可溶性生长刺激表达基因2蛋白、氨基末端脑钠肽前体及同型半胱氨酸水平在急性冠脉综合征中的表达及临床意义
2019-01-08张巧玲邹文毕刘家超
张巧玲 邹文毕 刘家超

[摘要]目的 探讨可溶性生长刺激表达基因2蛋白(sST2)、氨基末端脑钠肽前体(NT-proBNP)及同型半胱氨酸(Hcy)水平在急性冠脉综合征(ACS)中的表达及临床意义。方法 选取2017年1月~2018年6月我院收治的87例ACS患者作为研究对象,根据临床表现、心电图、心肌损伤标志物的不同分为ST段抬高型心肌梗死(STEMI)组(31例)、非ST段抬高型心肌梗死(NSTEMI)组(30例)、不稳定型心绞痛(UA)组(26例);选取同期住院的非ACS患者100例作为对照组。检测并比较四组的sST2、NT-proBNP及Hcy水平,通过受试者工作特征(ROC)曲线评估sST2、Hcy及NT-proBNP诊断ACS的价值。结果 STEMI组和NSTEMI组的sST2水平高于对照组和UA组,差异均有统计学意义(P<0.05),病情越严重,sST2水平越高;STEMI组、NSTEMI组和UA组的NT-proBNP水平高于对照组,差异均有统计学意义(P<0.05);STEMI組和NSTEMI组的Hcy水平高于对照组,差异均有统计学意义(P<0.05)。sST2的ROC曲线下面积(AUC)为0.755(95%CI:0.685~0.824,P<0.001),最佳临界点为36.250,灵敏度为65.5%,特异度为73.0%;NT-proBNP的AUC为0.725(95%CI:0.653~0.797,P<0.001),最佳临界点为601.865,灵敏度为81.6%,特异度为57.0%;Hcy的AUC为0.652(95%CI:0.574~0.730,P<0.001),最佳临界点为10.250,灵敏度为66.7%,特异度为58.0%。三者联合检测的AUC为0.789,灵敏度为58.6%,特异度为89.0%。结论 血清sST2、NT-proBNP、Hcy及联合检测可作为诊断ACS的辅助指标,且sST2与疾病严重程度相关。
[关键词]急性冠脉综合征;可溶性生长刺激表达基因2蛋白;氨基末端脑钠肽前体;同型半胱氨酸
[中图分类号] R541.4 [文献标识码] A [文章编号] 1674-4721(2019)11(c)-0004-04
Expression and clinical significance of soluble growth stimulating gene 2 protein, amino-terminal pro-brain natriuretic peptide and homocysteine in acute coronary syndrome
ZHANG Qiao-ling1 ZOU Wen-bi1 LIU Jia-chao2
1. Department of Clinical Laboratory, Sanshui District People′s Hospital of Foshan City, Guangdong Province, Foshan 528100, China; 2. Department of Internal Medicine-Cardiovascular, Sanshui District People′s Hospital of Foshan City, Guangdong Province, Foshan 528100, China
[Abstract] Objective To investigate the expression and clinical significance of soluble growth stimulating gene 2 protein (sST2), amino terminal pro-brain natriuretic peptide (NT pro-BNP) and homocysteine (Hcy) in acute coronary syndrome (ACS). Methods A total of 87 patients with ACS admitted to our hospital from January 2017 to June 2018 were selected as the research objects, they were divided into three groups: ST segment elevation myocardial infarction (STEMI) group (31 cases), non ST segment elevation myocardial infarction (NSTEMI) group (30 cases) and unstable angina (UA) group (26 cases), according to the different clinical manifestations, ECG and myocardial injury markers. 100 cases of non ACS patients at the same period were taken as the control group. The levels of sST2, NT proBNP and Hcy were measured and compared among the four groups. The diagnostic value of sST2, Hcy and NT pro-BNP in ACS was evaluated by ROC curve. Results The levels of sST2 in STEMI group and NSTEMI group were higher than those in control group and UA group, the differences were statistically significant (P<0.05), the more serious the disease, the higher the level of sST2. The level of NT pro-BNP in STEMI group, NSTEMI group and UA group were higher than those in the control group, the differences were statistically significant (P<0.05). The Hcy level of STEMI group and NSTEMI group were higher than those of the control group, the differences were statistically significant (P<0.05). The area under ROC curve (AUC) of sST2 was 0.755 (95%CI was 0.685-0.824, P<0.001), the best critical point was 36.250, the sensitivity was 65.5%, and the specificity was 73.0%. The area under ROC curve (AUC) of NT-proBNP was 0.725 (95%CI was 0.653-0.797, P<0.001), the best critical point was 601.865, the sensitivity was 81.6%, the specificity was 57.0%. The AUC of Hcy was 0.652 (95%CI was 0.574-0.730, P<0.001), the best critical point was 10.250, the sensitivity was 66.7%, and the specificity was 58.0%. Combined detection of the three, the AUC was 0.789, the sensitivity was 58.6%, and the specificity was 89.0%. Conclusion Serum sST2, NT pro-BNP, Hcy and combined detection can be used as auxiliary indexes to diagnose ACS, and ST2 is related to disease severity.
[Key words] Acute coronary syndrome; Soluble growth stimulating gene 2 protein; Amino-terminal pro-brain natriuretic peptide; Homocysteine
急性冠脉综合征(acute coronary syndrome,ACS)是冠心病中的一种危重情况,ACS患者病情变化快,临床表现多样,对ACS患者进行及时合理的风险评估,有助于判断预后,选择合理的治疗策略。研究[1]显示,动脉粥样硬化是一种慢性炎症性疾病,炎症细胞刺激炎症因子表达,诱导组织因子及一氧化氮的产生,使血小板聚集、激活凝血系统,使不稳定斑块发生破裂、形成血栓,造成血管阻塞,最后导致ACS的发生[2]。可溶性生长刺激表达基因2蛋白(soluble growth-stimulated gene 2,sST2)作为一种新型的标志物,在全身多种器官炎症性疾病中都有升高[3],由于能同时反映心肌纤维化和心肌重构等情况,对多种心血管疾病不良预后事件具有较强的预测价值[4-5],已被纳入2017 ACC/AHA心力衰竭的管理更新版指南中[6],有望成为新的治疗靶点。本研究即通过检测ACS患者血清中sST2、氨基末端脑钠肽前体(amino-terminal pro-brain natriuretic peptide,NT-proBNP)及同型半胱氨酸(homocysteine,Hcy)水平,探讨sST2、NT-proBNP及Hcy水平在ACS中的表达及临床意义,现报道如下。
1资料与方法
1.1一般资料
选取2017年1月~2018年6月我院收治的87例ACS患者作为研究对象,根据临床表现、心电图、心肌损伤标志物的不同分为ST段抬高型心肌梗死(ST segment elevation myocardial infarction,STEMI)组(31例)、非ST段抬高型心肌梗死(non-ST segment elevated myocardial infarction,NSTEMI)组(30例)、不稳定型心绞痛(unstable angina,UA)组(26例);选取同期住院的非ACS患者100例作为对照组。STEMI组中,男24例,女7例;年龄47~85岁,平均(64.2±12.2)岁。NSTEMI组中,男21例,女9例;年龄47~90岁,平均(66.3±13.1)岁。UA组中,男19例,女7例;年龄47~84岁,平均(66.9±12.8)岁。对照组中,男73例,女27例;年龄42~81岁,平均(58.9±9.3)岁。四组的一般资料比较,差异无统计学意义(P>0.05),具有可比性。本研究已经医院医学伦理委员会审核批准。
实验组纳入标准:①所有患者参考中华医学会《急性ST段抬高型心肌梗死诊断和治疗指南(2015)》[7]和中华医学会《非ST段抬高型急性冠脉综合征诊断和治疗指南(2012)》的诊断标准[8];②所有患者及其家属均知情同意。实验组排除标准:①冠脉血运重建、慢性心功能不全、心肌病、心脏瓣膜病的患者;②哮喘、慢性阻塞性肺疾病的患者;③急慢性感染、肿瘤的患者;④严重肝、肾功能不全的患者。对照组纳入标准:①心绞痛症状不典型者;②心电图未见明显异常者;③冠脉造影结果未见明显异常者。对照组排除标准同实验组。
1.2方法
患者入院第2天清晨,采集空腹桡静脉血5 ml置于分離胶管,4 h内采用离心机2000 r/min离心20 min,取其血清,分装于1 ml EP管中,在-50℃冰箱中保存,留待检测sST2水平。剩余血清在2 h内检测NT-proBNP水平,24 h内检测Hcy水平。
1.3观察指标及评价标准
比较四组的sST2、NT-proBNP及Hcy水平,通过受试者工作特征(ROC)曲线评估sST2、Hcy及NT-proBNP诊断ACS的价值。①采用sST2酶联免疫分析试剂盒(德国QIAGEN公司,批号:201801)检测sST2水平。实验按照试剂盒说明书方法操作。最终测得450 nm波长的吸光度(OD值),按照标准物浓度及OD值绘制坐标图,计算出sST2浓度的直线回归方程式,将样本的OD值代入方程式计算出sST2的浓度,乘以稀释倍数,即为样品的实际浓度。②采用Cobas E602型电化学发光仪(美国罗氏公司)及原装配套试剂(美国罗氏公司,批号:209223、227748、292808)检测NT-proBNP水平。③采用ARCHITECT 12000SR型化学发光仪(美国雅培公司)及原装配套试剂(美国雅培公司,批号:10650UP00、10656UP00、10676UP00)检测Hcy水平。
1.4统计学方法
采用统计学软件SPSS 25.0分析数据,符合正态分布的计量资料以均数±标准差(x±s)表示,采用t检验;不符合正态分布的计量资料以中位数(四分位数)表示,采用非参数检验中的Kruskal-Wallis H检验;采用受试者工作特征(ROC)曲线评估各指标的诊断价值,预测ΔCI≥15%的效能,并确定各参数最佳临界值,以P<0.05为差异有统计学意义。
2结果
2.1 四组研究对象血清中sST2、NT-proBNP及Hcy水平的比较
STEMI组和NSTEMI组的sST2水平高于对照组和UA组,差异均有统计学意义(P<0.05),病情越严重,sST2水平越高;对照组和UA组的sST2水平比较,差异无统计学意义(P>0.05);STEMI组和NSTEMI组的sST2水平比较,差异无统计学意义(P>0.05)。STEMI组、NSTEMI组和UA组的NT-proBNP水平高于对照组,差异均有统计学意义(P<0.05);STEMI组、NSTEMI组和UA组的NT-proBNP水平比较,差异无统计学意义(P>0.05)。STEMI组和NSTEMI组的Hcy水平高于对照组,差异均有统计学意义(P<0.05);对照组和UA组的Hcy水平比较,差异无统计学意义(P>0.05);STEMI组、NSTEMI组和UA组的Hcy水平比较,差异无统计学意义(P>0.05)(表1)。
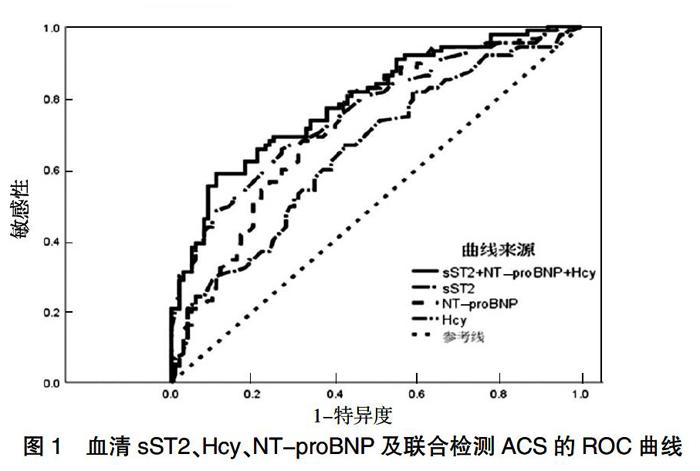
2.2 ROC曲线评估sST2、Hcy、NT-proBNP及联合检测的诊断价值
sST2的ROC曲线下面积(AUC)为0.755(95%CI:0.685~0.824,P<0.001),最佳临界点为36.250,灵敏度为65.5%,特异度为73.0%;NT-proBNP的AUC为0.725(95%CI:0.653~0.797,P<0.001),最佳临界点为601.865,灵敏度为81.6%,特异度为57.0%;Hcy的AUC为0.652(95%CI:0.574~0.730,P<0.001),最佳临界点为10.250,灵敏度为66.7%,特异度为58.0%。三者联合检测的AUC为0.789,灵敏度为58.6%,特异度为89.0%(图1)。
3讨论
sST2是白细胞介素-33(IL-33)的可溶性受体[9],当心肌细胞受到生物机械性拉伸时sST2和跨膜型ST2(ST2L)表达明显增高,尤其是sST2表达更为明显,大量sST2与IL-33结合,从而阻断IL-33与ST2L结合,继而削弱IL-33/ST2L信号通路的心血管保护作用[10]。急性心肌梗死(AMI)缺血缺氧促进IL-33和sST2的表达及细胞凋亡[11]。AMI患者血清sST2水平明显升高,提示sST2水平可以反映心脏功能[12]。Andersson等[13]的研究显示,sST2水平升髙可能与潜在的心血管风险增加有关。本研究结果显示,STEMI组和NSTEMI组的sST2水平高于对照组和UA组,差异均有统计学意义(P<0.05);对照组和UA组的sST2水平比较,差异无统计学意义(P>0.05);STEMI组和NSTEMI组的sST2水平比较,差异无统计学意义(P>0.05)。
缺血缺氧可能刺激NT-proBNP的分泌,且与缺血的严重程度密切相关[14]。ACS患者冠脉病变远端血管为完全性或非完全性闭塞,心肌常为缺血状态,无论是不稳定性心绞痛(UAP)患者或AMI患者,在心肌细胞急性缺氧或者是坏死的情况下,均可使NT-proBNP表达增加。sST2、NT-proBNP水平在急性心力衰竭患者及慢性心力衰竭急性失代償患者血清中均有升高,其水平与心衰严重程度成正相关[15-16];有研究[17]显示,ACS患者心室肌细胞所分泌释放的NT-pro BNP与冠状动脉病变血管支数及心肌缺血程度成正相关。本研究结果显示,STEMI组、NSTEMI组和UA组的NT-proBNP水平高于对照组,差异均有统计学意义(P<0.05);STEMI组和NSTEMI组的Hcy水平高于对照组,差异均有统计学意义(P<0.05);对照组和UA组的Hcy水平比较,差异无统计学意义(P>0.05);STEMI组、NSTEMI组和UA组的Hcy水平比较,差异无统计学意义(P>0.05)。国内外研究显示[18-19],血清Hcy随着冠心病病情的严重程度而升高,且冠状动脉病变支数随Hcy水平上升呈增加的趋势,提示Hcy在冠心病的发展进程中扮演着重要的角色,临床上可将其作为冠心病的预警因子,并用来评价冠状动脉病变的程度。
Marino等[20]的研究结果显示,sST2对出院后30 d心脏病死亡率具有更高的预后价值,在STEMI患者中,sST2值>35 ng/ml对短期死亡率有最高预测能力。血清ST2,IL-33和NT-proBNP水平是主要冠脉不良事件的独立危险因素,其水平较低的AMI患者的1年总生存率较高[21]。本研究结果显示,sST2诊断ACS效果最好,NT-proBNP灵敏度最好,三者联合诊断的特异度最高,与宗斌[22]的研究结果相符。
本研究的基线资料显示,有高血压/高血脂的患者比正常人患ACS的风险分别高1.526、2.284倍,限于本研究的样本量,笔者将对有无高血压或高血脂的人群展开进一步的分析放在下一阶段的研究中。同时,指标对于ACS危险分层和预后的预测价值如何,也是笔者接下来研究的方向。
综上所述,血清sST2、NT-proBNP、Hcy及联合检测可作为诊断ACS的辅助指标,且sST2与疾病严重程度相关。
[参考文献]
[1]Libby P.Inflammationin atherosclerosis[J].Arterioscler Thromb Vasc Biol,2012,32(9):2045-2051.
[2]Ross R.Atherosclerosis——an inflammatory disease[J].N Engl J Med,1999,340(2):115-126.
[3]Sun Z,Chang B,Huang A,et al.Plasma levels of soluble ST2,but not IL-33,correlate with the severity of alcoholic liver disease[J].J Cell Mol Med,2019,23(2):887-897.
[4]Liu X,Hu Y,Huang W,et al.Soluble ST2 for prediction of clinical outcomes in patients with ST-segment elevation myocardial infarction receiving primary PCI[J].Int Heart J,2019,60(1):19-26.
[5]Billiar IM,Guardado J,Abdul-Malak O,et al.Elevations in circulating sST2 levels are associated with in-hospital mortality and adverse clinical outcomes after blunt trauma[J].J Surg Res,2019,244:23-33.
[6]Yancy CW,Jessup M,Bozkurt B,et al.2017 ACC/AHA/HFSA focused update of the 2013 ACCF/AHA guideline for the management of heart failure:a report of the american college of Cardiology/American heart association task force on clinical practice guidelines and the heart failure society of america[J].J Card Fail,2017,23(8):628-651.
[7]中華医学会心血管病学分会,中华心血管病杂志编辑委员会.急性ST段抬高型心肌梗死诊断和治疗指南[J].中华心血管病杂志,2015,43(50):380-393.
[8]中华医学会心血管病学分会,中华心血管病杂志编辑委员会.非ST段抬高急性冠状动脉综合征诊断和治疗指南[J].中华心血管病杂志,2012,40(5):353-367.
[9]Schmitz J,Owyang A,Oldham E,et al.IL-33,an interleukin-1-like cytokine that signals via the IL-1 receptor-related protein ST2 and induces T helper type 2-associated cytokines Schmitz[J].Immunity,2005,23(5):479-490.
[10]Mueller T,Jaffe AS.Soluble ST2-analytical considerations[J].Am J Cardiol,2015,115(7S):8B-21B.
[11]Yang J,Hu F,Fu X,et al.Mir-128/Sox7 alleviates myocardial ischemia injury by regulating IL-33/sST2 in acute myocardial infarction[J].Biol Chem,2019,400(4):533-544.
[12]张剑,王明磊.急性心肌梗死患者血清HS、sST2的变化及预测价值[J].中国循证心血管医学杂志,2018,10(12):1568-1570.
[13]Andersson C,Enserro D,Sullivan L,et al.Relations of circulating GDF-15,soluble ST2,and troponin-Ⅰconcentrations with vascular function in the community:the framingham heart study[J].Atherosclerosis,2016,248:245-251.
[14]de Lemos JA,Morrow DA.Brain natriuretic peptide measurement in acute coronary syndromes:ready for clinical application?[J].Circulation,2002,106(23):2868-2870.
[15]高明,李琳,崔维.急性心力衰竭患者sST2、NT-proBNP的水平变化及临床意义[J].中国循证心血管医学杂志,2019,11(1):41-43,47.
[16]尹坤,张武,向睿.血清可溶性ST2在慢性心力衰竭急性失代偿早期诊断和近期预后评估中的作用[J].临床内科杂志,2019,36(4):250-253.
[17]Struthers AD,Davies J.B-type natriuretic peptide:a simple new test to identify coronary artery disease[J].QJM,2005, 98(10):765-769.
[18]马锦洪,史伟峰,于宗良,等.血清同型半胱氨酸和血脂代谢水平与冠状动脉病变的相关性分析[J].中国卫生检验杂志,2016,26(5):706-708,711.
[19]Cioni G,Marcucci R,Gori AM,et al.Increased homocysteine and lipoprotein(a) levels highlight systemic atherosclerotic burden in patients with a history of acute coronary syndromes[J].J Vasc Surg,2016,64(1):163-170.
[20]Marino R,Magrini L,Orsini F,et al.Comparison between soluble ST2 and high-sensitivity troponin i in predicting short-term mortality for patients presenting to the emergency department with chest pain[J].Ann Lab Med,2017,37(2):137-146.
[21]Wang YP,Wang JH,Wang XL,et al.Roles of ST2,IL-33 and BNP in predicting major adverse cardiovascular events in acute myocardial infarction after percutaneous coronary intervention[J].J Cell Mol Med,2017,21(11):2677-2684.
[22]宗斌.外周血内sST2水平评价急性心力衰竭患者病情严重程度及预后质量的临床价值分析[J].中国医药导报,2017,14(26):60-63.
(收稿日期:2019-04-09 本文编辑:刘克明)
