfortunately,because there was no consideration of the rarity of this case,there were not enough intraoperative photographs remaining.Upon gross pathological inspection,the total length of the duplex appendix was approximately 6 cm.There were two cavities in the root of the cecum,both of which led to a swollen inflamed appendix containing a fecalith.Subsequently,a meticulous inspection of distal ileal segments and right tuboovarian structures was performed through palpation,and we unexpectedly found a hard mass,10 cm proximal to the ileocecal valve,which gave rise to a mild stenosis of the intestine.Additionally,a right ovarian cyst was found,as previously mentioned.Hence,partial resection of the small intestine with end-to-end anastomosis was executed,as well as right oophorectomy by a gynecologist.Grossly,the soft tissue mass had a size of 1.5 cm × 1.5 cm,but the serosal surface and the mucosa were normal.The cut surface revealed hard nodular regions,which contained some small cystic spaces brimmed with both serous fluid and hemorrhage.The ovarian cyst showed that the cut surface also contained several small cystic spaces and was filled with chocolate-like cyst fluid and old bleeding.
OUTCOME AND FOLLOW-UP

Figure 1 Computed tomography scan of the patient’s abdomen.
Hematoxylin and eosin staining revealed obvious acute and chronic inflammatory cell infiltration within and around the duplex appendix.The lumens of the two appendixes were obstructed with fecalith.Meanwhile,several ectopic endometrialtype glands and stroma were found in the thickened muscularis propria of the duplex appendix (Figure 3),small intestine (Figure 3),and right ovary (Figure 3).Additionally,the glands were dilated,most of which contained hemorrhage within their cavities.Histological diagnoses of duplex appendix with fecalith and endometriosis were made,which caused acute appendicitis,and diagnoses of endometriosis of the small intestine and the right ovary were also made.These results were surprising discoveries.The patient subsequently recovered well with no complications and was discharged from the hospital on the 10th postoperative day.She was referred to a gynecological clinic for further assessment of her endometriosis.At the 6-month follow-up,there were no recurrences of abdominal pain or other clinical symptoms.
DISCUSSION
Duplication of the digestive tract is a rare congenital malformation in adults because more than 80% of cases have serious abdominal or intestinal obstruction before the age of 2 years[5].Appendiceal duplication is extremely rare and may be related to the duplication of other organs or other anomalies.Colons investigated 50000 pathological specimens of the appendix,and there were only just two cases of duplication[6].The overall incidence of appendiceal duplication is approximately 0.004%[6].Appendiceal duplication was first formally classified by Cave in 1936 and divided into three types based on their anatomic locations.Then,this classification was updated and amended in 1962 by Wallbridge[7]and is called the “Cave-Wallbridge” classification.Subsequently,this classification was further improved by Biermannet al[8]and Kjossevet al[9],respectively.However,there were several cases that could not be classified according to the above classifications,for instance,horseshoe appendix and triplex appendix.We believe that an updated classification system is needed to distinguish appendiceal anomalies or to modify the present system.Therefore,Calotăet al[10]proposed a new classification system for appendiceal anomalies in 2010,which was divided into number anomalies and shape anomalies and was modified by Takabatakeet al[11]again in 2016.The new classification system of appendiceal anomalies is presented in Table 1[4,10-13].Most cases can be classified on the basis of the new classification.There have been 22 cases of Type A,8 cases of Type B1,46 cases of Type B2,10 cases of Type C,2 cases of triple appendix,and 14 cases of horseshoe appendix reported as of the beginning of 2018[3,4].Although the duplex appendix is rare,surgeons should suspect the possibility of it when performing an appendectomy to prevent adverse consequences and medical disputes.In addition,a differential diagnosis is also necessary,including Meckel's diverticulum,colonic tumor,gastroenteritis,congenital cecal diverticulum,intussusceptions,and inflammatory bowel disease[14].In the presence of a duplex appendix,the possibility of other congenital malformations should be further explored,especially in cases of Type B1 and Type C.However,Type B2,which is the most common variety and the most likely to be misdiagnosed or mismanaged,is unrelated to any other congenital anomalies[3].

Figure 2 lntraoperative photograph of the patient.
In the classification of duplex appendix,the horseshoe appendix is a rarer congenital malformation.In 1989,Meskoet al[15]first depicted the horseshoe appendix.Through a review of the literature,14 patients with horseshoe appendix have been reported to date[4],and as per our knowledge,our patient was the 15th patient with a reported horseshoe appendix.The etiology and pathogenesis of horseshoe appendix are still unclear because there are extremely limited cases that have been reported thus far.Currently,some theories have been proposed to explain how the horseshoe appendix forms[16].First,the horseshoe appendix may form by the mutual fusion between the tip of the normal appendix and that of the abnormal appendix.Second,a horseshoe appendix may develop from the fusion between the tip of the appendix and another part of the cecum,which then becomes the second base.Third,in the embryonic period,the base of the appendix split into two parts,each of which develops continuously,resulting in two bases that are also single structures.However,the first two theories do not seem to explain why both appendixes are supplied by a single blood vessel in the mesoappendix,and its branches fan out instead of forming an arcade.The study of the formation mechanism of the duplex appendix revealed that a “transient appendix” at the terminus of the cecum,which was distinct from the normal appendix,was observed during the 6th week of embryonic development and atrophy at the 7th week[17].If the transient appendix does not disappear,a duplex appendix may form.Additionally,the horseshoe appendix,a subtype of the duplex appendix,may be caused by some abnormalities in the embryonic period.Therefore,the third theory is most likely to explain the formation of a horseshoe appendix.However,more research is needed to support this theory,because of the limited number of cases.
The horseshoe appendix can be divided into two types according to the following new classification system (Table 1):Frontal type,in which both bases of the appendix are not on the tenia,and sagittal type,in which the bases are along the tenia[11].The malformation of our patient was a horseshoe type with a frontal location.In addition,we must simultaneously pay attention to whether the patient had other malformations because genitourinary,other intestinal,or vertebral malformations have been observed in cases with a duplex appendix.Fortunately,other associated congenital anomalies had not been observed in our patient,except for the endometriosis of the small intestine and ovary.Preoperative diagnosis is extremely difficult,whether it is a horseshoe appendix or other types of duplex appendix.It has been reported that[4]ultrasound and three-dimensional reconstruction may be helpful for the preoperative diagnosis of a horseshoe appendix,but most cases are accidentally discovered during surgery,and only two patients had a clear diagnosis before surgery.In our patient,imaging failed to preoperatively diagnose appendiceal anomalies.However,after surgery,we reviewed the CT scan repeatedly,and the images showed that there were two free fecaliths at the root of the appendix,which may indicate the presence of a duplex appendix (Figure 1).This finding was easily ignored.
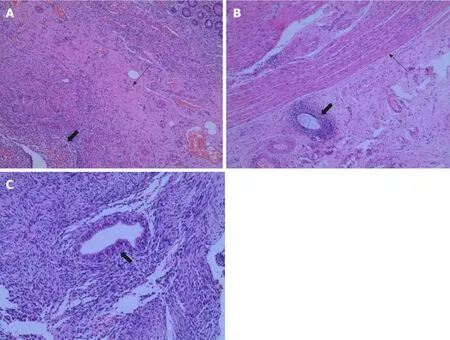
Figure 3 Histopathological appearances of the endometriosis in appendix,small intestine,and ovary.
Endometriosis,which is defined as the growth of endometrial glands and stroma outside the uterine cavity,is a fairly common disease that affects up to 15% of women in childbearing age.Von Rokitansky first described endometriosis in 1860[18].Several theories have been proposed to explain the pathogenesis of endometriosis,including retrograde menstruation and implantation theory,coelomic metaplasia theory,lymphovascular spread theory,direct transplantation and dissemination theory,and the cellular immunity theory which was a newly developed theory[19-21].However,the specific etiology of endometriosis is still unclear.A variety of factors potentially contribute to the disease.Endometriosis can occur anywhere in the body,including pelvis organs,gastrointestinal tract,and pleural and pericardial cavities,but the ambilateral adnexa is the most frequent.Once involving the gastrointestinal tract,endometriosis also commonly involves the recto-sigmoid (72%),recto-vaginal septum(13%),small intestine (7%),cecum (3.6%),and appendix (3%)[18].Endometriosis of the appendix is a rare disease,and its overall incidence ranges between 0.02% and 36.6%,which is widely variable and depends on the population being evaluated[22].Our patient not only had rare appendix and ileum involvement but also had a duplex appendix.This dual participation has not been observed thus far.
Clinically,the symptoms of endometriosis are diverse and have been determined by the site of occurrence.Endometriosis of the appendix is usually asymptomatic,but it may also cause acute or chronic pelvic pain,appendicitis,lower gastrointestinal hemorrhage,and intussusception[19,22].Consistent with some reports (Table 2)[19,23-27],our patient also presented the symptoms of acute appendicitis.Moreover,laparoscopic exploration also showed the presence of bloody fluid in the abdominal cavity.The hemoperitoneum is likely to be related to menstruation,because in these reports (Table 2),patients presented the symptoms of acute appendicitis during the menstrual period.As our patient presented the symptoms of appendicitis on the 5th day after the end of menstruation,we assume it to be related to the appendiceal fecalith.The occurrence of acute appendicitis may be the result of the dual effects of endometriosis and appendiceal fecalith.Moreover,our patient had a history ofrepeated lower abdominal pain which was associated with menstruation,consistent with some reports[23,26,27].It suggests that hemoperitoneum and chronic abdominal pain may be important signs of endometriosis diagnosis,which further validates the theory of retrograde menstruation.Additionally,gastrointestinal endometriosis can present with episodes of abdominal pain,change in bowel habits,abdominal distention,rectal bleeding,and intestinal obstruction[28-30].Fortunately,although small intestinal endometriosis in our case was asymptomatic,it did not cause intestinal obstruction due to timely detection.
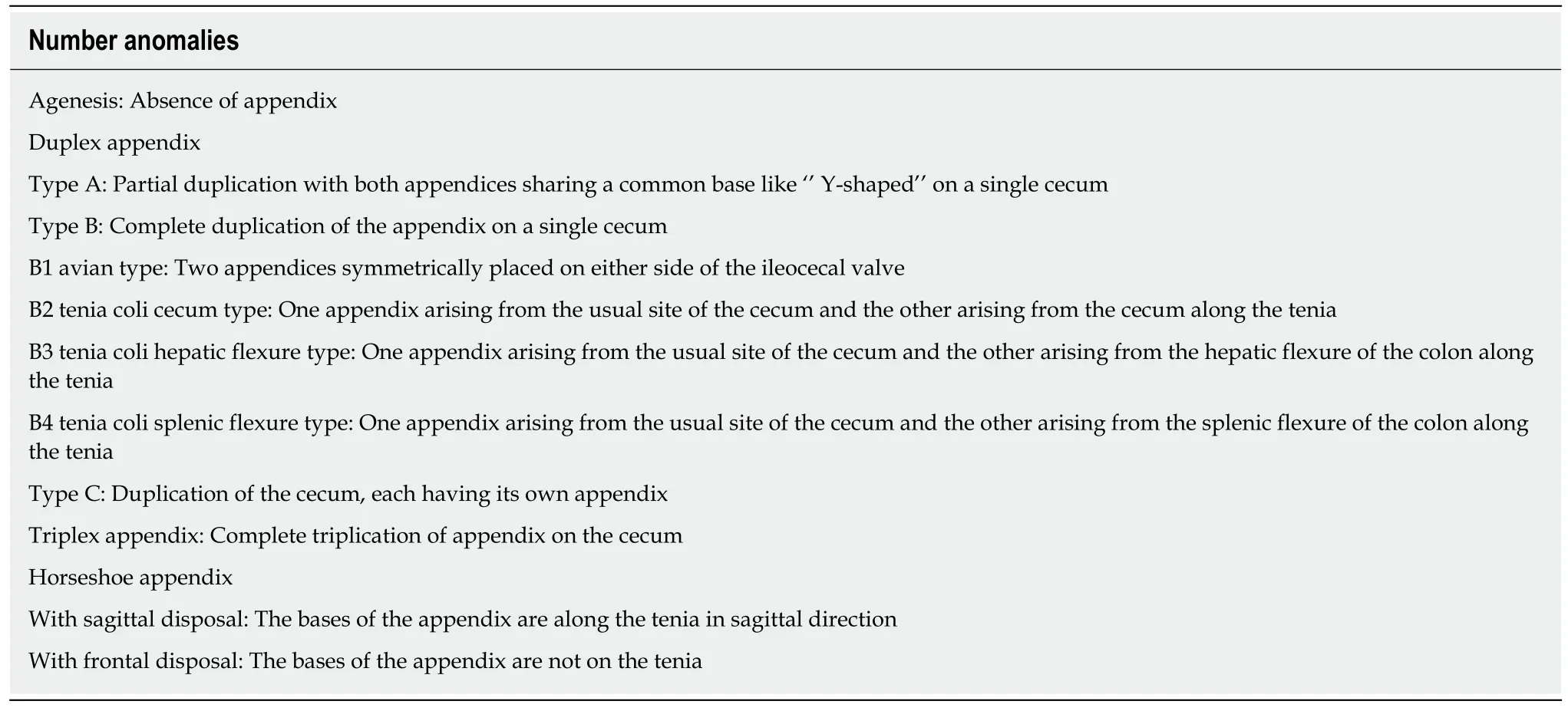
Table 1 New classification of appendiceal anomalies
The clinical manifestations of endometriosis are usually nonspecific,leading to the diagnostic dilemma.Therefore,complete preoperative examination is needed,including CT scan,magnetic resonance imaging (MRI),abdominal ultrasonography,and laboratory examination.It was reported that[31]multislice CT has a great potential for detecting alterations in the intestinal wall,especially when combined with enteroclysis.MRI has a high sensitivity (77%-93%) in the diagnosis of bowel endometriosis[32].Unfortunately,there is currently no gold standard for the imaging diagnosis of endometriosis[20].The serum CA125 level,which has been used to monitor the progress of endometriosis,may be a useful diagnostic indicator[33].However,it has also been reported that CA125 is not sensitive enough to the diagnosis of endometriosis[30].In our patient,the abdominal CT scan did not suggest endometriosis,but she had a high preoperative serum CA125 level of 69.5 U/mL.Therefore,we believe that the presence of endometriosis needs to be suspected when patient have elevated serum CA125 levels.Additionally,except for the hemoperitoneum we have mentioned above,blueberry spot of the peritoneum and nodularity of the appendix may also indicate the presence of endometriosis during surgery[19,23].Intraoperatively,we only found moderate hemorrhagic peritoneal fluid in our patient.However,the postoperative pathology of our patient confirmed the presence of endometriosis in the appendix,small intestine,and ovary.Therefore,laparoscopy and pathological confirmation remain the gold standard for the diagnosis of endometriosis.Given the nature of endometriosis,patients such as ours should be encouraged to refer to gynecologists for further assessment of the extent of endometriosis and for postoperative follow-up.
CONCLUSION
Acute appendicitis is a common abdominal disease.Although duplex appendix is rare,especially the horseshoe appendix,surgeons who may not encounter it throughout their careers need to be aware of the possibility of it when performing an appendectomy.In particular,preoperative CT showed two separate fecaliths at the root of the appendix,which may be a useful sign for the diagnosis of a duplex appendix.Therefore,a detailed exploration of the cecal pole and retrocecal space is encouraged to avoid misdiagnosis during surgery; misdiagnosis of appendixduplication may result in a poor clinical outcome and law dispute.In addition,women of childbearing age who have chronic pelvic pain or elevated CA125 levels need to highly suspect the possibility of endometriosis.In summary,whether laparoscopy or laparotomy is used,careful exploration of the entire abdomen is crucial and occasionally surprises us.
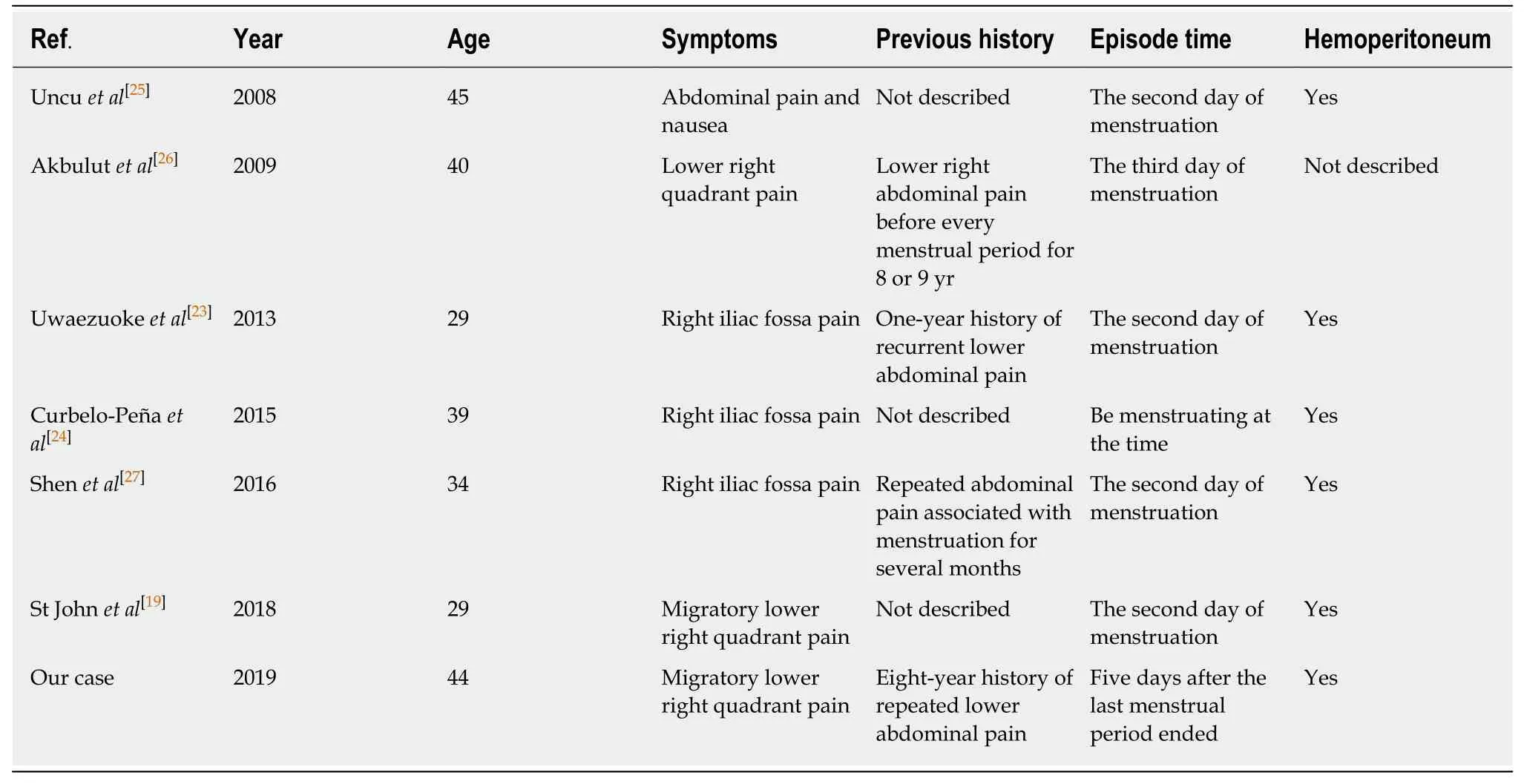
Table 2 Clinical features of patients with appendix endometriosis
ACKNOWLEDGEMENTS
We wish to acknowledge Wen-Yan Shen (Department of Pathology,The Second Affiliated Hospital of Jiaxing University,Jiaxing) for her support on this case.
杂志排行
World Journal of Clinical Cases的其它文章
- Percutaneous coronary intervention for ostial lesions of the left main stem in a patient with congenital single left coronary artery: A case report
- Common iliac artery occlusion with small intestinal transection caused by blunt abdominal trauma: A case report and review of the literature
- c.753_754delAG,a novel CFTR mutation found in a Chinese patient with cystic fibrosis: A case report and review of the literature
- Fever and neck pain after pacemaker lead extraction: A case report
- Gastric duplication cyst mimicking large cystic lymphangioma in an adult: A rare case report and review of the literature
- Oncogenic osteomalacia caused by a phosphaturic mesenchymal tumor of the femur: A case report