Experimentally investigating the effect of buccal acupuncture on analgesic time-effect characteristics and monoamine neurotransmitters
2018-09-12PuRuisheng蒲瑞生FangXiaoli方晓丽JieWangjun颉旺军LiuDinglong刘丁龙SuChenghong苏成红
Pu Rui-sheng (蒲瑞生) , Fang Xiao-li (方晓丽) Jie Wang-jun (颉旺军) Liu Ding-long (刘丁龙) Su Cheng-hong (苏成红)
Abstract Objective: To investigate the analgesic time-effect characteristics and changes in concentrations of rabbit’s hypothalamic 5-hydroxytryptamine (5-HT) and noradrenaline (NE) caused by buccal acupuncture in the rheumatoid arthritis (RA) rabbits,and to reveal the analgesic central mechanism of buccal acupuncture, thereby providing a theoretical basis for the treatment of pain by buccal acupuncture.Methods: Forty rabbits were randomly divided into a normal group, a model group, a body acupuncture group, and a buccal acupuncture group, with 10 rabbits in each group. No model was established in the normal group, while equal dose of normal saline was injected at the matched site and time point; rabbits in other groups were subjected to the establishment of RA models using egg protein. From the 27th day of the experiment, rabbits in each group received the designated intervention. Rabbits in the normal group and the model group were fixed for 30 min every day using the same method as those in the other groups. In the acupuncture group, Dubi (ST 35) and Zusanli (ST 36) on bilateral hind limbs were selected. Perpendicular needling (using the needles with 0.25 mm in diameter and 25 mm in length) was performed with twirling manipulation for 15 s at intervals of 5 min. The needles were retained for 30 min and acupuncture was performed once a day. In the buccal acupuncture group, the knee point in the buccal acupuncture and needles with a diameter of 0.25 mm and a length of 15 mm were selected. Oblique needling was performed with twirling manipulation for 15 s at intervals of 5 min. The needles were retained for 30 min and acupuncture was performed once a day. The thermal pain thresholds at the 0, 5, 15, 30, 60, 120 and 240 min after the 1st and 10th acupuncture therapy were measured with a PL-200 thermal-inducing pain meter. After the 10th acupuncture therapy, rabbit’s hypothalamus was removed, and the 5-HT and NE concentrations in the hypothalamus at the peak point of the acupuncture pain threshold curve were determined by high performance liquid chromatography (HPLC).Results: The analgesic effect was obvious at 5 min after buccal acupuncture started, peaked at 30 min, and decreased to the lowest value at 240 min. Rabbits in the body acupuncture group began to show significant analgesic effect at 15 min, which was peaked at 30 min, and began to decline at 60 min. The pain threshold at 240 min was still higher than that at 0 min.Compared with the model group, the concentrations of hypothalamic 5-HT in the buccal acupuncture group and the body acupuncture group was significantly increased, and the between-group differences were statistically significant (both P<0.05). The NE/5-HT ratios in hypothalamus in the buccal acupuncture group and the body acupuncture group were significantly lower than the ratio in the model group, and the differences were statistically significant (both P<0.05);difference in the decrease was statistically significant between the buccal acupuncture group and the body acupuncture group (P<0.05).Conclusion: The analgesic effect of buccal acupuncture shows an obvious time-dependent curve. It is characterized by rapid onset of pain relief, rapid increase and decline in pain threshold. 5-HT and NE levels in rabbit’s hypothalamus can be affected by buccal acupuncture, with increased 5-HT concentration and reduced NE/5-HT ratio.
Keywords: Acupuncture Therapy; Buccal Acupuncture; Acupuncture Analgesia; Arthritis, Rheumatoid; 5-Hydroxytryptamine;Neuroregulators; Rabbits
Buccal acupuncture therapy is a method for treating diseases by puncturing specific acupoints in the buccal region. It has the advantages of simple acupoint selection, simple operation, rapid analgesic effect, lower recurrence, high safety and wide range of indications[1].Buccal acupuncture therapy has a good analgesic effect,but the characteristics of its analgesic effect, such as the time-effect and dose-effect, are still unclear. The experimental research on its analgesic mechanism is still at an exploratory stage.
In this study, by targeting the analgesic effect of buccal acupuncture, an egg protein-induced rheumatoid arthritis (RA) rabbit model was used to compare different stimulation methods. By comparing the pain threshold at different time points after the buccal acupuncture and the body acupuncture, the analgesic time-effect characteristics of the buccal acupuncture were clarified, and the differences in the time-effect characteristics of the analgesic effect between buccal acupuncture and body acupuncture were explored to provide a theoretical basis for the treatment of pain by buccal acupuncture. The central mechanism of the analgesic effect of buccal acupuncture was further revealed by observing the central monoamine neurotransmitter.
1 Materials and Methods
1.1 Experimental animals and grouping
In this experiment, 40 healthy white-ear rabbits aged 2 months were used, half male and half female,weighing 2.0-2.5 kg. The rabbits were adaptively fed for 1 week before the experiments, and screened with a thermal pain threshold assay. Rabbits with pain thresholds below 3 s (sensitive allodynia) and over 10 s(indicating dull allodynia) were excluded. The 40 rabbits all passed the pain threshold screening and then were randomly divided into a normal group, a model group, a body acupuncture group and a buccal acupuncture group (n=10) using the Microsoft Excel 2003 software.
1.2 Experimental drugs and reagents
Freund’s complete adjuvant (batch number:CAS9007-81-2) and egg albumin powder (batch number:SLBF-0342V) (Sigma, USA); methanol and acetonitrile(J.T. Baker Chemical Co., USA); formic acid (Buchs,Switzerland); DL-norepinephrine hydrochloride and dopamine hydrochloride (Sigma-Aldrich, USA);serotonin hydrochloride (Beijing J&K Scientific, China);5-hydroxyindole-3-acetic acid (Tokyo Chemical Industry Co., Ltd., Japan); acetic acid, sodium hydroxide and chromatography methanol [Rionlon Bohua (Tianjin)Pharmaceutical & Chemical Co., Ltd., China]; ultrapure water (Lanzhou University, China).
1.3 Main experimental instruments and materials
PL-200 thermal-inducing pain meter (Chengdu Taimeng Software Co., Ltd., China); acupuncture needle(Suzhou Medical Products Factory Co., Ltd., China);JA1003N precision electronic balance (Jinan Puna Instrument Equipment Co., Ltd., China); L-550 centrifuge (Changsha Hengyu Experimental Instrument Equipment Co., Ltd., China); MDF-382E ultra-low temperature refrigerator (Sanyo Electric Co., Ltd., Japan);LC1620 liquid chromatograph (Shanghai Sunny Hengping Scientific Instrument Co., Ltd, China); RF-530 fluorescence high performance liquid chromatography(HPLC) detector (Shimadzu, Japan); EL-20 acidity meter[Mettler Toledo (Shanghai) Co., Ltd., China]; TGL-16 high speed centrifuge (Jiangsu Jintan Zhongda Instrument Factory, China).
1.4 RA model preparation method
No model was established in the normal group, while the same dose of saline was injected at the same site and same time.
Except the normal group, RA rabbit models in the other three groups were prepared according to the relevant literatures[2-7]: the egg albumin powder was mixed with an equal volume of Freund’s complete adjuvant (CFA) at a concentration of 4 mg/mL. The mixture was shaken thoroughly for about 15 min until it became gelled liquid. Hair on rabbit's back and knee joints was then removed using an electric clipper. Three pairs (6 in total) of injection sites were symmetrically selected between the scapula of rabbit back in the model group, the buccal acupuncture group and the body acupuncture group. Each injection site was injected subcutaneously with 0.2 mL of the gelled liquid.After 14 d, subcutaneous injection was performed again with the same dose at the 6 sites; 0.4 mL of egg albumin saline solution (20 mg/mL) was injected into bilateral hind limb knee joints of the rabbits 7 d later.One week after the injection, decreased food-intake and activity, swelling bilateral knee joints, and significantly reduced pain threshold indicated a successful model.
1.5 Intervention by groups
From the 27th day of the experiment, designated intervention was performed for rabbits in each group,once per day with 10 consecutive interventions.
1.5.1 Normal group
Rabbits in the normal group were fixed on a rabbit table for 30 min each day.1.5.2 Model group
Rabbits in the model group were fixed on a rabbit table every day for 30 min.
1.5.3 Body acupuncture group
Acupoints: Bilateral Dubi (ST 35) and Zusanli (ST 36).
Methods: Acupoint positioning for rabbits was referred to the Experimental Acupuncture Science[8]by analogic acupoint location.
Dubi (ST 35) is at 1 cm lateral to the tibia. Zusanli(ST 36) is at about 1.2 cm below the capitulum fibulae and 1 cm behind the tibia in the dorsolateral lower leg.The rabbits in the body acupuncture group were fixed on a rabbit table to perform perpendicular needling using the needles of 0.25 mm in diameter and 25 mm in length, with twirling manipulation for 15 s at intervals of 5 min. The needles were retained for 30 min and acupuncture was performed once a day.
1.5.4 Buccal acupuncture group
Acupoints: Knee points of bilateral buccal acupunture[at the midpoint between Jiache (ST 6) and Chengjiang(CV 24) in buccal region][9].
Methods: Acupuncture was performed every day after rabbits were fixed on a rabbit table. Needles of 0.25 mm in diameter and 15 mm in length were selected. Oblique needling was performed with twirling manipulation for 15 s at intervals of 5 min. The needles were retained for 30 min and acupuncture was performed once a day.
1.6 Observing analgesic time-effect
High spotlight of the PL-200 thermal-inducing pain meter was used to generate a variable intensity radiation beam to irradiate the rabbit's ear pain test area after infrared filter focus. The struggling action of withdrawing ears in rabbits was used as an indicator of pain response. The latency time from initiating the irradiation to appearing reaction in rabbits was used as the pain threshold (unit: second). It was measured three times, at the intervals of 10 s, and the average value of three times was used as the final pain threshold. Pain thresholds at the time points of 0, 5, 15, 30, 60, 120 and 240 min were measured after the 1st and 10th interventions, respectively (the measured time point was calculated from the acupuncture time, so the first four time points were during needle retaining, while the last three time points were after needle withdrawal).
1.7 Sample collection
After the 10th acupuncture therapy, rabbits were sacrificed by dislocation, and the whole brain was quickly removed on ice to separate the hypothalamus.Blood on the surface of hypothalamus tissues was washed with cold saline and the tissues were dried with filter paper, and placed in a centrifuge tube on ice after accurately weighed using an electronic balance. Nine times of volume of normal saline versus the brain tissues was added into the centrifuge tube to make a rabbit hypothalamic tissue homogenate at a concentration of 10%, and centrifuged immediately at 4 ℃ and 3 000 r/min for 15 min. The supernatant was collected and stored in centrifuge tube at –80 ℃.
1.8 Detecting concentrations of 5-hydroxytryptamine(5-HT) and noradrenaline (NE)
The concentrations of 5-HT and NE in the hypothalamus, at the peak point of pain threshold curve,were determined by HPLC with fluorescence after the 10th acupuncture.
1.9 Statistical processing
All data were analyzed using SPSS version 13.0 statistical software. The normally distributed data were expressed as mean ± standard deviation (±s); the paired t-test was used for comparison in the same group; pairwise comparisons between groups were conducted using one-way ANOVA. Repeated measurements were compared using a multivariate analysis of variance. P<0.05 indicated a statistically significant difference.
2 Experimental Results
2.1 Pain threshold comparison
Pain thresholds at the seven time points in each group after the 1st acupuncture were compared: the pain thresholds in the normal group and the model group showed no significant time-effect feature(P>0.05); the analgesic effect of the buccal acupuncture group and the body acupuncture group showed a significant time-effect feature (P<0.01), i.e., the change in the pain threshold over time showed a time-effect curve of ascending, peaking and descending (Table 1).
The analgesic time-effect in the buccal acupuncture group and the body acupuncture group was significant after the 1st acupuncture (F=15.780, P=0.000), the analgesic effects of the buccal acupuncture group and the body acupuncture group all changed with time. The interaction between time and group was significant(F=16.125, P=0.000), indicating a statistically significant difference in the time variation trend of analgesic effects between the two groups (Table 2).
Pain thresholds at the seven time points within each group after the 10th acupuncture were compared: the pain thresholds of the normal group and the model group showed no obvious time-effect feature (P>0.05).The acupuncture analgesic effect of the buccal acupuncture group and the body acupuncture group showed a significant time-effect feature (P<0.01), i.e.,the change in the pain threshold over time showed a time-effect curve of ascending, peaking, and descending (Table 3).
Table 1. Comparing pain thresholds at different time points after the1st acupuncture (±s, s)

Table 1. Comparing pain thresholds at different time points after the1st acupuncture (±s, s)
Group n 0 min 5 min 15 min 30 min 60 min 120 min 240 min Normal 10 6.71±0.65 6.67±0.48 6.64±0.57 6.69±1.08 6.64±0.88 6.66±1.27 6.90±1.25 Model 10 4.29±0.60 4.29±0.38 4.05±0.75 4.11±0.67 4.09±0.93 4.16±0.52 4.17±0.56 Body acupuncture 10 3.73±1.08 4.04±0.91 5.11±1.83 5.89±1.69 5.41±1.67 4.82±1.37 4.40±1.23 Buccal acupuncture 10 4.10±1.05 4.74±1.40 5.53±1.46 6.00±1.56 5.30±1.52 4.38±1.31 3.87±0.96
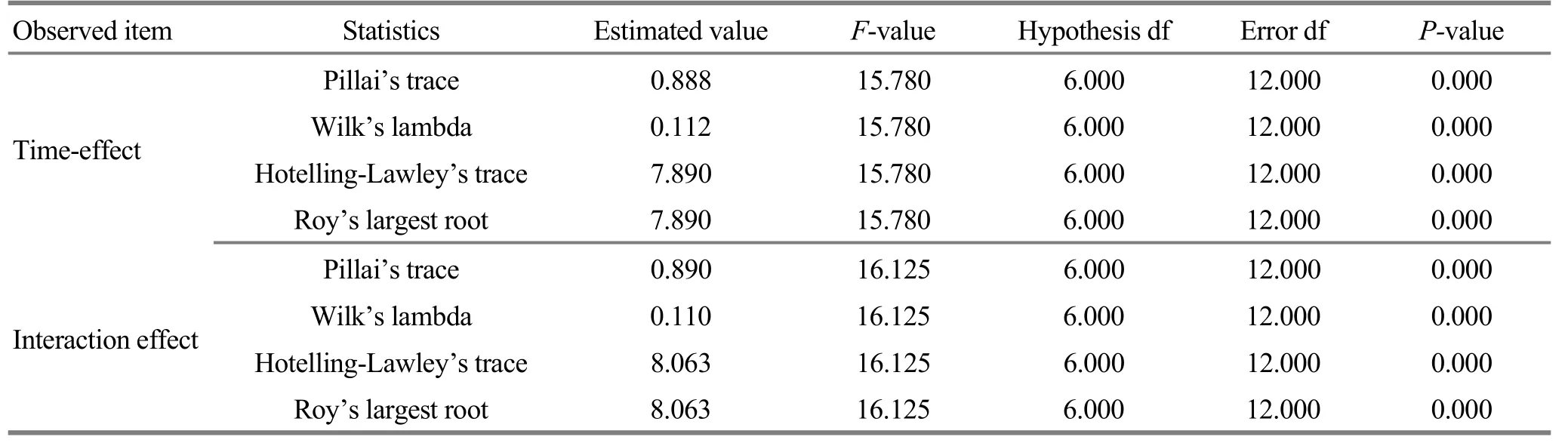
Table 2. Comparing the analgesic time-effect after the 1st acupuncture between the buccal acupuncture group and the body acupuncture group
Table 3. Comparing pain thresholds at different time points after the 10th acupuncture (±s, s)

Table 3. Comparing pain thresholds at different time points after the 10th acupuncture (±s, s)
Group n 0 min 5 min 15 min 30 min 60 min 120 min 240 min Normal 10 6.74±1.05 6.84±1.30 6.66±1.48 6.86±1.76 6.69±1.06 6.91±1.09 6.91±1.04 Model 10 4.29±0.54 4.26±0.56 4.23±0.60 4.23±0.40 4.28±0.40 3.95±0.70 4.16±0.53 Body acupuncture 10 4.13±0.97 4.43±0.93 5.47±1.01 6.71±1.49 6.20±1.79 5.80±1.23 4.91±1.27 Buccal acupuncture 10 4.74±1.01 5.56±1.08 6.06±1.42 6.74±1.24 5.56±1.15 5.06±1.08 4.21±0.98
The analgesic time-effect in the buccal acupuncture group and the body acupuncture group was very significant (F=29.378, P=0.000), and the analgesic effect of the buccal acupuncture group and the body acupuncture group all changed with time; the interaction between time and group was also very significant (F=19.173, P=0.000), indicating a significant difference in the time variation trend of analgesic effects between the two groups (Table 4).
After the 1st and 10th acupuncture in the buccal acupuncture group, the analgesic effects all changed with time (P<0.05). The pain threshold after the 10th buccal acupuncture treatment was significantly higher than that after the 1st buccal acupuncture treatment(P<0.05), (Table 5).
The analgesic time-effects after the 1st and 10th buccal acupuncture treatment were all significant(F=15.473, P=0.000), but the interaction between the time and group was not significant (F=0.973, P=0.486).That is, there was no significant difference in the time variation trend of the analgesic effect between the 1st and the 10th buccal acupuncture treatment (Table 6).
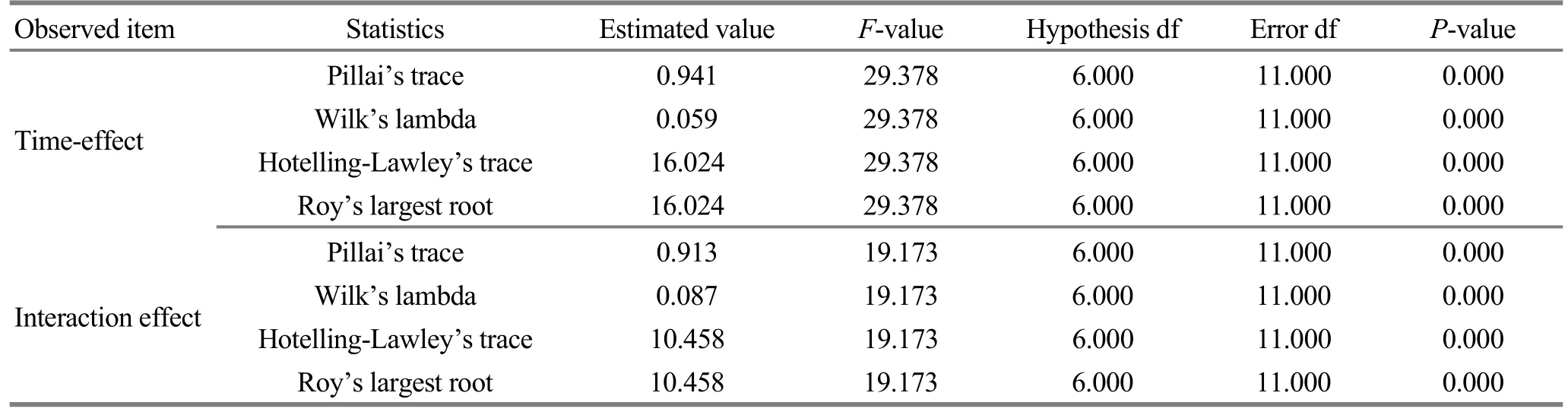
Table 4. Comparing the analgesic time-effect after the 10th acupuncture between the buccal acupuncture group and the body acupuncture group
Table 5. Pain thresholds at different time points in the buccal acupuncture group after the 1st and 10th acupuncture (±s, s)

Table 5. Pain thresholds at different time points in the buccal acupuncture group after the 1st and 10th acupuncture (±s, s)
?
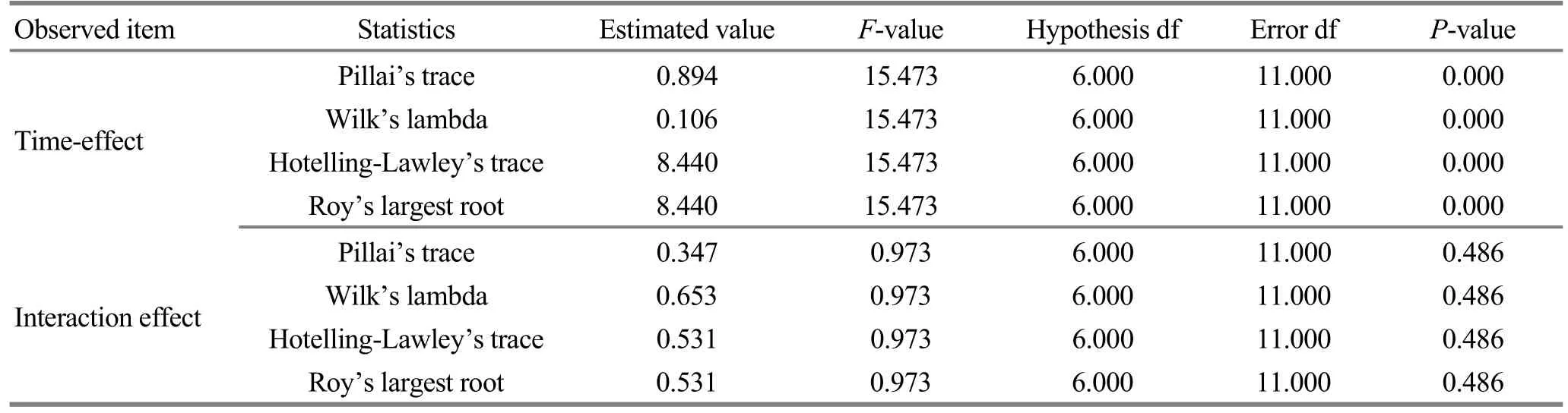
Table 6. Comparison of analgesic time-effect changes in the buccal acupuncture group between the 1st and 10th acupuncture
2.2 Comparing 5-HT and NE concentrations and NE/5-HT ratio in the thalamus
The 5-HT concentration in the model group was significantly lower than that in the normal group, and the difference was statistically significant (P<0.05). After the treatment, compared with the model group, the 5-HT concentrations in the rabbit’s hypothalamus in the buccal acupuncture group and the body acupuncture group were significantly increased, and the differences were statistically significant (all P<0.05). The increase in the body acupuncture group was more significant compared with that in the buccal acupuncture group but without statistical significance (P>0.05), (Table 7).
NE concentration of the model group was lower than that of the normal group, and the difference was statistically significant (P<0.05). After the treatment,compared with the model group, the NE concentration in hypothalamus of the body acupuncture group was increased, and the difference was statistically significant(P<0.05); the NE concentration in rabbit’s hypothalamus in the buccal acupuncture group was decreased, and the difference was statistically significant (P<0.05),(Table 7).
NE/5-HT ratio of the model group was higher than that of the normal group, and the difference was statistically significant (P<0.05). After the treatment,compared with the model group, the hypothalamic NE/5-HT ratios of the buccal acupuncture group and the body acupuncture group were all decreased, and the differences were statistically significant (all P<0.05),(Table 7).
Table 7. Comparison of 5-HT and NE concentrations and NE/5-HT ratio in rabbit’s hypothalamus (±s)
Note: Compared with the normal group, 1) P<0.05; compared with the model group, 2) P<0.05, 3) P<0.01
Group n 5-HT (ng/mL) NE (ng/mL) NE/5-HT Normal 10 3.567±0.737 36.167±2.83 10.42±2.30 Model 10 2.067±0.151) 27.867±0.751) 13.51±0.691)Body acupuncture 10 2.833±0.312) 30.000±0.302) 10.67±1.172)Buccal acupuncture 10 2.700±0.262) 25.033±1.612) 9.35±1.353)
3 Discussion
Buccal acupuncture is a method to needle specific acpoints in buccal region. It is guided by the bioholographic theory and a brand-new microacupuncture therapy discovered by Dr. Wang Yong-zhou,Professor Fang Xiao-li and their research team through the clinical practice[9]. Existing clinical studies have shown that the treatment effect of buccal acupuncture on painful diseases is significant. Buccal acupuncture has the advantages of rapid pain relief, easy operation,high safety and wide indications[10-13]. The preliminary basic research found that the buccal acupuncture could up-regulate the concentration of β-endorphin (β-EP) in cerebrospinal fluid and recover the concentration of cholecystokinin octapeptide-8 (CCK-8) to the normal level. This may be one of the central mechanisms of buccal acupuncture analgesia[14-16].
Buccal acupuncture can treat RA by regulating multiple signal transduction pathways, and regulating various proteins in rabbit cerebrospinal fluid, suggesting that buccal acupuncture has multi-target therapeutic mechanisms[17].
The results of this experiment showed that the analgesic effects of the buccal acupuncture group and the body acupuncture group all changed with time, and at the time point of 5 min, there was a statistically significant difference between the two groups (P<0.05);at the time point of 240 min, the difference in pain threshold was also statistically significant (P<0.05). This indicated that the analgesic effect of the buccal acupuncture had a significant time-effect. The timeeffect curves of the analgesic effects in the buccal acupuncture group and the body acupuncture group were similar, but there were significant differences. In general, buccal acupuncture showed a rapid pain relief,and rapid increase and decline in pain threshold. Body acupuncture showed a slow onset of analgesia, and slow increase and decline in pain threshold.
From the anatomic structure of acupoints for the buccal acupuncture, the nerves distributed in the acupoints are mainly the trigeminal and facial nerves.The facial nerves are mixed nerves and dominate facial expression movements. The main component is the movement fiber. The sensory part is the intermediate nerve and mainly composed of special visceral sensory fibers (i.e., taste fibers) and a small amount of general somatosensory fibers, which mainly dominate the taste and secretion of glands (salivary glands and lacrimal glands). Therefore, the facial nerves are not the main pathways for the afferent buccal acupuncture signal.
The trigeminal nerve is a mixed nerve and composed of sensory and motor fibers, and the main sensory nerve in the face. The sensory fibers are responsible for the feelings of the face, mouth cavity and the front of the calvaria; and the motor fibers dominate the movement of the masticatory muscles. Studies have shown that the analgesic effect of acupuncture on facial acupoints disappears when the trigeminal nerve is blocked with anesthetics, indicating that trigeminal nerve is the main afferent pathway of acupuncture signal for facial acupoints. The analgesic effect of puncturing facial acupoints is mainly caused by transition of acupuncture signal through the trigeminal nerve into the high-level site of the central nervous system[18].
The analgesic effects of buccal acupuncture and body acupuncture had similar time-effect curves, suggesting that the analgesic effects of buccal acupuncture and body acupuncture may have similar neurophysiological mechanisms; but the buccal acupuncture signal is directly transmitted from the trigeminal nerve (as the main pathway) to the central nervous system, including brainstem, thalamus and cerebral cortex, this results in the analgesic effects by interacting and synthesizing with the pain signals at all levels while the body acupuncture signal is first transmitted from the peripheral nerves to the spinal cord where it is integrated, and then transmitted along the ventrolateral spinal cord to the high level centers where it interacts with the pain signals to exert analgesic effects. It is suggested that the difference in afferent pathways between buccal acupuncture and body acupuncture may be one of the mechanisms causing the differences in the analgesic time-effect curves.
The results of this experiment showed that with the buccal acupuncture treatment, the pain threshold after the 10th acupuncture was significantly higher than that after the 1st acupuncture, but the analgesic effect over time was consistent and did not change with the number of treatment, indicating that the analgesic effect of buccal acupuncture has an inherent, specific time-effect curve, which does not change with the number of treatment.
The results of this experiment showed that: after treatment, compared with the model group, the 5-HT concentrations in the rabbit’s hypothalamus in the buccal acupuncture group and the body acupuncture group were significantly increased; the NE concentration in hypothalamus in the body acupuncture group was increased, and NE concentration in hypothalamus was decreased in the buccal acupuncture group; hypothalamic NE/5-HT ratios were decreased in both groups. Previous studies have shown that central 5-HT plays an important role in acupuncture analgesia, and NE in the brain resists acupuncture analgesia. During acupuncture analgesia,the synthesis, release, and utilization of 5-HT in the brain are increased, but the synthesis is more than consumption, so the 5-HT concentration in the brain is increased[19]. The results of our current experiment are consistent with previous research results. The data showed that the concentrations of 5-HT in the brain were increased after both buccal acupuncture and body acupuncture. There was no significant difference in the effect on 5-HT between the two different acupuncture methods. Both methods could down-regulate the NE/5-HT ratio to the normal level which was elevated after modeling. The existing studies on the renewal rate of neurotransmitter in the brain have shown that,during acupuncture analgesia, the synthesis, release and use of NE in the brain are all increased, but the use is more than synthesis, so the NE concentration in the brain is reduced[19]. However, the results of current experiment showed that compared with the model group, the NE concentration in brain in the buccal acupuncture group was decreased, and NE concentration in the body acupuncture group was increased. This may be caused by the higher consumption rate of NE than the synthesis rate in the brain after buccal acupuncture, resulting in lower NE concentration in rabbit brain after acupuncture than in the model group.
In summary, the analgesic effect of the buccal acupuncture has an inherent and specific time-effect curve. The buccal acupuncture can affect the concentration of monoamine neurotransmitters, which may be another mechanism of the neurochemical central role of the buccal acupuncture analgesia.
Conflict of Interest
The authors declared that there was no potential conflict of interest in this article.
Acknowledgments
This work was supported by National Natural Science Foundation of China (国家自然科学基金项目, No.81260559).
Statement of Human and Animal Rights
The treatment of animals conformed to the ethical criteria in this experiment.
Received: 15 October 2017/Accepted: 13 November 2017
猜你喜欢
杂志排行
Journal of Acupuncture and Tuina Science的其它文章
- Modern quantum theories and experimental achievements motivate new exploration of acupuncture in traditional Chinese medicine
- Application and exploration of suspended magnetic moxibustion cup for obesity
- Therapeutic efficacy observation on acupuncture for persistent allergic rhinitis
- Correlation analysis on clinical effects of acupuncture for elderly patients with sensorineural deafness and ear distending sensation
- Effect of Governor Vessel-unblocking and mindrefreshing acupuncture plus functional training on neural development in infants with brain damage
- Effects of acupuncture on ovarian blood supply and pregnancy outcomes in patients receiving assisted reproduction