Effects of Maixuekang Capsules Combined with Edaravone on Serum MMP-9, S-100β Protein Levels and Neurological Functions in Patients with Hemorrhagic Cerebral Infarction
2019-01-24ZhangJianqiang张建强JiaoYongping焦永平
Zhang Jianqiang (张建强), Jiao Yongping (焦永平)
aDepartment of Neurology, First Affiliated Hospital of Henan University of Science and Technology, Luoyang 471003, China
bDepartment of Neurology, Linying People's Hospital, Luohe 462600, China
ABSTRACT
OBJECTIVE: To investigate the effects of Maixuekang Capsules combined with edaravone on serum matrix metalloproteinase-9 (MMP-9), S-100β protein levels and neurological functions in patients with hemorrhagic cerebral infarction. METHOSDS: A total of 76 patients with hemorrhagic cerebral infarction treated in the First Affiliated Hospital of Henan University of Science and Technology from January 2017 to May 2018 were selected and were randomly divided into treatment group and control group, with 38 patients in each group. The control group was given edaravone, and the treatment group was given Maixuekang Capsules on the basis of the control group. The clinical efficacy, serum MMP-9 and S-100β protein levels, neurological function recovery, activity of daily living and incidence rate of adverse reactions were compared between the 2 groups. RESULTS: The total effective rate of the treatment group was 92.11%, which was higher than 71.05% of the control group (P < 0.05); the National Institutes of Health Stroke Scale(NIHSS) score in the 2 groups decreased (P < 0.05), and the Activity of Daily Living Scale (ADL) score increased(P < 0.05), the improvement of the above 2 scores in the treatment group were better than those in the control group(P < 0.05); the level of MMP-9 was gradually decreasing in the 2 groups, on the 7th day, 14th day after treatment, and the levels of MMP-9 decreased significantly (P < 0.05), and the treatment group was lower than the control group at all time points (P < 0.05); on the 3rd day after treatment, the levels of S-100β protein in the 2 groups increased significantly(P < 0.05); on the 7th day, 14th day after treatment, the levels of S-100β protein in the two groups decreased significantly(P < 0.05), and the treatment group was significantly lower than the control group (P < 0.05); there was no significant difference in incidence rate of adverse reactions between 7.89% in the control group and 5.26% in the treatment group (P > 0.05). CONCLUSION: The combination of Maixuekang Capsules and edaravone is effective in treating hemorrhagic cerebral infarction, and it can significantly improve neurological function defect and daily living ability,reduce serum MMP-9 and S-100β protein levels, and has higher safety.
KEYWORDS: Maixuekang Capsules; Edaravone; Hemorrhagic cerebral infarction; Matrix metalloproteinase-9;S-100β protein; Neurological function
There are two types of cerebral infarction:hemorrhagic infarction and ischemic infarction.Hemorrhagic infarction (HI), also known as cerebral hemorrhage after cerebral infarction[1], refers to a kind of disease of posthemorrhage in infarction area caused by the recovering perfusion of vessels in ischemic area during infarction period. The major pathogenic factors are cardiogenic cerebral embolism and large area of atherosclerosis cerebral infarction. Clinical manifestations are: headache and vertigo, nausea and vomiting, consciousness disturbance, ataxia, hemiplegia,hemianopsia, etc., usually accompanied with pulmonary infection, hemorrhage of digestive tract, anxiety and depression, etc., which place heavy burden on patients and their families[2]. Edaravone has been used in treating hemorrhagic infarction in the past clinical practice,while its efficacy is poor; and further study has found that Maixuekang Capsules also has curative effects on hemorrhagic infarction[3]. Therefore, this study used Maixuekang Capsules on the basis of edaravone,aiming to achieve a better curative effect through this combination. Here is the report.
MATERIALS AND METHODS
General materials
The research subjects were 76 patients with hemorrhagic infarction treated in First Affiliated Hospital of Henan University of Science and Technology from January 2017 to May 2018, all conforming to the diagnosis standards of hemorrhagic infarction revising in the 4thacademic conference on cerebrovascular disease[4].All patients were randomly divided into treatment group and control group, with 38 cases in each group. There were 20 males and 18 females in treatment group aged from 44 to 74 years old, with an average age of 62.48 ± 6.18 years old, and the time after infarction from 3 to 24 h, and 13.56 ± 2.25 h on average. And there were 22 patients whose lesion location was in basal ganglia, 10 in temporal occipital, and 6 in cerebellum. The bleeding volume was 5-28 mL, with 15.78 ± 5.52 mL on average. There were 21 males and 17 females in treatment group aged from 44 to 74 years old, with an average age of 62.36 ± 6.11 years old, and the time after infarction from 3-21 h, and 12.16 ± 3.15 h on average. And there were 23 patients whose lesion location was in basal ganglia, 10 in temporal occipital, and 5 in cerebellum. The bleeding volume was 7-30 mL, with 16.18 ± 4.82 mL on average. The general clinical materials of the two groups including gender, age,disease time, lesion location, and bleeding volume, etc. were compared and the differences had no statistical significance(P > 0.05), which meant the two groups have comparability.
Inclusion criteria
(1) Patients who accorded with the above diagnosis standards of hemorrhagic infarction were inluded. (2)Hemorrhagic infarction was confirmed through the examination of CT and MRI. (3) Bleeding volume was no more than 30 mL. (4) It was the first time of all the patients to have such attack. The time after attack was no more than 24 h. And the bleeding didn't enter ventricle. (5)According with the requirements of medical ethics, the informed consent was voluntarily signed by patients and their families.
Exclusion criteria
(1) Patients with organic cerebral diseases like concurrent cerebral tumor were excluded. (2) Patients with severe dysfunction of kernel, hepatic, and renal system were excluded. (3) Patients who were with anaphylaxis to medications in this study were excluded.(4) Patients with blood coagulation dysfunction were excluded. (5) Patients with serious mental disorder and incapable to cooperate with the treatment were excluded.
Methods
Basic therapy including electrocardiogram (ECG)monitoring, dehydration, oxygen inhalation, blood pressure control, water and electrolyte balance were used in two groups of patients. The dilution solution with 20 mg edaravone injection (made by Nanjing Simcere Pharmaceutical Co. LTD, SFDA: H20050280, specification:20 mL:30 mg) and 100 mL physiological saline was used in control group through intravenous drip in 30 minutes on the basis of basic therapy twice a day for continuous 2 weeks. Maixuekang Capsules (made by Chongqing Dopt Pharmaceutical Co. LTD, SFDA: Z10970056,specification: 0.25 g) was used in treatment group three capsules each time and three times a day for continuous 2 weeks on the basis of the treatment in control group.
Criterion of clinical effects
Clinical effects of patients in 2 groups were evaluated according to National Institute of Health Stroke Scale (NIHSS)[5]and Modified Rankin Score (mRS)[6].Recovery: the decline of NIHSS score was no less than 90%, and the disabled degree of mRS was 0. Markedly effective: the decline of NIHSS score was no less than 45%, and the disabled degree of mRS was 1. Effective:the decline of NIHSS score was no less than 18% and less than 45%, and the disabled degree of mRS was 2-3.Ineffective: the decline of NIHSS score was less than 18%, and the disabled degree of mRS was 4-5. Total effective rate = recovery rate + markedly effective rate +effective rate.
Observation index
(1) Neurological function: NIHSS was used to evaluate the defect degree of patients' neurological function before and after the treatment, including 11 items like the level of consciousness, visual field, starring, facial palsy, sensation, language, etc., and the score ranged from 0 to 42 points. The higher the score was, the severer the defect of patients' neurological function was. (2) Daily living activity: Activity Daily Living Scale (ADL)[7]was used to evaluate patients' daily living activity before and after the treatment with 100 points in total. The higher thescore was, the better the recovery of patients' daily living activity was. (3) Changes of MMP-9 and S-100β protein level: patients' fasting venous blood was gathered and centrifuged with a speed of 3000 r/min for 15min before and after the treatment on the 3rd, 7th, 14thday after the treatment. The supernatant was reserved in temperature of -20℃. Enzyme Linked Immunosorbent Assay (ELISA)was used to detect the levels of MMP-9 and S-100β in serum strictly according to the instructions.

Table 1. Clinical effects comparison (%)
Adverse reactions
Adverse reactions including dizziness, nausea and vomiting in the patients of the 2 groups were observed and recorded during the treatment.
Statistical methods
In this study, Software SPSS 23.0 was used to analyze data; inter-group and between-group comparison was made through t-test; percentage was used to express the counting data which was tested by χ2test. P < 0.05 indicated the difference was statistically significant.
RESULTS
Comparison of clinical effects
The total effective rate in treatment group (92.11%)was significantly higher than that (71.05%) of control group (P < 0.05). See Table 1.
Comparison of NIHSS and ADL score
The NIHSS score of both 2 groups decreased significantly after the treatment, while ADL score vitally increased (P < 0.05). The numerical difference in treatment group was significantly higher than control group (P < 0.05). See Table 2.
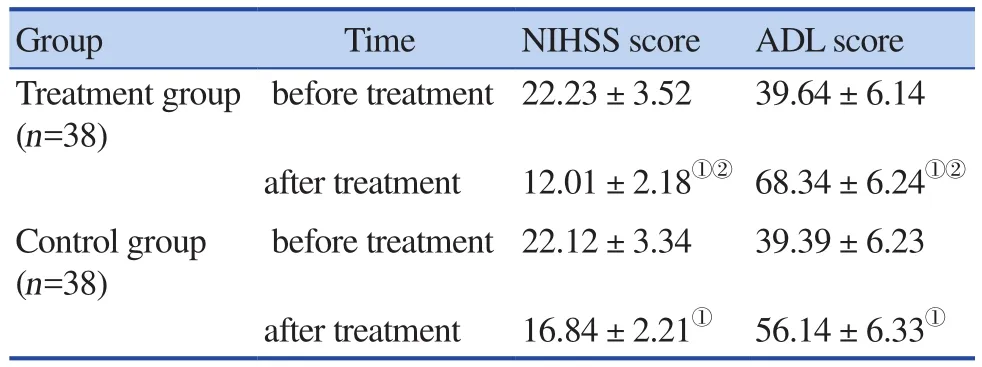
Table 2. Comparison of NIHSS and ADL score of before and after the treatment in 2 groups
The changes of MMP-9, S-100β level in serum
The level of MMP-9 and S-100β in 2 groups vitally decreased after the treatment. And on the 3rdday S-100β in the 2 groups increased after the treatment(P < 0.05).
There was no statistically significant difference between MMP-9 level on the 3rdday after the treatment and before the treatment. The levels of MMP-9, S-100β on the 7thand 14thday decreased significantly after the treatment (P < 0.05), and the treatment group was vitally lower than the control group (P < 0.05). See Table 3.
Comparison of adverse reactions
Control group: there was 1 case of hepaticdysfunction, 1 case of rash, 1 case of limbs weakness after medication with incidence rate of 7.89%. Treatment group:there was 1 case of rash, 1 case of limbs weakness with incidence rate of 5.26%. The incidence rate of 2 groups had no significant difference (x2=0.000, P = 1.000).
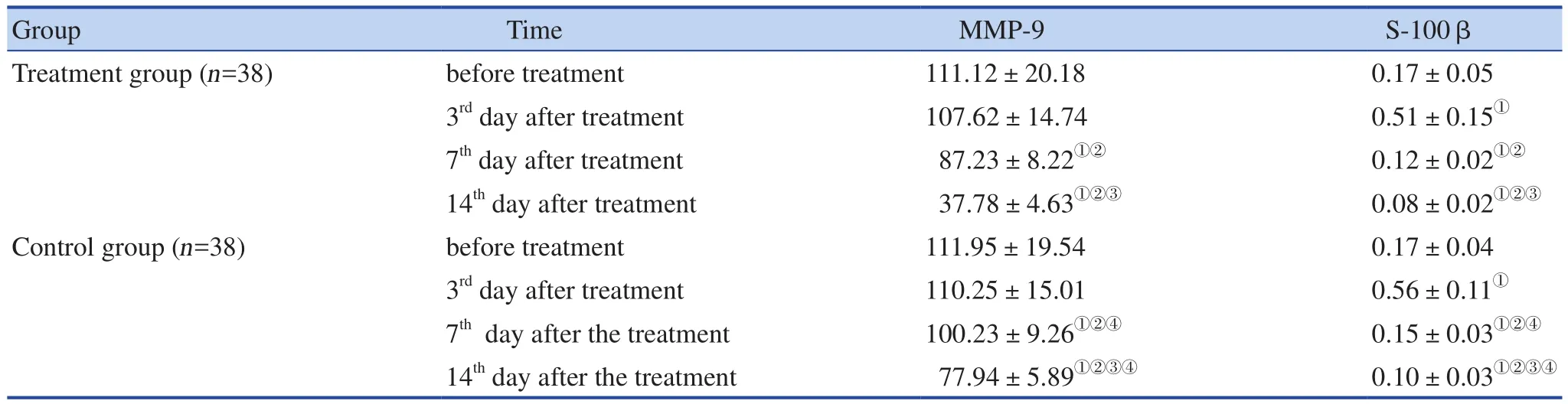
Table 3. The changes of MMP-9, S-100β level before and after the treatment (ng/mL)
DISCUSSION
Hemorrhagic cerebral infarction refers to a kind of disease of posthemorrhage in infarction area caused by the recovering perfusion of vessels in ischemic area during infarction period.. The main pathogeneses are[8]: (1) the recanalization of blocked vessels; (2)large area infarction or cerebral edema; (3) the flow of collateral circulation; (4) the fluctuation of hypertension,hyperglycemia and hyperlipidemia. The intracerebral hematoma caused by hemorrhagic infarction can directly stimulate and press surrounding cerebral tissues, leading to degeneration and necrosis of cerebral cells. Besides, it can also cause ischemia and anoxia of regional cerebral organization, which will further lead to degeneration or damage of neurological cells. Patients might have headache, dizziness, limb paralysis, etc., and some might also be in critical situation like consciousness disorder,central fever, and even brain hernia and death.
Hemorrhagic infarction in traditional Chinese medicine belongs to stasis syndrome or stroke, which mainly occurrs in middle-aged or aged people. As Jingyue's Complete Works puts, "aged people are weak... this syndrome will occur only beyond middle age. The book explains the disease mechanism as mutual stagnation of phlegm and stasis, deficiency of original qi and incitement between wind and fire, which can be briefly summarized as deficiency, phlegm, stasis,fire, qi, wind and blood. The deficiency of original qi is the root cause while other factors of phlegm, stasis,wind and fire are superficial causes, and the most basic is yin deficiency of liver and kidney. As is said in the 12thvolume of Root Cause of Stroke in Zabing Yuanliu Xizhu (the source and development of miscellaneous diseases), the deficiency of original qi is the root cause of stroke. Furthermore, blood stasis and phlegm are pathological products of deficiency of original qi which is unable to promote blood circulation due to the old age. Treatment should focus on eliminating blood stasis and phlegm, recovering original qi and resuscitation,aiming to achieve simultaneous treatment of root cause and symptoms[10].
Edaravone has been widely used on hemorrhagic infarction in past clinical practices. It is a kind of effective free-radical scavenger, which can decrease vasopermeability, increase the closely combination of cells, reduce local oxidative stress (OS) reaction and local inflammation reaction of cerebral tissues by depressing monocyte chemoattractant protein-1, which can further protect nervous system, alleviate the dysfunction and injury of nerves caused by local damage of cerebral tissue. However, the effect of edaravone alone is limited[9].The combination of traditional Chinese medicine and Western medicine has been gradually recognized in clinical practice over the past years. Several clinical researches[14,15]based on the combination of traditional Chinese medicine and Western medicine in treating hemorrhagic infarction has been done and received positive efficacy.
Medicines like Maixuekang Capsules are widely used in traditional Chinese medicine in treating hemorrhagic infarction, and Maixuekang Capsules is one of the representative medicines of traditional Chinese medicine in promoting blood circulation for removing blood stasis, whose essential component is hirudin.As Shennong's Herbal puts, Hirudo is mainly used to expel pathogenic blood stasis. It can remove blood stasis and disintegrate masses with drastic medicaments,and promote urination as well. That means Hirudo has a function of removing blood stasis with drastic medicaments, and promoting blood circulation without damaging new blood[11]. Modern pharmacology has confirmed that the partially hydrolyzed fragment of hirudin can restrain the function of thrombin, prolong the time of serum thrombin, prothrombin, and thrombin of activation part through direct impact on thrombin; it can also decrease the level of plasma fibrillarin and prevent thrombosis. Clinical practices have shown that the effectiveness of hirudin alone was obviously better than simple western medicine in treating infarction, but it's still not very effective[13].
This study used Maixuekang Capsules on the basis of edaravone in treatment, and found that the total effective rate of treatment group (92.11%) was significantly higher than that in control group (71.05%), which indicated that the combination of these two medicines could actually improve the effectiveness of the treatment. Besides,other study[16]has found that Maixuekang Capsules can relieve inflammation reaction around hematoma area by promoting the absorption of surrounding hematoma, and then facilitating the recovery of cerebral nerves' function and decreasing invalidism rate. To further confirm above study result, this study observed patients' improvement of neurological functions and their recovery conditions after the treatment, and found that the declining degree of NIHSS score and increasing degree of ADL score in treatment group were all higher than thohse of control group, which confirmed that the combination of these two medicines could further promote the recovery of patients'neurological function, improve their living ability after the surgery and prevent patients from disability after the treatment.
The concentrations of MMP-9 and S-100β in blood is low in normal condition. However, if the nerves were damaged, MMP-9 and S-100β could seep from damaged neuron, get into blood through blood-brain barrier, and result in the abnormal increase of the concentrations of MMP-9 and S-100β in serum. MMP-9 is a crucial protein of transudate from blood-brain barrier, which is the core reason of plaque instability[17], and the specific biochemistry marker of acute cerebral infarction at the early stage. Liu Jingsong and his team had studied the relationship between MMP-9 and the prognosis of infarction[18], and found that the incidence of complication after hemorrhagic infarction could be significantly decreased by inhibiting the expression of MMP-9 protein, which had positive effect on the prognosis of the patients. S-100β is a kind of acidic micromolecule calbindin protein secreted by cerebral astrocyte and glial cells, which can not only reflect the damage degree of nerve cells, but also decide the prognosis of hemorrhagic infarction[19]. The result of this study showed that the level of MMP-9 and S-100β in treatment group is significantly lower than that in control group; the decreasing degree of NIHSS score and increasing degree of ADL score in treatment group were both vitally higher than control group.
The result further indicated that the combination could obviously decrease the level of MMP-9 and S-100β,reduce the damage of cerebral organization and relatively accelerate the recovery of neurological function. It might because MMP-9 can enhance the permeability of vessels in basal lamina by degrading its crucial component,which will further damage blood-brain barrier, rupture the plaque, and contribute to cerebral thrombosis; and then will cause the disorder of cerebral flow, secondary cerebral hemorrhage and cerebral edema. Moreover, S-100β,as neurotrophic factor, can promote the recovery and regeneration of nervous tissues, but it can also stimulate microglia secrete large amount of inflammation factors and NO, etc., which can injure nerve cells.
In addition, this study also found that the level of S-100β was significantly increased on the 3rdday after the treatment while vitally decreased after that. It might because of the continuing rupture of the cerebral microvessels, incomplete effect of drugs and the delayed recovery of blood-brain barrier. The level of S-100β of patients with acute infarction had already been detected by Tang Fei's team in 2014[20]; they found that the level of S-100β in their study also reached the peak at the 3rdday after the attack, and patients with cerebral hemorrhage would have an extending peak, which was almost the same as the results in our study. The results indicated that closely attention should be paid on patients at the 3rdday after the treatment and thrombolysis, pressure release and other symptomatic treatment should always be ready in case of the enlargement of infarction area and deteriorating extent of cerebral edema.
Above all, Maixuetong Capsules combined with edaravone can significantly decrease the level of serum MMP-9 and S-100β protein of patients with hemorrhagic infarction, improve both the function of nerve cells and daily living abilities of the patients with lower incidence of adverse reactions and guaranteed security.
猜你喜欢
杂志排行

World Journal of Integrated Traditional and Western Medicine的其它文章
- World Integrated Medicine Master Wu Yiling
- Evaluation of Efficacy and Safety of Electro-acupuncture Precondition on Postoperative Cognitive Dysfunction (POCD)Following Knee Replacement in Elderly:A Randomized Controlled Trial
- New Year's Message
- Effects of Acupoint Massage Combined with Psychological Nursing on Depression and Hope Level and Coping Style in Hospitalized Patients with Hepatocirrhosis
- The Method of Soothing the Liver in the Treatment of Acute Abdominal Pain
- Effects of Yigan Tiaozhi Decoction on Serum NO, Endotoxin and RBP4 in Patients with Nonalcoholic Fatty Liver Disease