Tuina for primary insomnia: a meta-analysis
2018-09-12CaoMiao曹淼DengFangfang邓芳芳YuanQun袁群ZhangJidong张冀东HeQinghu何清湖
Cao Miao (曹淼), Deng Fang-fang (邓芳芳), Yuan Qun (袁群), Zhang Ji-dong (张冀东), He Qing-hu (何清湖)
Abstract Objective: To systematically evaluate the therapeutic efficacy of tuina therapy for primary insomnia.Methods: Nine Chinese and English databases were searched from the inception to May 2017 to identify randomized controlled trials (RCTs) studying tuina therapy for insomnia. The enrolled articles were all RCTs with tuina as the monotherapy or major therapy in the experiment group, with clear diagnostic criteria for primary insomnia well recognized worldwide or in China, and Pittsburgh sleep quality index (PSQI) as one of the outcome measures. Two researchers evaluated the risk of bias and quality of the enrolled studies by following Cochrane Handbook version 5.1.0. The meta-analysis was performed by RevMan version 5.3.Results: Eleven studies were included with a total of 1 076 participants. The Western medication adopted in the control groups were benzodiazepine receptor agonists. The studies were all assessed as high risk of bias for blinding since blinding method was unable to be performed due to the specificity of tuina therapy; no study reported the support of fund or potential interest conflict, so they were all rated unclear for selective reporting. The meta-analysis showed that compared with other traditional Chinese medicine therapies, tuina worked more effectively in reducing the PSQI score (MD=–4.11<0,95% confidence interval (CI) –6.01 to –2.22, P<0.0001); compared with oral administration of Western medication, tuina showed more significant efficacy in reducing the PSQI score (MD=–3.42<0, 95%CI –5.19 to –1.66, P<0.0001). Subgroup analysis showed that head tuina alone showed no significant difference compared with oral administration of Western medication regarding the change of PSQI score (MD=–4.19<0, 95%CI –8.87 to 0.50, P>0.05); a combination of head and back tuina could more effectively reduce the PSQI score compared with oral administration of Western medication (MD=–2.08<0,95%CI –3.09 to –1.06, P<0.0001).Conclusion: Tuina can produce more significant efficacy in treating primary insomnia compared with other traditional Chinese medicine therapies and oral administration of Western medication, especially the combination of head and back tuina.
Keywords: Tuina; Massage; Insomnia; Acupoint, Head; Pittsburgh Sleep Quality Index; Randomized Controlled Trial;Systematic Review; Meta-analysis
Insomnia is a very common disease mainly characterized by difficulty initiating or maintaining sleep or frequent waking up[1-3]. It not only affects the daily function and quality of life[4], but also closely relates to chronic mental disorders[5-7]. There are many treatments available to treat insomnia, different methods for different groups of people, while benzodiazepine receptor agonists are most commonly used. However, there is a high risk of relapse after termination of this type of drug, not to mention that it may cause many side effects[8-9]. Besides oral medications, non-drug therapies are also used to treat insomnia and generally considered safer and suitable for more people despite its slow action and indefinite efficacy[10]. Different insomnia patients may have completely different requirements for treatment, and doctors should try different ways to treat it. Tuina is a traditional Chinese medicine (TCM) therapy. It is estimated that one of every four insomnia patients has used this therapy[11-12]. Tuina has a very long history not only in China but also in countries like India where similar therapies have existed for a long time[13]. Tuina has many advantages in treating insomnia, including high safety, sufficient number of tuina practitioners and high accessibility[14-15]. Modern medical studies have verified the effect of tuina therapy in improving cardiovascular function, endocrine system, blood circulation, tension and pain[16-19]. The main action mechanism of tuina therapy is to produce neural stimulation and send it to autonomic nervous system and central nervous system to promote the release of neurotransmitters through touching, pressing and thermal effect[20]. Recent studies have proved that tuina can mitigate insomnia in peri-menopausal women and the elderly[21-22]. Despite many literatures that provide evidence for the efficacy of tuina for insomnia, the overall efficacy has not been systematically evaluated.Therefore, we conducted this research to systematically review the therapeutic efficacy of tuina for insomnia.
1 Materials and Methods
1.1 Retrieve of study
Nine Chinese and English databases were searched from the inception to May 2017.
The English databases included: PubMed, Embase,Cumulative Index to Nursing and Allied Health Literature (CINAHL), the Cochrane Central Register of Controlled Trials (CENTRAL) and the Allied and Complementary Medicine (AMED).
The Chinese databases included: Chinese Biomedical Literature Database (CBM), China National Knowledge Infrastructure (CNKI), Chongqing VIP Database (CQVIP)and Wanfang Academic Journal Full-text Database(Wanfang).
Only randomized controlled trials (RCTs) were identified.
#1 Key words of disease name: including ‘Shi Mian’,‘Bu Mei’, ‘Shao Mian’ and ‘Shui Mian Zhang Ai’ for Chinese databases; ‘insomnia’, ‘sleeplessness’ and‘sleep disorders’ for English databases.
#2 Key words of interventions: including ‘Tui Na’, ‘An Mo’ and ‘Shou Fa’ for Chinese databases; ‘tuina’,‘manipulation’ and ‘massage’ for English databases.
Search strategy: #1 AND #2. To avoid missed retrieval,‘randomized controlled trial’ was not used as the research term but confirmed later by review of abstract and full text.
1.2 Inclusion criteria
1.2.1 Diagnostic criteria
Insomnia was the major complaint of the participants and the case conformed to the following diagnostic criteria: Diagnostic and Statistical Manual of Mental Disorders (DSM)[4,23], International Classification of Sleep Disorders (ICSD)[24], International Classification of Diseases (ICD)[25], Chinese Classification and Diagnosis of Mental Diseases (CCMD, including CCMD-3 and CCMD-4)[26-27]; insomnia accompanied by other diseases and secondary insomnia were excluded.
1.2.2 Interventions and controls
Tuina, acupuncture-moxibustion and oral administration of Chinese medication are major TCM interventions with totally different action mechanisms.Moreover, there are already systematic reviews of acupuncture-moxibustion and oral Chinese medication for primary insomnia. Hence, trials studying tuina plus acupuncture-moxibustion and tuina plus oral Chinese medication were excluded. Trials studying tuina as the major treatment plus other assistant TCM methods such as foot bath and auricular point sticking were included. The controls could be conventional modern medicine therapies, e.g. benzodiazepine receptor agonists, or other TCM methods for insomnia including acupuncture-moxibustion and Chinese medication, but controls containing tuina therapy were excluded.
1.2.3 Study design
Only RCTs were enrolled while the detailed method was not limited; regardless of blinding or concealing;written in Chinese or English.
1.2.4 Outcome measure
Pittsburgh sleep quality index (PSQI) was used as the main outcome measure since it is one of the most popular and well-recognized insomnia measures[28-29].
1.3 Data extraction and study quality assessment
Two authors independently extracted data (Cao Miao and Deng Fang-fang were in charge of English articles;Cao Miao and Yuan Qun were in charge of Chinese articles). The extracted data included: where the trial was conducted, diagnostic criteria, disease duration,sample size, age, gender, interventions and controls,treatment duration, follow-up, outcome measures and adverse reactions. The methodological quality was assessed using Cochrane Collaboration’s risk of bias tool(Cochrane Handbook 5.1.0) from nine aspects: random sequence generation; allocation concealment; blinding method; incomplete outcome data; selective reporting;other bias (baseline, fund support or potential conflict of interest).
1.4 Statistical analysis
The data were analyzed using RevMan version 5.3.We examined heterogeneity among the stu2dies. A fixed effects model was used when P>0.01 and I<50% which in2dicated insignificant heterogeneity; when P≤0.01 and I≥50% which indicated significant heterogeneity, and the heterogeneity was unexplainable by clinical or methodological heterogeneity, a random effects model would be used. Enumeration data were analyzed as dichotomous data and expressed as relative risk (RR)and 95% confidence interval (CI); measurement data were examined as continuous data and expressed as mean difference (MD) and 95%CI. Subgroup analysis was conducted according to the different body parts that received tuina treatment. A funnel plot was carried out to analyze the publication bias.
2 Results
2.1 Literature search and screening result
According to the search strategy, 1 613 articles were identified at the initial search; 162 full-text articles were remained after general screening; 151 articles were removed after review of detailed information including participants, intervention methods, control methods and outcome measures. As a result, 11 articles were included for meta-analysis[30-40]. The screening process is shown in Figure 1.
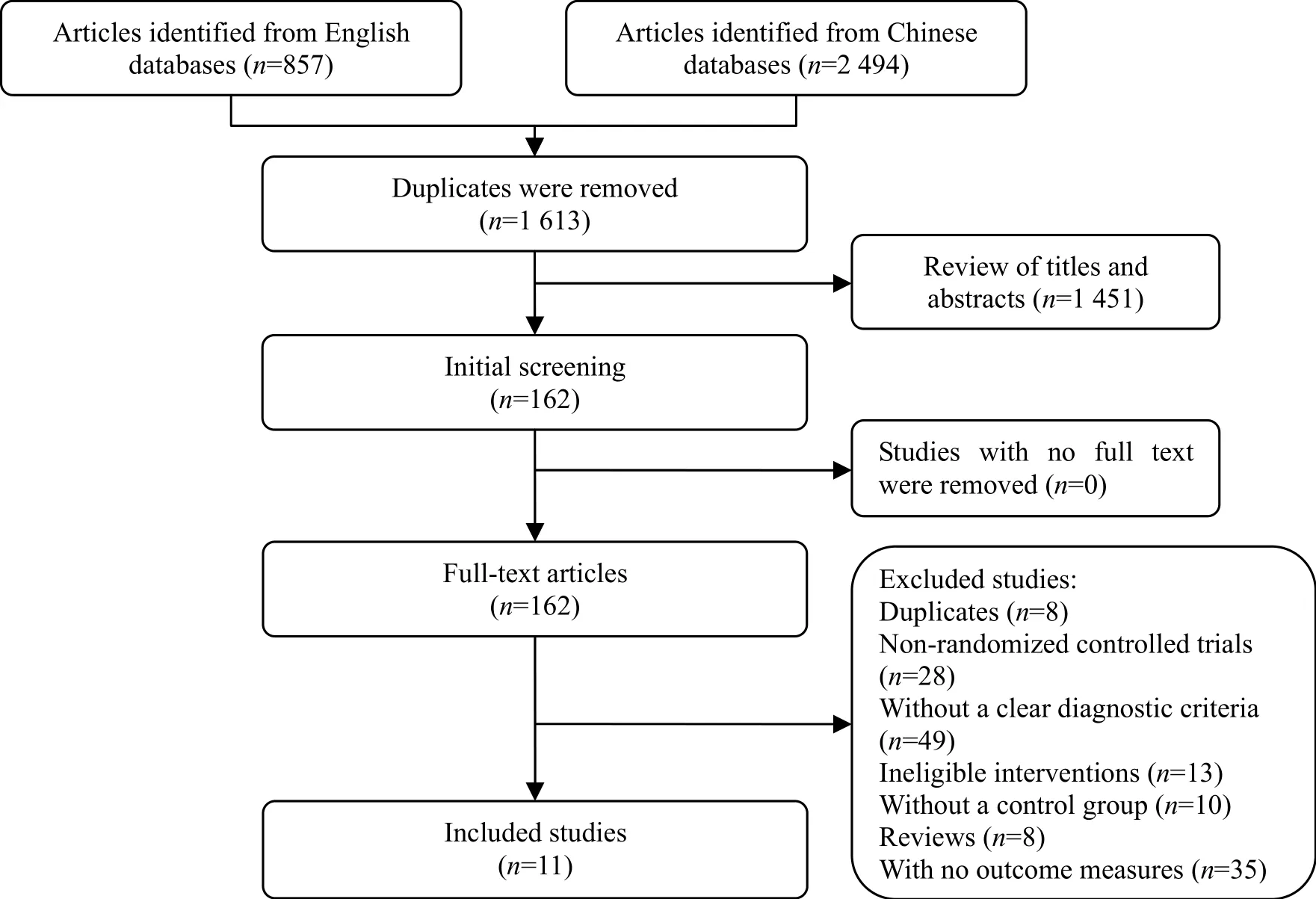
Figure 1. Literature screening process
Of the included studies, 7 adopted the diagnostic criteria of CCMD, 3 used the criteria of ICD and 1 conformed to the criteria of DSM. The 11 studies enrolled a total of 1 076 participants whose data of gender and age were unclear. Of the 11 studies, 4 studies used tuina plus other TCM therapies in the experiment group, including auricular point sticking[39],foot bath[34,38]and acupoint injection[36]; one study used a combination of tuina and Western medication as the experiment intervention[31]. The details are shown in Table 1.
2.2 Risk of bias analysis
Only five trials reported the method of random sequence generation, using a randomization table or computer-generated randomization number[31,37-40],while the rest did not report the method of randomization. None of the studies reported the allocation concealment. Because it is difficult to perform blinding in the study of tuina treatment, all studies were evaluated as ‘high risk’ in the performance of blinding. The studies were all rated ‘unclear’ in the selective reporting as the provided data were inadequate. All trials were evaluated as ‘low risk’ in the domain of other bias. No trial reported fund support or potential conflict of interest. Details of the risk of bias analysis are presented in Table 2.
The analysis did not reveal any significant publication bias in the 11 studies and the Egger’s test showed t=1.40, 95%CI [-3.89, 16.56], P=0.195 (Figure 2).
2.3 Tuina therapy versus other TCM therapies
Of the 11 included studies, 3 compared tuina therapy with other TCM therapies by evaluating the PSQI score.The heterogeneity analysis of the three trials showed P≤0.1 and I2≥50%, indicating significant heterogeneity.Therefore, a random effects model was used for synthesis and the result showed that tuina therapy was more effective than other TCM therapies in reducing the PSQI score (MD=–4.11<0, 95%CI –6.01 to –2.22,P<0.0001), (Figure 3).
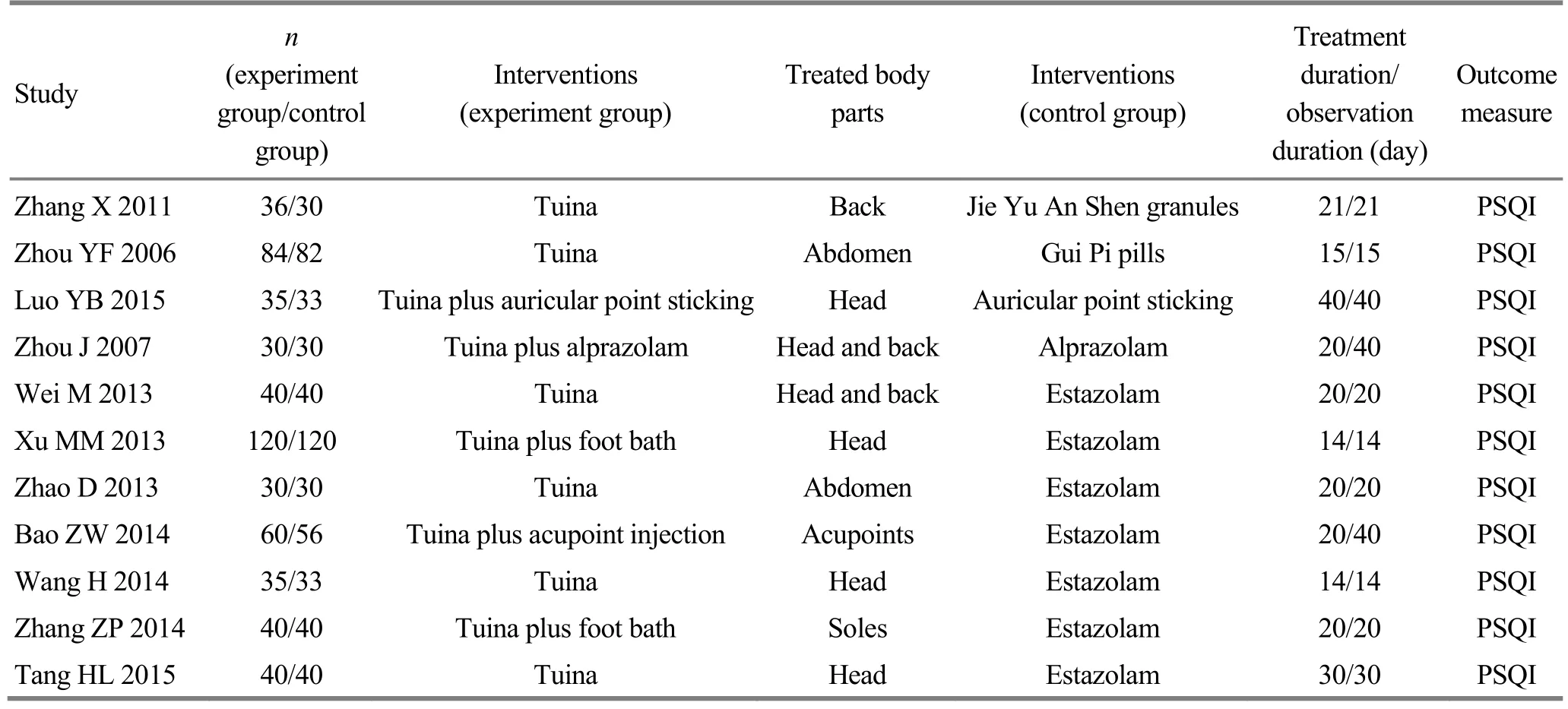
Table 1. Summary of the included studies
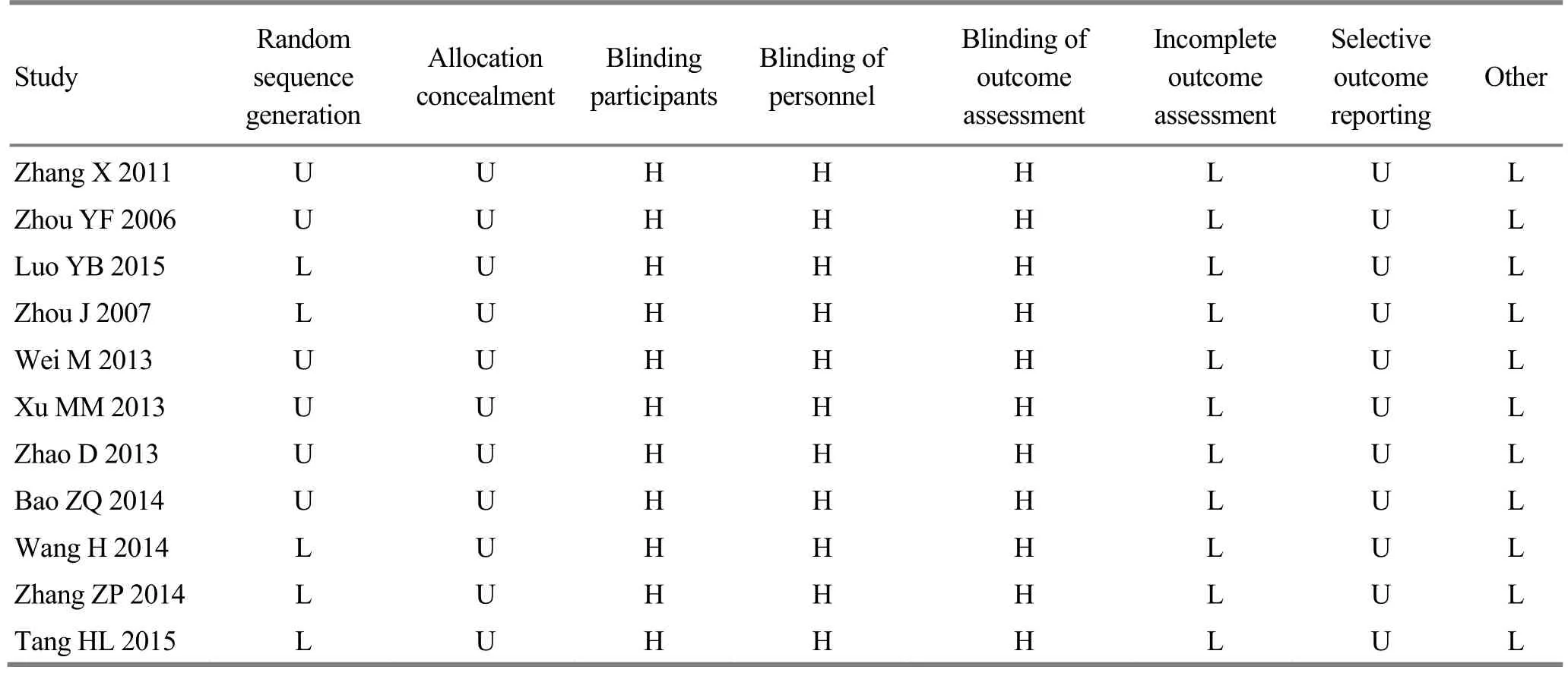
Table 2. Publication bias of the included studies
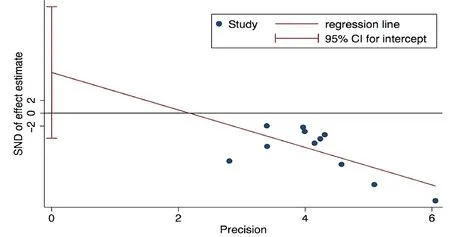
Figure 2. Funnel plot of the publication bias

Figure 3. Tuina therapy versus other TCM therapies for the PSQI score
2.4 Tuina therapy applied to different body parts versus oral Western medication
Of the 11 included studies, 2 adopted head and back tuina in the experiment group, 3 adopted head tuina,and 3 applied tuina to other body parts. They all took oral Western medication as the control and employed the PSQI score as the outcome measure. These 8 articles were also enrolled for a subgroup analysis based on the different treated regions. The heterogeneity analysis of the eight studies showed P≤0.1 and I2≥50%which indicated significant heterogeneity. Therefore, a random effects model was used for synthesis and the result showed a significant difference in favor of tuina therapy versus oral Western medication in reducing the PSQI score (MD=–3.42<0, 95%CI –5.19 to –1.66,P<0.0001). The subgroup analysis based on different tuina regions showed that there was no significant difference in the improvement of PSQI score between head tuina and oral Western medication (MD=–4.19<0,95%CI –8.87 to 0.50, P>0.05); the results identified a significant difference in favor of head and back tuina versus oral Western medication in the improvement of PSQI score (MD=–2.08<0, 95%CI –3.09 to –1.06,P<0.0001), (Figure 4).
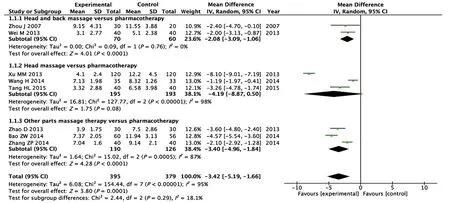
Figure 4. Tuina at different body parts versus oral Western medication for the PSQI score
2.5 Adverse reactions
None of the included studies reported adverse reactions.
3 Discussion
This research identified a significant difference in favor of tuina therapy versus oral administration of Western medication for the improvement of PSQI score and sleep quality. This conclusion conformed to recent study findings that tuina could ease the tension and anxiety in insomnia patients[22-23]. Treatment of insomnia with tuina involves a very complex physiological mechanism. Modern science majorly uses reflexology to explain the action mechanism, which holds that stimulation to different parts of skins and muscles can produce corresponding changes in activities of central nervous system. There was also evidence showing that tuina could stimulate the body to produce sleep-promoting factors such as 5-hydroxytryptamine (5-HT)[35]. A prospective study used polysomnography to observe women with insomnia and found that tuina shortened stage I of non-rapid eye movement (NREM) sleep and rapid eye movement (REM) sleep duration, and significantly extended state III and IV of NREM, which may be related to the function of tuina[41]. TCM believes that yin-yang imbalance should be the major factor causing insomnia.In a normal state, yang qi runs superficially in the daytime while internally in the nighttime. When yin and yang are imbalanced, yang qi will be unable to go internally but remain in the surface at night, manifested by excitement, difficulty initiating sleep or even insomnia. Via stimulating meridians and acupoints,tuina can regulate yin-yang and restore their balance[42-43]. Currently, tuina is mainly applied to head,back and soles, where most of the meridians associated with sleep distribute.
However, the following factors may influence the reliability of the conclusion in this research. Firstly, the included studies were different in the inclusion criteria,and were not quantified or unified in manipulations,treated body parts and treatment duration of tuina.Secondly, this study only searched Chinese and English databases, while there may be relevant studies written in other languages. Thirdly, the quality of the included trials was generally low and the risk of bias was high since double-blind method cannot be performed for tuina study. Fourthly, there were not enough studies comparing tuina with other forms of TCM therapies,making it unable to determine the advantage of tuina therapy.
4 Conclusion
To conclude, this meta-analysis identified a significant difference in favor of tuina versus oral administration of benzodiazepine receptor agonists for the improvement of PSQI score and sleep quality. Tuina should be recommended as one of the options to treat insomnia,and it should be applied to both head and back instead of head alone. Nevertheless, with regards to the low quality of the included studies, the conclusion in favor of tuina for insomnia needs to be supported by more rigorous RCTs with a large sample size.
Conflict of Interest
The authors declared that there was no potential conflict of interest in this article.
Acknowledgments
This work was supported by Hunan Provincial Innovation Foundation for Postgraduate (湖南省研究生科研创新项目, No. CX2017B427).
Received: 25 September 2017/Accepted: 29 October 2017
猜你喜欢
杂志排行

Journal of Acupuncture and Tuina Science的其它文章
- Therapeutic efficacy observation on acupuncture for persistent allergic rhinitis
- Effects of acupuncture on ovarian blood supply and pregnancy outcomes in patients receiving assisted reproduction
- Effect of Governor Vessel-unblocking and mindrefreshing acupuncture plus functional training on neural development in infants with brain damage
- Correlation analysis on clinical effects of acupuncture for elderly patients with sensorineural deafness and ear distending sensation
- Observation of therapeutic effects of point application at Shenque (CV 8) plus moxa-salt hot compress for prevention of gastrointestinal adverse reactions after chemotherapy for non-Hodgkin lymphoma
- Application and exploration of suspended magnetic moxibustion cup for obesity