血浆同型半胱氨酸及白细胞水平与终末期肾病患者合并主动脉夹层的相关性研究
2019-02-11谢家和谢龙胡育华
谢家和 谢龙 胡育华

[摘要]目的 探討血浆同型半胱氨酸及白细胞(WBC)水平与终末期肾病(ESRD)患者合并主动脉夹层(AD)的关系。方法 回顾性分析2011年1月~2018年12月在赣南医学院第一附属医院与赣州市人民医院诊断为AD的125例患者的临床资料,其中ESRD合并AD 22例(作为ESRD夹层组),分别为肾性ESRD 16例,糖尿病ESRD 2例,高血压ESRD 4例;肾功能正常的AD 103例(作为肾功能正常夹层组)。检测两组患者的血浆同型半胱氨酸(Hcy)、血肌酐(SCr)、肾小球滤过率(GFR)、WBC水平,并分析Hcy与SCr、GFR及WBC的关系。结果 ESRD夹层组患者的SCr、Hcy水平分别为(927.72±465.30)、(23.89±12.16)μmol/L,均明显高于肾功能正常夹层组的(76.71±16.51)、(16.79±9.32)μmol/L,差异有统计学意义(P<0.05)。ESRD夹层组患者的GFR及WBC水平分别为(9.93±9.01)ml/(min·1.73 m2)、(8.05±2.94)×109/L,均明显低于肾功能正常夹层组的(106.33±15.06)ml/(min·1.73 m2)、(10.89±3.55)×109/L,差异有统计学意义(P<0.05)。相关性分析结果显示,Hcy与SCr成正相关(r=0.18,P<0.05),GFR与Hcy成负相关(r=-0.24,P<0.01),WBC计数与Hcy无相关性(r=0.04,P=0.62)。结论 血浆高Hcy可能参与ESRD患者AD的发生,提示降低Hcy水平可能成为预防ESRD患者发生AD的一个有效措施。
[关键词]同型半胱氨酸;终末期肾病;主动脉夹层;炎症;肾功能
[中图分类号] R543.1 [文献标识码] A [文章编号] 1674-4721(2019)12(a)-0004-04
Study on the correlation between plasma homocysteine and white blood cell levels and aortic dissection in patients with end-stage renal disease
XIE Jia-he1,2 XIE Long3 HU Yu-hua4 LI Qing-rui4 LIU Yong-sheng5 ZHONG Yi-ming1,2 XIE Dong-ming1,2▲
1. Department of Cardiology, the First Affiliated Hospital of Gannan Medical University, Jiangxi Province, Ganzhou 341000, China; 2. Key Laboratory of Cardiovascular and Cerebrovascular Disease Prevention and Control Ministry of Education, Gannan Medical University, Jiangxi Province, Ganzhou 341000, China; 3. Department of Geriatrics, People′s Hospital of Ganzhou City, Jiangxi Province, Ganzhou 341000, China; 4. School of Graduate, Gannan Medical University, Jiangxi Province, Ganzhou 341000, China; 5. Ruijin People′s Hospital, Jiangxi Province, Ruijin 342500, China
[Abstract] Objective To explore the relationship between plasma homocysteine and white blood cell (WBC) levels and aortic dissection (AD) in patients with end-stage renal disease (ESRD). Methods The clinical data of 125 patients with AD diagnosed in the First Affiliated Hospital of Gannan Medical University and People′s Hospital of Ganzhou City from January 2011 to December 2018 were retrospectively analyzed. There were 22 cases of ESRD with AD (used as the ESRD dissection group), including 16 cases of kidney disease related to ESRD, 2 cases of diabetes mellitus related to ESRD, 4 cases of hypertension related to ESRD, and the remaining 103 cases were patients with normal renal function combined with AD (used as the normal renal function dissection group). The plasma homocysteine (Hcy), serum creatinine (SCr), glomerular filtration rate (GFR), and WBC levels were measured in both groups and the relationship between Hcy and SCr, GFR, WBC was analyzed. Results The levels of SCr and Hcy in the ESRD dissection group were (927.72±465.30) and (23.89±12.16) μmol/L, respectively, which were significantly higher than those in the normal renal function dissection group for (76.71±16.51) and (16.79±9.32) μmol/L, and the differences were statistically significant (P<0.05). The GFR and WBC levels in the ESRD dissection group were (9.93±9.01) ml/(min·1.73 m2) and (8.05±2.94)×109/L, respectively, which were significantly lower than those in the normal renal function dissection group for (106.33±15.06) ml/(min·1.73 m2), (10.89±3.55)×109/L, and the differences were statistically significant (P<0.05). Correlation analysis showed that Hcy was positively correlated with SCr (r=0.18, P<0.05), GFR was negatively correlated with Hcy (r=-0.24, P<0.01), and WBC count was not correlated with Hcy (r=0.04, P=0.62). Conclusion High plasma Hcy may be involved in the occurrence of AD in patients with ESRD, suggesting that lowering Hcy levels may be an effective measure to prevent AD in patients with ESRD.
[Key words] Plasma homocysteine; End-stage renal disease; Aortic dissection; Inflammation; Renal function
终末期肾病(end-stage renal disease,ESRD)是指肾脏结构或功能异常≥3个月,肾小球滤过率(glomerular filtration rate,GFR)<15 ml/(min·1.73 m2)。ESRD患者较肾功能正常人群并发心血管疾病风险显著增加,已严重影响患者的生存及预后[1-2]。主动脉夹层(aortic dissection,AD)是指主动脉壁内膜破裂,导致假腔和/或壁内血肿的形成及相应器官血流灌注受损,严重者可因动脉壁的破裂导致患者急性死亡[3-4]。近年来,ESRD并发AD的患者不断增多,但还尚不清楚其与肾功能正常AD患者之间有何异同点及其可能的机制。
高同型半胱氨酸血症(hyperhomocysteinemia,HHcy)及血管炎症是心血管疾病发生的独立危险因素[5-7]。相关研究表明,ESRD患者血浆同型半胱氨酸(Hcy)及炎症水平显著增高[8-9]。但Hcy是否参与ESRD患者合并AD的发生,目前不清楚。本研究通过比较ESRD合并AD患者与肾功能正常的AD患者之间血浆Hcy及白细胞(WBC)等指标水平差异,以期为认识ESRD合并AD的发病机制及改善患者预后提供新的依据,现报道如下。
1资料与方法
1.1一般资料
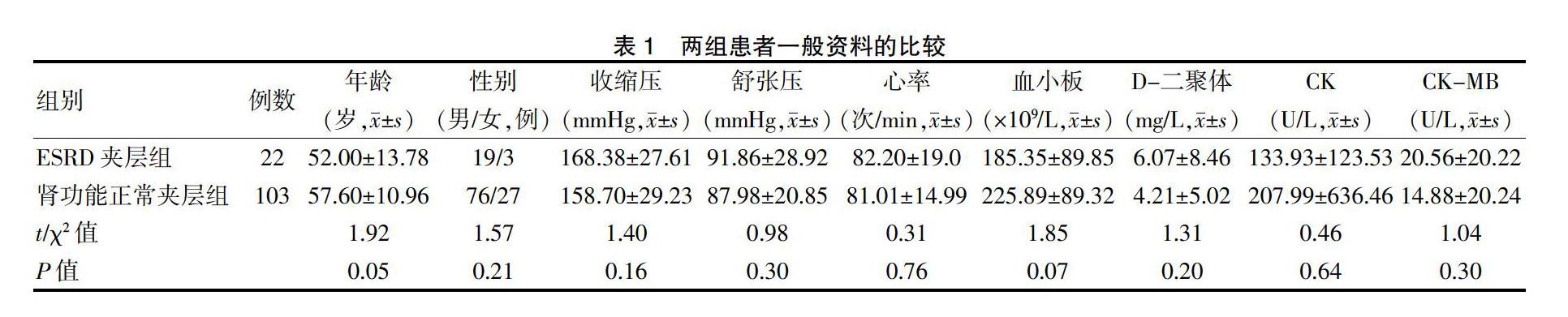
回顾性分析2011年1月~2018年12月在赣南医学院第一附属医院与赣州市人民医院经影像学明确诊断为AD的125例患者的临床资料。AD定义及诊断标准:AD指主动脉内膜破裂,血液从内膜撕裂处进入主动脉中膜,使内膜与中膜分离,形成主动脉真假腔,其诊断主要通过主动脉增强CT或磁共振等影像學技术;ESRD的定义及诊断标准:肾功能结构或功能异常≥3个月,GFR≤15 ml/(min·1.73 m2)。排除标准:服用维生素、叶酸患者;合并恶性肿瘤、甲状腺功能减退患者;合并马方(Marfan)综合征等先天性主动脉血管病变患者。其中ESRD合并AD 22例(作为ESRD夹层组),分别为肾性ESRD 16例,糖尿病ESRD 2例,高血压ESRD 4例;肾功能正常的AD 103例(作为肾功能正常夹层组)。两组患者的年龄、性别、收缩压、舒张压、心率、血小板、D-二聚体、肌酸激酶(CK)及肌酸激酶同工酶(CK-MB)等一般资料比较,差异无统计学意义(P>0.05)(表1),具有可比性。本研究经赣南医学院第一附属医院医学伦理委员会批准,所有患者对诊治均知情同意并签署了知情同意书。
1.2方法
1.2.1临床资料数据收集 收集入选患者的年龄、性别、血压(收缩压、舒张压)、心率、合并疾病等信息。
1.2.2血液标本收集及指标测定 所有患者空腹8~12 h,抽取静脉血行血浆Hcy、血小板、D-二聚体、CK、CK-MB、血肌酐(SCr)、GFR等生化指标检测,具体操作由赣南医学院第一附属医院检验科完成,操作步骤参考检测仪器及试剂盒说明书。
1.3观察指标
比较两组患者的Hcy、SCr、WBC、GFR指标水平,并对各指标之间的相关性进行分析。
1.4统计学方法
采用SPSS 20.0及GraphPad Prism 5.0软件统计学软件进行数据分析,符合正态分布的计量资料采用均数±标准差(x±s)表示,两组间比较采用t检验,不符合正态分布者转换为正态分布后行统计学分析;计数资料用率(%)表示,组间比较采用χ2检验;相关性分析采用直线回归分析,以P<0.05为差异有统计学意义。
2结果
2.1两组患者实验室指标水平的比较
ESRD夹层组患者的SCr、Hcy水平均明显高于肾功能正常夹层组,差异有统计学意义(P<0.05);ESRD夹层组患者的GFR及WBC水平均明显低于肾功能正常夹层组,差异有统计学意义(P<0.05)(表2)。
2.2相关性分析
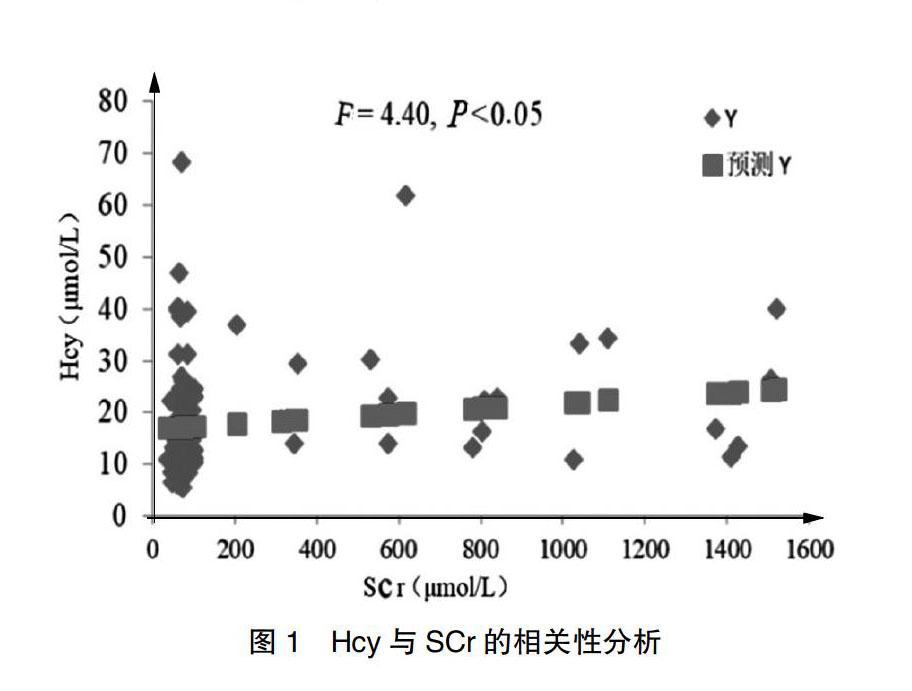
2.2.1 Hcy与SCr的相关性分析 患者血浆Hcy与SCr成正相关(r=0.18,F=4.40,P<0.05),直线回归方程为Y=16.91X-0.005(图1)。
2.2.2 Hcy与GFR的相关性分析 患者血浆Hcy与GFR成负相关(r=-0.24,F=7.45,P<0.01),直线回归方程为Y=23.56X+0.06(图2)。
2.2.3血浆WBC计数与Hcy的相关性分析
患者血浆WBC计数与Hcy无相关性(r=0.04,F=0.25,P=0.62),直线回归方程为Y=10.68X+0.01(图3)。
3讨论
近年来,随着人口老龄化及肾脏替代治疗技术的发展,ESRD患病人数及并发心血管疾病的风险也显著增加,已严重影响患者的预后,而继发AD是其最严重并发症之一[10]。目前临床上对ESRD患者预防AD的发生除控制血压外尚缺乏有效的措施。因此,探索ESRD患者AD的发生因素及机制对其防治具有重要意义。高Hcy是指血液中Hcy≥15 μmol/L,其在肾功能正常AD患者中的作用已有研究报道,认为高Hcy会导致AD的发生[11]。此外,HHcy是自发性颅内AD和Marfan综合征患者继发AD的重要危险因素[12-13]。但是目前尚不清楚Hcy在ESRD患者继发AD中的影响。本研究结果显示,ESRD合并AD患者的血浆Hcy水平较肾功能正常AD患者显著升高,差异有统计学意义(P<0.05),提示高Hcy可能在ESRD患者AD的发病中发挥作用。
既往研究表明,炎症是AD发生的重要机制,血管壁浸润的炎症细胞可以触发炎症反应及增加基质金属蛋白酶(MMP)的分泌,从而导致弹性纤维降解及动脉壁中层结构破坏,最终促使AD的形成[14]。此外,大量的研究已证实,促炎因子可以促使AD形成,而抗炎因子可以抑制AD的扩张[15-16]。同样,高Hcy通过促使血管炎症反应,导致动脉粥样硬化,其机制与Hcy激活NLRP 3炎症小体,并介导巨噬细胞增加促炎因子白介素-1β(IL-1β)和白介素-18(IL-18)等表达有关[17]。
本研究结果显示,ESRD合并AD患者的血浆WBC水平低于肾功能正常AD患者,差异有统计学意义(P<0.05),提示炎症与ESRD患者AD的形成关系可能不密切。氧化应激异常是ESRD的重要病生特征,其可以損伤血管内皮细胞,破坏血管结构[1,18]。同时,活性氧自由基过多的产生也是AD形成的重要病生机制[19]。此外,有研究报道高Hcy可通过激活NADPH氧化酶加重血管损伤,导致腹主动脉瘤形成[20]。推测氧化应激等机制可能在ESRD患者AD发生中发挥重要作用,具体机制需要后续研究进一步求证。本研究结果还提示,相关性分析结果显示,Hcy与SCr成正相关(r=0.18,P<0.05),GFR与Hcy成负相关(r=-0.24,P<0.01),WBC计数与Hcy无相关性(r=0.04,P=0.62)。
综上所述,血浆高Hcy在ESRD患者AD发生中可能有重要作用,其机制可能与高Hcy诱发的机体氧化应激失衡等因素有密切联系,提示降低ESRD患者的血浆Hcy水平可能成为预防包括AD在内的心血管疾病的一个有效措施。
[参考文献]
[1]Duni A,Liakopoulos V,Rapsomanikis KP,et al.Chronic Kidney disease and disproportionally increased cardiovascular damage:Does oxidative stress explain the burden?[J].Oxid Med Cell Longev,2017,2017:9 036 450.
[2]Ronco C,Bellasi A,Di Lullo L.Cardiorenal syndrome:An overview[J].Adv Chronic Kidney Dis,2018,25(5):382-390.
[3]Melvinsdottir IH,Lund SH,Agnarsson BA,et al.The incidence and mortality of acute thoracic aortic dissection:results from a whole nation study[J].Eur J Cardiothorac Surg,2016,50(6):1111-1117.
[4]Parve S,Ziganshin BA,Elefteriades JA.Overview of the current knowledge on etiology,natural history and treatment of aortic dissection[J].J Cardiovasc Surg(Torino),2017,58(2):238-251.
[5]Leng YP,Ma YS,Li XG,et al.l-Homocysteine-induced cathepsin V mediates the vascular endothelial inflammation in hyperhomocysteinaemia[J].Br J Pharmacol,2018,175(8):1157-1172.
[6]Ganguly P,Alam SF.Role of homocysteine in the development of cardiovascular disease[J].Nutr J,2015,14:6.
[7]Holtzman JL.The role of low levels of the serum glutathione-dependent peroxidase and glutathione and high levels of serum homocysteine in the development of cardiovascular disease[J].Clin Lab,2002,48(3-4):129-130.
[8]Ferechide D,Radulescu D.Hyperhomocysteinemia in renal diseases[J].J Med Life,2009,2(1):53-59.
[9]Malecki R.Hyperhomocysteinemia as a risk factor for cardiovascular diseases in patients with chronic renal failure[J].Pol Arch Med Wewn,2000,104(4):695-701.
[10]Schiffrin EL,Lipman ML,Mann JF.Chronic kidney disease:effects on the cardiovascular system[J].Circulation,2007, 116(1):85-97.
[11]Sbarouni E,Georgiadou P,Analitis A,et al.High homocysteine and low folate concentrations in acute aortic dissection[J].Int J Cardiol,2013,168(1):463-466.
[12]Luo H,Liu B,Hu J,et al.Hyperhomocysteinemia and methylenetetrahydrofolate reductase polymorphism in cervical artery dissection:a meta-analysis[J].Cerebrovasc Dis,2014,37(5):313-322.
[13]Jiménez-Altayó F,Meirelles T,Crosas-Molist E,et al.Redox stress in Marfan syndrome: Dissecting the role of the NADPH oxidase NOX4 in aortic aneurysm[J].Free Radic Biol Med,2018,118:44-58.
[14]Nienaber CA,Clough RE,Sakalihasan N,et al.Aortic dissection[J].Nat Rev Dis Primers,2016,2:16 053.
[15]Xu H,Du S,Fang B,et al.VSMC-specific EP4 deletion exacerbates angiotensin Ⅱ-induced aortic dissection by increasing vascular inflammation and blood pressure[J].Proc Natl Acad Sci U S A,2019,116(17):8457-8462.
[16]Yoshida S,Yamamoto M,Aoki H,et al.STAT3 activation correlates with adventitial neutrophil infiltration in human aortic dissection[J].Ann Vasc Dis,2019,12(2):187-193.
[17]Wang R,Wang Y,Mu N,et al.Activation of NLRP3 inflammasomes contributes to hyperhomocysteinemia-aggravated inflammation and atherosclerosis in apoE-deficient mice[J].Lab Invest,2017,97(8):922-934.
[18]Duni A,Liakopoulos V,Roumeliotis S,et al.Oxidative stress in the pathogenesis and evolution of chronic kidney disease:untangling Ariadne′s thread[J].Int J Mol Sci,2019,20(15):E3711.
[19]Timkova V,Tatarkova Z,Lehotsky J,et al.Effects of mild hyperhomocysteinemia on electron transport chain complexes,oxidative stress,and protein expression in rat cardiac mitochondria[J].Mol Cell Biochem,2016,411(1-2):261-270.
[20]Liu Z,Luo H,Zhang L,et al.Hyperhomocysteinemia exaggerates adventitial inflammation and angiotensin II-induced abdominal aortic aneurysm in mice[J].Circ Res,2012,111(10):1261-1273.
(收稿日期:2019-08-06 本文編辑:任秀兰)
