The Pulmonary Hypertension Story
2018-07-04RichardContiMDMACCandRobertHamburgerDOMPH
C.Richard Conti, MD, MACC and Robert Hamburger, DO, MPH
lntroduction
Pulmonary hypertension is not a single entity and not all forms have the same prognosis.
The purpose of this editorial is to provide information to the general cardiologist relating to which type of pulmonary hypertension the patient is experiencing.In order to do this properly, one must determine the cause, the severity, the prognosis, and develop treatment plans for the different forms of pulmonary hypertension.
Pulmonary Arterial Hypertension
Pulmonary arterial hypertension (PAH) is the most malignant of the different types of pulmonary hypertension.While typically being diagnosed in a younger population than the other types, PAH may be showing a trend towards diagnosis later in the life than what was thought from older registry data[1].The usual causes of cardiovascular death in patients with PAH includes right heart failure and sudden death [2].
Secondary Pulmonary Hypertension
There are multiple causes of what used to be called secondary pulmonary hypertension.One must be aware that there are some surgical and nonsurgical treatable causes of marked pulmonary hypertension–e.g.pulmonary emboli, chronic lung disease, rheumatoid diseases, sarcoid, etc.Left Heart causes of pulmonary hypertension include chronic systolic and diastolic heart failure, pulmonary venous obstruction, cor triatriatum, and mitral valve stenosis and or regurgitation.Echocardiography can usually detect left heart causes of treatable secondary pulmonary hypertension.
Definitive Diagnosis of Pulmonary Hypertension
The definitive diagnosis of pulmonary hypertension requires right heart catheterization with a mean pulmonary arterial pressure (mPAP) greater than 25 mm of mercury [3].
Pre-Capillary Pulmonary Hypertension
Those with pulmonary hypertension related to precapillary changes have elevated PA pressures but they have a pulmonary capillary wedge pressure(PCWP) of less than 15 mmHg.
If present and with other causes of pre-capillary pulmonary hypertension ruled out such as by a negative V/Q scan (ruling out Group 4) or absence of chronic lung disease or sarcoidosis, the diagnosis of Group 1 pulmonary arterial hypertension is suggested.
Post Capillary Changes
Post capillary pulmonary hypertension patients also have a mean PA pressure greater than 25 mmHg but a PCWP of greater than 15 mmHg.Thus the pulmonary hypertension is due to left heart disease(type 2), or pulmonary hypertension with unclear and or multifactorial mechanisms (type 5).
Group 2 pulmonary hypertensionis supported by the presence of mPAP greater than 25 mmHg with a PCWP greater than 15 mmHg.There are commonly scenarios in which an elevated PCWP is present along with an elevated PVR greater than 3 Wood units in which case a mixed etiology of pulmonary hypertension may be present.
Group 3 pulmonary hypertensionis due to chronic lung disease.Patients usually are hypoxemic and have lung abnormalities on Chest X-ray or CT scan e.g.emphysematous lungs and abnormal pulmonary function tests.
Group 4 pulmonary hypertensionis related to chronic thromboembolic pulmonary hypertension(CTEPH).This diagnosis may be suggested by an abnormal V/Q scan in the presence of signs/symptoms of right ventricular strain.It is critical to establish this diagnosis as it is potentially curable by pulmonary thromboendarterectomy (PTE).Prompt referral to a PTE center is critical.
Group 5 pulmonary hypertensionis multi factorial and can be from multiple etiologies including sarcoidosis, histiocytosis, and other hematological diseases such as chronic hemolytic anemia.
Physical Exam
A physical exam performed on patients with pulmonary hypertension may reveal a loud pulmonary second sound, right ventricular lift, and increased JVP.
Electrocardiogram
ECG may show right ventricular hypertrophy and‘P’ pulmonale in many cases.
Chest X-ray
The X-ray may show large pulmonary arteries and usually clear lungs particularly if the patient has type 1 pulmonary hypertension.
lmaging Procedures Available to Assess Pulmonary Hypertension
Imaging procedures include;
1.Echocardiographyto evaluate the left atrium, left ventricle, right ventricle, and tricuspid and mitral valves.The presence of an elevated right ventricular systolic pressure estimate and right ventricular dilation or systolic dysfunction may be a clue to the presence of pulmonary hypertension.Other supportive signs include an elevated ratio between right and left ventricular size (RV:LV ratio >1) or fl attening of the interventricular septum.Presence of signif i cant left ventricular systolic or diastolic dysfunction, left ventricular hypertrophy, left atrial
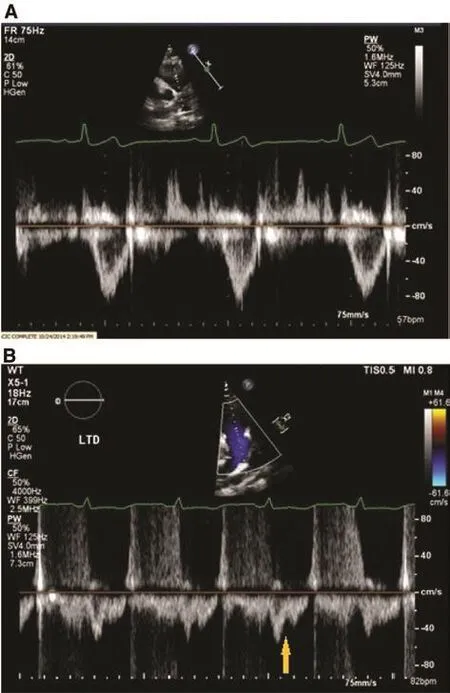
Figure 1 Pulsed Wave Doppler Patterns in the Right Ventricular Outf l ow Tract (RVOT).
2.Chest CTto assess for lung disease (Group 3) as a cause of pulmonary hypertension.
3.V/Q scanis done initially to search for the presence of CTEPH (Group 4).While it is possible to find chronic embolic disease on a CT angiogram,chronic thromboembolic disease often involves the peripheral pulmonary vasculature and may not be well visualized by CTA.
4.Pulmonary function testingto rule out chronic forms of lung disease such as COPD.Presence of PAH may be suspected by an isolated decrease in lung diffusion capacity for carbon monoxide(DLCO).
5.Right heart catheterizationis necessary to confirm the diagnosis of pulmonary hypertension and measure the pulmonary vascular resistance(
PVR) and pulmonary capillary wedge pressure.
Treat the Cause of the Pulmonary Hypertension
Pulmonary vasodilators such as phosphodiesterase inhibitors, endothelin receptor antagonists,and prostacyclin analogues should be reserved for Group 1 PAH patients i.e.those patients with increased pulmonary vascular resistance with normal PCWP.One exception would be patients with Group 4 CTEPH who are not candidates for PTE.These patients may be treated with the soluble guanylate cyclase stimulator, riociguat [5].Current guidelines do not support the use of pulmonary vasodilators in patients with pulmonary hypertension due to left sided heart disease [3].
Conclusion
Physicians should not consider pulmonary hypertension as a single entity.There are fi ve types of pulmonary hypertension.There are multiple imaging techniques to help define the type of pulmonary hypertension.Often, surgical as well as diagnostic procedures are aborted because of the possibility that all types of pulmonary hypertension increase the morbidity and mortality of whatever it is that is contemplated.There is no doubt that is the case in many instances, but it is not the same for every patient.For example if the patient has pulmonary hypertension because of elevation of the pulmonary artery pressure due to Left heart disease,pulmonary disease, Pulmonary emboli, type fi ve causes, then treating the pathologic cause is the therapy of choice and should be employed until stability is attained.
REFERENCES
1.Frost AE, Badesch DB, Barst RJ,Benza RL, Elliott CG, Farber HW, et al.The changing picture of patients with pulmonary arterial hypertension in the United States: how REVEAL differs from historic and non-US Contemporary Registries.Chest 2011;139(1):128–37.
2.Tonelli AR, Arelli V, Minai OA,Newman J, Bair N, Heresi GA,et al.Causes and circumstances of death in pulmonary arterial hypertension.Am J Respir Crit Care Med 2013;188(3):365–9.
3.Galiè N, Humbert M, Vachiery JL,Gibbs S, Lang I, Torbicki A, et al.2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: the Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology(ESC) and the European Respiratory Society (ERS): Endorsed by:Association for European Paediatric and Congenital Cardiology (AEPC),International Society for Heart and Lung Transplantation (ISHLT).Eur Respir J 2015;46(4):903–75.
4.Arkles JS, Opotowsky AR, Ojeda J, Rogers F, Liu T, Prassana V,et al.Shape of the right ventricular Doppler envelope predicts hemodynamics and right heart function in pulmonary hypertension.Am J Respir Crit Care Med 2011;183(2):268–76.
5.Ghofrani HA, D’Armini AM,Grimminger F, Hoeper MM, Jansa P, Kim NH, et al.Riociguat for the treatment of chronic thromboembolic pulmonary hypertension.N Engl J Med 2013;369(4):319–29.
杂志排行
Cardiovascular Innovations and Applications的其它文章
- Pulmonary Arterial Hypertension Medical Management of the Adult Patient with Congenital Heart Disease
- The Surgical Management of Ebstein Anomaly
- Evaluation of Left Ventricular Systolic Function after Pulmonary Valve Replacement Using Cardiovascular Magnetic Resonance lmaging
- Pregnancy in Congenital Heart Disease:A Review for the General Cardiologist
- Atrial Arrhythmias lncluding Atrial Fibrillation in Congenital Heart Disease: Mechanisms,Substrate ldentification and lnterventional Approaches
- Heart Transplantation for Adult Congenital Heart Disease: Overview and Special Considerations