The Surgical Management of Ebstein Anomaly
2018-07-04KarlReyesMDEricHunJengMDMBASusanCookePADavidHallMDandMarkBleiweisMDUniversityofFloridaCongenitalHeartCenterCongenitalHeartSurgery600SouthwestArcherRoadGainesvilleFL3608USA
Karl M.Reyes, MD, Eric l-Hun Jeng, MD, MBA, Susan Cooke, PA-C, David Hall, MD and Mark S.Bleiweis, MDUniversity of Florida, Congenital Heart Center, Congenital Heart Surgery, 600 Southwest Archer Road, Gainesville, FL 3608, USA
2University of Florida, Department of Surgery, Division of Thoracic and Cardiovascular Surgery, 1600 Southwest Archer Road, Gainesville, FL 32608, USA
Anatomy
Ebstein anomaly comprises about 1% of all congenital heart disease.Almost all cases are sporadic,although it has been associated with maternal lithium therapy [1].It is a malformation of the tricuspid valve (TV) and right ventricle (RV) and is characterized by: (a) failure of delamination of the septal and posterior leaflets resulting in adherence of the leaflets to the myocardium, (b) downward or apical displacement of the tricuspid annulus, (c) “atrialization” of a portion of the RV, (d) anterior leaflet “saillike” redundancy, tethering and fenestrations; and(e) dilatation of the right atrioventricular (annular)junction [2, 3] (Figure 1).
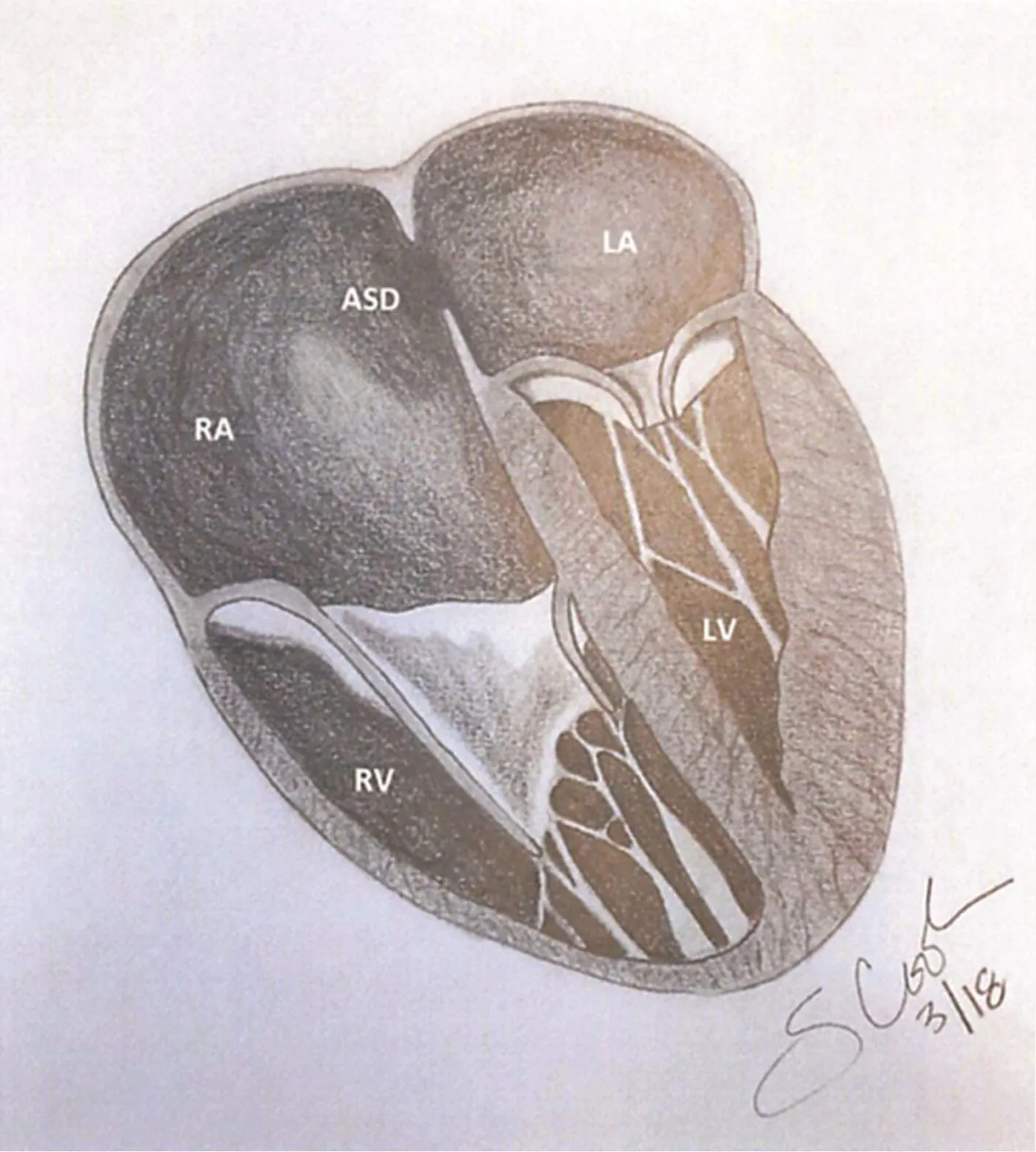
Figure 1: In Ebstein Anomaly, there is Failure Delamination of the Tricuspid Leaflet, a “Sail-Like’’ Anterior Leaflet, Downward Displaced of the Tricuspid Annulus,“Atrialization” of a Portion of the Right Ventricle, and Dilatation of the Tricuspid Annulus.
In normal hearts, there is a downward displacement of the septal and posterior leaflets in relation to the mitral leaflet of less than 8 mm/m2body surface area [2].However, in Ebstein anomaly there is a wide range of displacement of the posterior and septal leaflet from mild to complete tethering or an imperforate membrane or muscular shelf between the inlet and trabecular areas of the RV.The anterior leaflet is generally described as large, redundant and“sail-like”; and may contain fenestrations.Chordae are poorly developed and short and may not completely support the anterior leaflet.Occasionally,severely deformed anterior leaflets may obstruct the right ventricular outflow tract.These abnormal pathologies all contribute to the varying degrees of severity of tricuspid regurgitation.As for the anatomic TV annulus, it is usually severely dilated.The functional RV is often not located below the anatomic TV annulus but an “atrialized” portion often separates the true TV annulus from functional RV.The distinction between the “atrialized” portion and the functional RV is made by observing the appearance of the right ventricular wall.The “atrialized”RV will have a smooth myocardium that is dyskinetic, while functional RV will have a trabeculated myocardium.Furthermore, on inspection of the surface coronary anatomy, the right coronary artery is at the level of the true TV annulus that corresponds with the true atrioventricular junction.
In Ebstein anomaly, the RV is divided into two regions: the inlet region which is the area involved in the malformation and functionally part of the right atrium (RA), and the trabecular and outlet region which is the functional component of the RV.The severity of function of the RV is greatly dependent on the volume of the trabecular and outlet regions.In severe forms of Ebstein anomaly,the volume of the “atrialized” portion of the RV is significantly dilated and larger (more than half) than the trabecular and outlet region and this results in severely depressed RV function.In severe cases of right ventricular dilation, the dilation is not solely from the “atrialized” portion.The functional portion also becomes dilated and this is usually at the apex and outflow tract.Left ventricular function can also be severely impacted when there is severe right ventricular dilatation through compression of the left ventricular chamber and occasionally through left ventricular outflow tract obstruction [4].
Other forms of congenital heart disease may be present along with Ebstein anomaly.Interatrial communications are most common [4], and other right-sided lesions such as pulmonary stenosis or pulmonary atresia, as well as branch pulmonary artery stenosis and patent ductus arteriosus, are also frequently seen.The most commonly associated arrhythmias are from accessory conduction pathways (Wolf Parkinson White syndrome) often seen in younger patients and atrial fl utter or fi brillation which is often seen in older patients [5, 6].
Classification Systems
outflow tract obstruction;and in Type D there is almost complete atrialization of the RV with a small infundibular component [7].
In neonates, Celermajer et al.[8] described an echocardiographic grading score, the extended Glasgow Outcome Scale.It is the ratio of combined right atrium and atrialized RV to the functional RV and left heart ratio with grades between 1 and 4.It is used as an as objective criterion for mortality risk (Grade 1 is a ratio of <0.5.Grade 2 has a ratio between 0.5 and 0.99.Grade 3 has a ratio 1.0–1.49.Grade 4 has a ratio >1.5).
Pathophysiology and Clinical Presentation
The principal abnormality in patients with Ebstein anomaly is the decrease or lack of fl ow through the right side of the heart due to impaired RV contractility and tricuspid regurgitation.The impaired contractility is a result of a lack of functioning RV which progressively worsens as the right side of the heart is volume loaded and the RV progressively dilates even further, worsening contractility.The incompetence of the TV also results in dilation of both the RA and RV.The right ventricular dysfunction in the presence of an atrial level communication results in right to left shunting of blood with arterial desaturation.
The proportion to which the right atrium and ventricle can dilate is immense.In neonates with severe Ebstein anomaly, the chest X-ray may show a socalled “wall-to-wall” heart.Worrisome in neonates is not only the severity of cardiac enlargement, but also the retarded effect on pulmonary development and function that can be caused by lack of adequate pulmonary blood fl ow.Beyond the neonatal and infancy period are where most diagnosis of Ebstein anomaly is made.These are infants,children and adults with varying but lesser degrees of right ventricular dysfunction and tricuspid regurgitation.They will usually present with symptoms such as exertional dyspnea, fatigue, cyanosis or palpitations.Others, especially children greater than 10 years and adults may present with arrhythmias[8].However, many remain completely asymptomatic and are incidentally found.Rarely, adults will present with another medical condition such as paradoxical embolization from right to left shunting of an interatrial communication as their initial presenting symptom [9].
Given the varying presentations, there are no specific physical examination findings pathognomonic for Ebstein anomaly.Cyanosis may be present especially in symptomatic neonates or none at all in the asymptomatic child or adult.Signs of right sided heart failure such as jugular venous distention and hepatic congestion may be present in advanced cases, or none at all when the RA and RV is highly compliant.Regurgitation murmurs are usually soft if present due to large coaptation gaps, low right ventricular pressures and low velocity fl ows across the tricuspid valve and right ventricular outflow tract.Given all of the above, a patient may walk in completely asymptomatic and all that is found is a split-second heart sound from conduction delay and this will be the only physical finding that will point to a severe form of congenital heart disease; thus vigilance and a low threshold should be present for additional diagnostic testing in the presence of any suspicious findings.
Diagnosis
Two-dimensional echocardiography is the diagnostic test of choice for Ebstein anomaly.Principal features are: (a) apical displacement of the septal leaflet from the insertion of the mitral leaflet by at least 8 mm/m2body surface area [2], and (b) failure of delamination with points of tethering between leaflets and underlying myocardium causing restriction of motion [10] (Figure 2).In the recent era,3D echocardiography has become an important adjunct in analysis of the TV leaflets and subvalvar apparatus.This has been particularly important for pre-operative planning of valve reconstruction.

Figure 2: Two-Dimensional Echocardiographic Image of a Patient with Ebstein Anomaly.
As for cardiac catheterization, this is now rarely performed.The indications for cardiac catheterization are for hemodynamic assessment of left ventricular function, measurement of pulmonary artery pressure and pulmonary vascular resistance, and for coronary angiography in older patients.On the other hand, cardiac magnetic resonance imaging(MRI) has become routine and provides the most objective quantitative measurement of right atrial and right ventricular size and function [11].Our policy is to perform MRI in all patients beyond the neonatal period to evaluate adequacy of right ventricular function prior to surgical therapy.
Other exams include the chest X-ray which still remains an important initial imaging study.In symptomatic neonates, massive cardiomegaly (wall-towall heart) can be seen; and beyond the neonatal period, there will be varying degrees of cardiac enlargement and the heart is usually described as globe shaped with a narrow waist.An enlarged right atrial silhouette is also usually seen and the lung fi elds may show normal of decreased vascularity due to hypoplasia.Typical electrocardiography(ECG) findings are the following: (a) prolonged PR interval, (b) tall P waves and (c) right bundle branch block.First degree AV block is another frequent finding.Atrial fi brillation or fl utter is common in older patients and accessory conduction pathways are less common overall but typically will be found earlier on [5, 6].
Management
The surgical management of Ebstein anomaly is principally dependent on the severity at presentation.It is basically a dichotomous approach where either the patient presents with right sided heart failure at birth that cannot be medically managed and will be considered for conversion to single ventricle physiology; or the patient presents beyond the neonatal period with varying degrees of tricuspid regurgitation and right sided dysfunction and will be amenable to TV repair and right ventricular reconstruction.In select patients, biventricular repair in the neonatal period may be performed [11].Also, in patients with borderline right ventricular function,the addition of a bidirectional Glenn shunt to a TV repair off loads the right ventricle by permitting direct passive passage of blood to the pulmonary circulation (1.5 ventricle repair).For patients who present in adulthood with late severe right or biventricular dysfunction, heart transplantation is the remaining option.
In the neonate, evaluation begins ideally in the prenatal period.Prenatal diagnosis can be made by fetal echocardiography typically at 18–20 weeks of gestation.Generally, most fetuses tolerate pregnancy well, however rarely fetal hydrops can develop.Of great concern during the neonatal period is extreme cardiomegaly causing impaired pulmonary development.Another important factor is the presence of anatomic or functional obstruction of the right ventricular outflow tract.After delivery, assessment of degree of right ventricular failure and cyanosis is done; and if medical therapy can optimize the neonate.If medical management is unsuccessful, and typically these are neonates who are profoundly cyanotic, with a Great Ormond Street Score 3 or 4,cardiothoracic ratio >80% and severe TR [12] with a dysfunctional RV, functional pulmonary atresia with left ventricular due to massive right ventricular dilatation; RV exclusion with fenesterated patch closure of the TV orifice, atrial septectomy, right atrial reduction and right modified Blalock-Taussig shunt is performed [13].Additionally, main pulmonary artery ligation is performed if there is severe pulmonary regurgitation.This procedure, also called the Starnes procedure, essentially abandons the right ventricle and converts to a single ventricle physiology.Mortality with this operation can be high but they are merely reflective of the severity of the ongoing disease process.
For patients who survive or are diagnosed beyond the neonatal period, this subset is inherently of a less critical nature and will have varying degrees of TV regurgitation and right ventricular dysfunction.In the majority of these patients, they will ultimately require surgical intervention; however, timing of surgery depends on multiple factors.In our practice, we recommend surgery when symptoms of cyanosis, fatigue, exercise intolerance, progressive right ventricular dilatation and/or worsening tricuspid regurgitation are present.We also offer surgery to asymptomatic or mildly symptomatic patients with adequate right ventricular function and severe tricuspid regurgitation where preoperative imaging studies predict a high probability for successful repair.With this strategy, the aim is to both improve right ventricular function and TV competence, and also to optimize preservation of right ventricular function and prevent early heart failure.
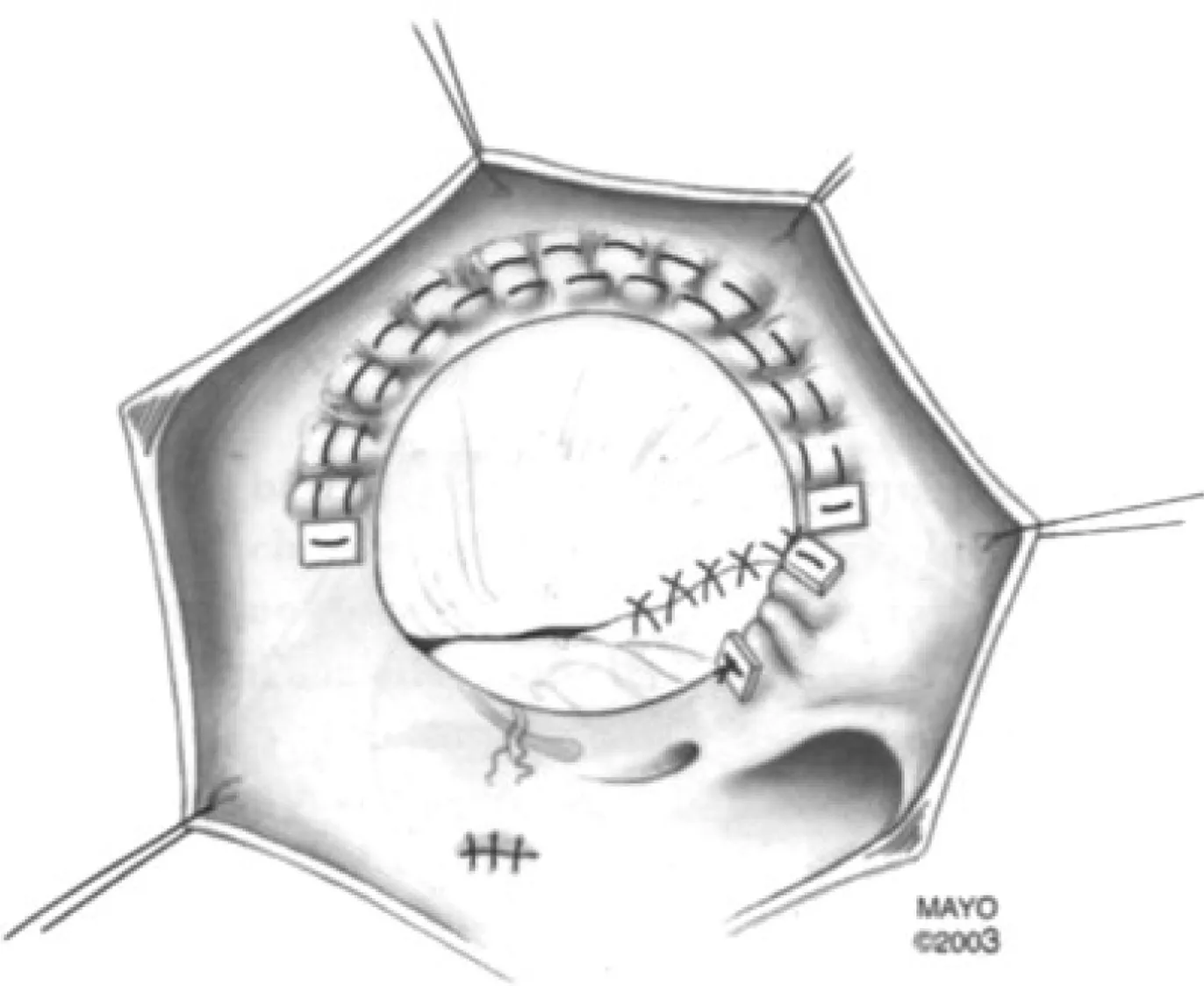
Figure 3: The Danielson Technique for Tricuspid Valve Repair in Ebstein Anomaly.
Popular techniques used in the past for tricuspid valve repair include the Mayo Clinic (Danielson)method [14] (Figure 3) and the Carpentier method[7, 15].Both surgical techniques utilized a monocusp concept and selective RV plication.Current or contemporary concepts, while also involving selective RV plication, now focus not just on tricuspid leaflet reconstruction, but the restoration of a more anatomic right ventricle.This contemporary concept of tricuspid repair, the Cone reconstruction, was conceptualized by da Silva et al.[16] (Figure 4).This technique involves detachment and delamination of anterior, septal and posterior leaflet tissue,rotation and reattachment of the recruited leaflet tissue at the true atrioventricular junction/tricuspid valve annulus thereby creating a 360 degree leaflet“cone,” plication of the tricuspid annulus to reduce its size, and internal plication of the “atrialized” ventricle.If the anterior leaflet subvalvar apparatus is rudimentary and not well-formed, additional fenestrations are made on the anterior leaflet.In patients with borderline right ventricular function, a small atrial septal defect (5 mm) is created to allow “popof ” into the left ventricle when there is worsening of RV function during the postoperative period.In older patients, a tricuspid annuloplasty ring is used to stabilize the repair.The Cone reconstruction may not be appropriate in patients older than 55–60 years with moderate pulmonary hypertension, significant left ventricular dysfunction (LVEF <30%), absent septal leaflet, a rudimentary or poorly developed anterior leaflet and severe RV dysfunction or enlargement.In these patients, successful rehabilitation of the right ventricle is unlikely and othotopic heart transplantation is a viable alternative.Furthermore,when tricuspid valve repair cannot be performed in the presence of adequate right ventricular function,tricuspid valve replacement with a porcine valve continues to be an excellent option [17].
Adjunctive procedures may also be performed in addition to tricuspid valve repair and right ventricular reconstruction.Selective use of the 1.5 ventricle repair through creation of a bidirectional cavopulmonary shunt (Glenn shunt) in patients with significant RV enlargement or dysfunction and/or moderate tricuspid valve stenosis (mean gradient greater than 8 mmHg) decreases the volume entering the right ventricle by 35–45%.This provides substantial unloading to the right ventricle and reduces stress on the tricuspid valve repair and improved loading of the left ventricle [18, 19].This may not be appropriate in patients with severe left ventricular dysfunction where it cannot be determined if the dysfunction is secondary to the right ventricular compression.The pulmonary pressures,pulmonary vascular resistance and left atrial pressures should be documented to be low prior to proceeding with cavopulmonary shunt.
Lastly, arrhythmia management is an important component of treating Ebstein anomaly.Routine preoperative electrophysiologic studies should be performed, and ablation of all accessory conduction pathways should be done at the electrophysiology lab prior to surgical repair.Surgical ablation of supraventricular tachyarrythmias has also been described and may be performed at the time of tricuspid valve repair [5, 20].Specific arrhythmia procedures at the time of surgery are the use of cryoablation and radiofrequency ablation to perform a modified right sided maze and cavotricuspid isthmus ablation.This is done for paroxysmal atrial fi brillation or fl utter.For chronic atrial fi brillation, a left atrial maze or pulmonary vein isolation is done[5, 6].Rarely, patients who develop complete heart block will need a permanent pacemaker.We prefer epicardial leads with left ventricular pacing because of better reliability of pacing the left over the right ventricle in Ebstein anomaly.
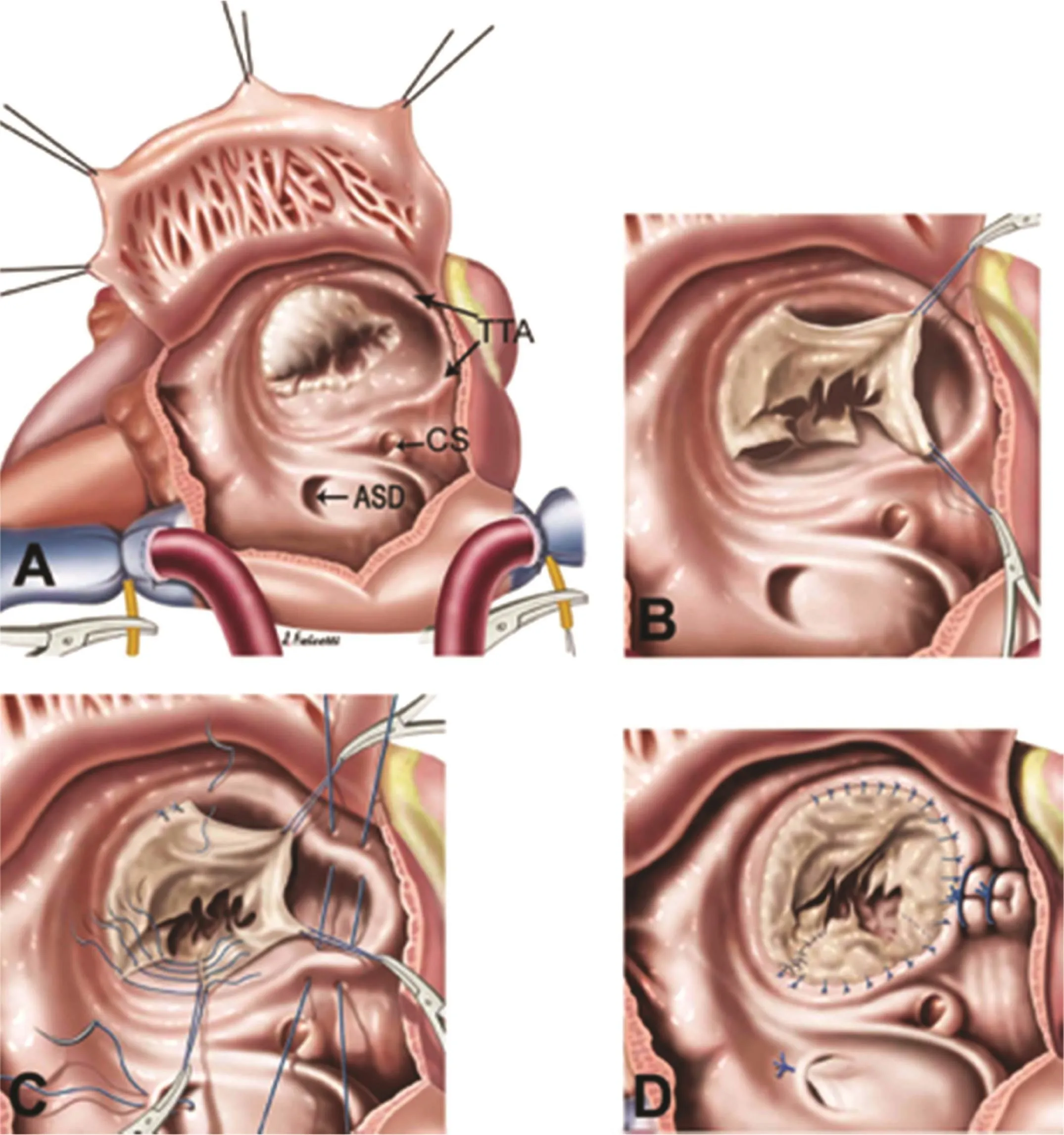
Figure 4: The Cone Reconstruction for Ebstein Anomaly.
Results
Advances both in operative techniques and postoperative management have contributed greatly to improved outcomes for patients with Ebstein anomaly.One of the largest experiences to date at the Mayo Clinic reported outcomes in 539 patients where they demonstrated excellent 10 and 20-year long term survival of 84.7 and 71.2%, respectively, and freedom from late reoperation at 10 and 20 years of 74.1 and 46.1%, respectively.Majority of patients (83%) remained in NYHA functional class I or II at late follow up [4].
The Cone reconstruction has by far been the contemporary tricuspid valve repair of choice for Ebstein anomaly.Its more “anatomic” reconstruction has drawn much favor due to the perceived benef its of restoring the tricuspid valve to its native annulus and having more available right ventricular myocardium which may help improve its function.The early-to-intermediate results have been promising with outcomes at 4 years follow up showing significant improvement in TV regurgitation and NYHA Functional Class with low in-hospital mortality (2.5%) [16].
Conclusion
Ebstein anomaly is a very rare form of congenital heart disease.It can present in every age group and its clinical severity strongly correlates with the age of presentation.Patients requiring neonatal surgery indicate severe disease and high operative mortality,while patients presenting after the neonatal period have low operative mortality and will have excellent quality of life despite a higher frequency of repeat interventions.In infants up to adults, we recommend surgery for nearly all patients with at least moderate tricuspid regurgitation and varying degrees of right ventricular dysfunction with the goal of preserving long-term right ventricular function.Adjunctive procedures such as the bidirectional cavopulmonary anastomosis and ablations for arrhythmia are performed after careful evaluation of their indications.The continued challenge however is in neonates with poorly functioning ventricles, younger patients with recurrent TR and progressively worsening right ventricular function, and late presenting patients with severe biventricular function.In these patients, the most important goal is to preserve ventricular function as long as possible as there may be no recourse but to await transplantation.
Disclosure Statement
All of the authors including Eric Jeng, Karl Reyes,Susan Cooke, David Hall, and Mark Bleiweis are in agreement with the content in the manuscript.There are no sources of financial support in the form of grants, equipment, and/or pharmaceutical items for this research.
Conflict of lnterest
The authors declare that they have no conflicts of interest.
REFERENCES
1.Cohen LS, Friedman JM, Jefferson EM, Weiner ML.A reevaluation of risk of in utero exposure to lithium.J Am Med Assoc 1994;271:146–50.
2.Edwards WD.Embryology and pathologic features of Ebstein’s anomaly.Prog Pediatr Cardiol 1993;2:5–15.
3.Dearani JA, Danielson GK.Ebstein’s anomaly of the tricuspid valve.In: Mavroudis C, Backer CL,editors.Pediatric cardiac surgery.3rd ed.Philadelphia, PA: Mosby;2003.pp.524–36.
4.Brown MI, Dearani JA, Danielson GK, Cetta F, Connolly HM, Warnes CA, et al.The outcomes of operations for 539 patients with Ebstein anomaly.J Thorac Cardiovasc Surg 2008;135(5):1120–36.
5.Khositseth A, Danielson GK,Dearani JA, Munger TM, Porter CJ.Superventricular arrhythmias in Ebstein anomaly: management and outcome.J Thorac Cardiovasc Surg 2004;128(6):826–33.
6.Stulak JM, Sharma V, Cannon BC,Ammash N, Schaff HV, Dearani JA.Optimal surgical ablation of atrial tachyarrhythmias during correction of Ebstein anomaly.Ann Thorac Surg 2015;99(5):1700–5; discussion 1705.
7.Carpentier A, Chauvaud S, Mace L,Reilland J, Mihaileanu S, Marino JP,et al.A new reconstructive operation for Ebstein’s anomaly of the tricuspid valve.J Thorac Cardiovasc Surg 1988;96:92–101.
8.Celermajer DS, Bull C, Till JA,Cullen S, Vassilikos VP, Sullivan D,et al.Ebstein’s anomaly: presentation and outcome from fetus to adult.J Ann Coll Cardiol 1994;23:170–6.
9.Attenhofer Jost CH, Connolly HM,Scott CG, Burkhart HM, Ammash NM, Dearani JA.Increased risk of possible paradoxical emobolic events in adults with Ebstein anomaly and severe tricuspid regurgitation.Congenit Heart Dis 2014;9(1):30–7.
10.Roberson DA, Silverman NH.Ebstein’s anomaly: echocardiographic and clinical features in the fetus and neonate.J Am Coll Cardiol 1989;14:1300–7.
11.Knott-Craig CJ.Management of neonatal Ebstein’s anomaly.Oper Tech Thorac Cardiovasc Surg 2004;9:194–207.
12.Boston US, Goldberg SP, Ward KE,Overholt ED, Spentzas T, Chin TK,et al.Complete repair of Ebstein anomaly in neonates and young infants: a 16 year follow-up.J Thorac Cardiovasc Surg 2011;141:1163–9.
13.Starnes VA, Pirlick PT, Bernstein D, Griffin ML, Choy M, Shumway NE.Ebstein anomaly appearing in the neonate.A new surgical approach.J Thorac Cardiovasc Surg 1991;101(6):1082–7.
14.Dearani JA, Danielson GK.Tricuspid valve repair for Ebstein’s anomaly.Oper Tech Thorac Cardiovasc Surg 2003;8:188–92.
15.Chauvaud S.Ebstein malformation.Surgical treatment and results.Thorac Cardiovasc Surg 2000;48(4):220–3.
16.Da Silva P, Baumgrauz FJ, Fonseca L, Franchi SM, Lopes LM, Tavares GM, et al.The cone reconstruction of the tricuspid valve in Ebstein anomaly.The operation: early and midterm results.J Thorac Cardiovasc Surg 2007;133(1):215–23.
17.Brown ML, Dearani JA, Danielson GK, Cetta F, Connolly HM, Warnes CA, et al.Comparison of the outcome of porcine bioprosthetic versus mechanical prosthetic replacement of the tricuspid valve in Ebstein anomaly.Am J Cardiol 2009;103(4):555–61.
18.Raju V, Dearani JA, Burkhart HM,Grogan M, Phillips SD, Ammash N, et al.Right ventricular unloading for heart failure related to Ebstein malformation.Ann Thorac Surg 2014;98(1):167–73; discussion 173–4.
19.Malhotra SP, Petrossian E, Reddy VM, Qiu M, Maeda K, Suleman S, et al.Selective right ventricular unloading and novel technical concepts in Ebstein anomaly.Ann Thorac Surg 2009;88(6):1975–81;discussion 1981.
20.Greason KL, Dearani JA, Theodoro DA, Porter CB, Warnes CA,Danielson GK.Surgical management of atrial tachyarrythmias associated with congenital cardiac anomalies: Mayo Clinic experience.Semin Thorac Cardiovas Surg Pediatr Card Surg Annu 2004;6:59–71.
杂志排行
Cardiovascular Innovations and Applications的其它文章
- Pulmonary Arterial Hypertension Medical Management of the Adult Patient with Congenital Heart Disease
- The Pulmonary Hypertension Story
- Evaluation of Left Ventricular Systolic Function after Pulmonary Valve Replacement Using Cardiovascular Magnetic Resonance lmaging
- Pregnancy in Congenital Heart Disease:A Review for the General Cardiologist
- Atrial Arrhythmias lncluding Atrial Fibrillation in Congenital Heart Disease: Mechanisms,Substrate ldentification and lnterventional Approaches
- Heart Transplantation for Adult Congenital Heart Disease: Overview and Special Considerations