Optic radiation injury in patients with aneurismal subarachnoid hemorrhage: a preliminary diffusion tensor imaging report
2018-04-04SungHoJangChulHoonChangYoungJinJungSeongHoKimJeongPyoSeo
Sung Ho Jang, Chul Hoon Chang, Young Jin Jung, Seong Ho Kim, Jeong Pyo Seo,
1 Department of Physical Medicine and Rehabilitation, College of Medicine, Yeungnam University, Namku, Daegu, Republic of Korea
2 Department of Neurosurgery, College of Medicine, Yeungnam University, Namku, Daegu, Republic of Korea
Introduction
Rupture of a cerebral artery aneurysm can lead to spontaneous subarachnoid hemorrhage (SAH). It is known to accompany various neurological sequelae, including visual impairment (Sarner and Rose, 1967; van Gijn et al., 2007; Schweizer et al., 2012;Rabinstein, 2013). Visual field defect, sequela of which have been reported in approximately 50% of patients with SAH, is one of the visual problems observed in patients with SAH (Tsementzis and Williams, 1984; Obuchowska et al., 2011). However, little is known about the pathogenic mechanism of visual field defect in SAH following rupture of a cerebral artery aneurysm.
Visual field defect is a typical clinical symptom of optic radiation (OR) injury (Mizrachi et al., 2005; Jang and Seo, 2015; Seo et al., 2015). A thorough examination in the aspects of safety and performance of activity of daily living for diagnosis of OR injury would be important for stroke patients (Gall et al., 2010). Conventional brain CT or brain MRI has mainly been used in the diagnosis of OR injury, however, it is limited because the OR cannot be distinguished from adjacent neural structures on these images(Kan and Matsubayashi, 1978; Zhang et al., 2006). In contrast,diffusion tensor imaging (DTI) allows three-dimensional reconstruction and evaluation of the OR (Werring et al., 1999; Berman et al., 2009; Hofer et al., 2010; Yeo et al., 2012a). Using DTI, a few studies have reported on OR injury in stroke patients (Yoshida et al., 2006; Polonara et al., 2011; Seo et al., 2013). However, there is no study reporting OR injury in patients with SAH. In the current study, we investigated the DTI finding of the OR in patients with SAH following rupture of a cerebral artery aneurysm.
Subjects and Methods
Subjects
Twenty-one patients with SAH (9 males, 12 females, mean age 53.43 years, range 40–68 years) and 21 age-matched normal control subjects with no history of neurologic or psychiatric diseases(12 males, 9 females, mean age, 52.67 years; range, 41–68 years)were recruited for this study. Among 148 patients with SAH admitted for rehabilitation in the Department of Rehabilitation of Yeungnam University Hospital, Republic of Korea, 21 consecutive patients were recruited according to the following inclusion criteria: 1) first ever stroke; 2) age: 21–69 years; 3) hemorrhage in the subarachnoid space due to aneurismal rupture revealed by brain CT (Figure 1); 4) DTI scanning was performed during the early stage (between three weeks and three months after onset);5) no intraventricular hemorrhage, intracerebral hemorrhage, or hydrocephalus; and 6) no de finite lesion along the visual pathway,including the OR on brain MRI (T1-weighted, T2-weighted, and fluid attenuated inversion recovery [FLAIR] images), con firmed by a neuroradiologist. The Institutional Review Board of Yeungnam University Hospital approved the study protocol (approval No. 2014-01-425), and this study was conducted retrospectively.
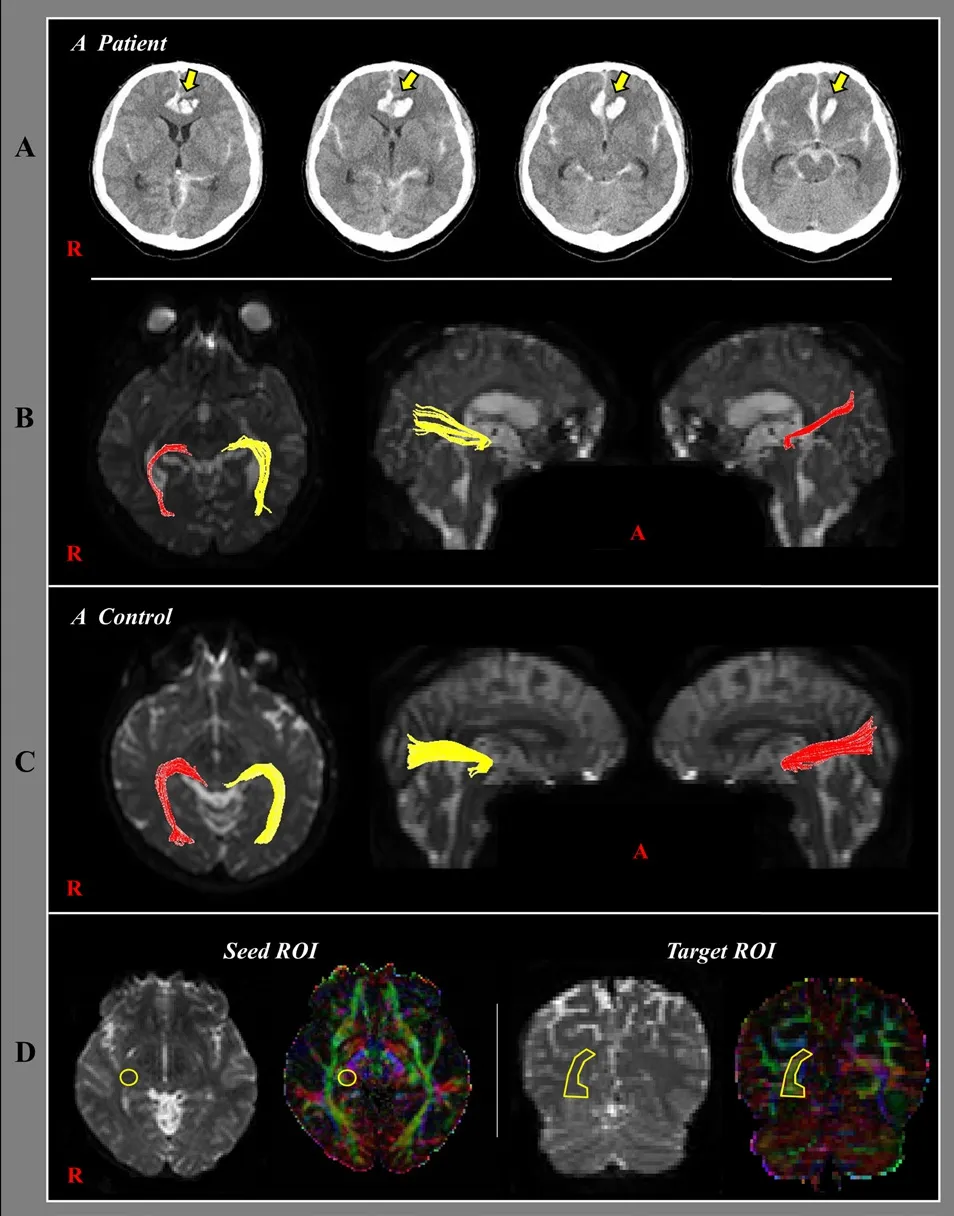
Figure 1 Brain CT images and diffusion tensor tractography images of patients with aneurismal SAH.
Table 1summarizes the demographic data from patients with aneurismal SAH and normal controls. Causes of SAH for 21 patients were as follows: the anterior communicating artery aneurysm rupture (n = 15, 71.4%), anterior cerebral artery aneurysm rupture (n = 3, 14.2%), posterior communicating artery aneurysm rupture (n = 1, 4.8%), middle cerebral artery aneurysm rupture (n= 1, 4.8%), and basilar artery aneurysm rupture (n = 1, 4.8%). The neurosurgical procedure for ruptured aneurysm was performed in 20 patients (aneurysm clipping in 17 patients and aneurysm coiling in 3 patients). Fisher CT grade was used to assess the severity of SAH (average grade: 2.9 ± 0.7) (Fisher et al., 1980).
Diffusion tensor imaging
Using a 1.5-T Philips Gyroscan Intera system (Philips, Ltd, Best,The Netherlands) equipped with a synergy-L Sensitivity Encoding (SENSE) head coil with a single-shot, spin-echo planar imaging pulse sequence, DTI data were acquired at an average of 5.9 weeks (range: 3–12 weeks) after onset. For each of the 32 non-collinear diffusion sensitizing gradients, we acquired 65 contiguous slices parallel to the anterior commissure-posterior commissure line. Imaging parameters were as follows: field of view = 221 × 221 mm2; repetition time = 10,726 ms; acquisition matrix = 96 × 96; echo time = 76 ms; number of excitations = 1;reconstruction matrix = 128 × 128 matrix; thickness = 2.3 mm;b = 1,000 s/mm2; and echo planar imaging factor = 67.
Eddy current-induced image distortions were removed using affine multi-scale two-dimensional registration at the Oxford Centre with the Functional Magnetic Resonance Imaging of the Brain (FMRIB) Software Library (FSL; www.fmrib.ox.ac.uk/fsl)(Smith et al., 2004). DTI-Studio software (CMRM, Johns Hopkins Medical Institute, Baltimore, MD, USA) was used for evaluation of the OR (Jiang et al., 2006). For reconstruction of the OR, a seed region of interest (ROI) was drawn manually on the lateral geniculate body on the color map, and a target ROI was placed in the middle of the OR bundle between the lateral geniculate body and occipital pole with the option of a CUT operation (Glass et al.,2010; Hofer et al., 2010; Seo et al., 2013). The CUT operation was used for reconstruction of the OR between the seed and target ROIs by eliminating other redundant fiber trajectories (fractional anisotropy (FA) threshold of > 0.2 and direction threshold < 60°)(Xie et al., 2007; Seo et al., 2013). The FA (the degree of directionality of microstructures) value, apparent diffusion coefficient (the magnitude of water diffusion, ADC) value, and fiber number (the neural fiber number of a neural tract) of the OR were measured in both hemispheres using DTI-Studio software (Laboratory of Brain Anatomical MRI, Johns Hopkins Medical Institute).
Table 1 Demographic data of patients with aneurismal SAH and normal control subjects
Statistical analysis
Statistical analysis was performed using SPSS 17.0 for Windows(SPSS Inc., Chicago, IL, USA). Data are expressed as the mean ±SD. The FA value, ADC value, and fiber number of the OR were compared between patients and normal controls, and between the left and right hemispheres using independent samples t-test.A level of P < 0.05 was considered statistically signi ficant.
Results
The ORs were reconstructed in 84 hemispheres of 42 whole subjects (100%). The DTI findings of patients with aneurismal SAH and normal controls are shown inTable 2andFigure 2.The FA value of the OR was significantly decreased, and the ADC value was signi ficantly increased, in patients with aneurismal SAH compared with those in the normal control subjects(both P < 0.05). However, there was no signi ficant difference in the fiber number of the OR between patients with aneurismal SAH and normal control subjects (P > 0.05). No difference in any of DTI parameters (FA, ADC and fiber number) of the OR was observed between the left and right hemispheres in patients with aneurismal SAH or normal control subjects (P > 0.05).
Discussion
In the current study, we recruited patients with aneurismal SAH who did not show any specific lesion in the visual pathway, including the OR, on brain MRI, and adopted three DTI parameters (the FA, ADC, and fiber number) to assess the state of the OR. FA value was signi ficantly decreased and ADC value was significantly increased in patients with aneurismal SAH than in normal control subjects. But there was no significant difference in the fiber number of the OP between patients with aneurismal SAH and normal control subjects. FA value indicates the degree of directionality of water diffusion and reflects the integrity of white matter microstructures, such as axon, myelin,and microtubule (Assaf and Pasternak, 2008; Neil, 2008). ADC value represents the magnitude of water diffusion (Assaf and Pasternak, 2008; Neil, 2008; Jang and Jang, 2016). Fiber number indicates the total number of neural fibers in a neural tract (Jang and Jang, 2016). The decrement of FA value and increment of ADC value of the OR in patients with aneurismal SAH suggest OR injury. Many studies have reported on visual impairment in patients with SAH (Tsementzis and Williams, 1984; Chan et al.,1997; Hara et al., 2003; Obuchowska et al., 2010, 2011; Walkden and Brennan, 2012). Most of these studies focused on visual problems caused by lesions in the visual pathway, except for the OR, such as the eye, optic nerve, or optic chiasm (Tsementzis and Williams, 1984; Chan et al., 1997; Hara et al., 2003; Obuchowska et al., 2010; Walkden and Brennan, 2012). To the best of our knowledge, only a few studies have reported results that appeared to be related to injury of the OR (Liu et al., 2007; Obuchowska et al., 2011). In 2007, Liu et al. reported that the ADC value in normal appearing white matter in the occipital lobe, as well as the whole cerebral lobe, except for the frontal lobe, was increased in patients with aneurismal SAH in the subacute stage. In 2011,Obuchowska et al. reported detection of visual field defects in 50% of 23 patients with SAH who were treated with aneurismal clipping. The relatively frequent types of visual field defects include constricted field (47.8%), multiple peripheral foci (26.1%),and superior field defect (17.4%). They suggested that the pattern of these abnormalities corresponds to damage to the anterior segment of the visual pathways such as optic nerve or optic chiasm.However, in this study, we found differences in DTI parameters consistent with OR injury located in the posterior portion of the visual pathway in patients with aneurismal SAH.
The pathogenic mechanism of neural injury in SAH has not been elucidated. There are few studies on this topic (Liu et al.,2007; Yeo et al., 2012b). In 2007, Liu et al. reported that SAH may cause global mild vasogenic edema in white matter and deep gray matter, but was detected by measuring the ADC value in the subacute stage of SAH. Therefore, this result indicates that SAH can cause injury to white matter, which is located far from the subarachnoid space. In 2012, Yeo et al. demonstrated injury of the corticospinal tract at the midbrain in patients with SAH (Yeo et al., 2012b). They suggested that injury of the corticospinal tract at the midbrain occurred through chemical(a blood clot itself can cause extensive damage) or mechanical mechanisms (increased intracranial pressure or direct mass)(van Gijn et al., 1985; Chua et al., 2009). Considering the results of the previous studies, we can assume that SAH may cause injury to the OR, which is located far from the arachnoid space, as well as near to the arachnoid space in the occipital lobe. Further studies are required to analyze the according to the distance from the arachnoid space. In addition, DTI studies addressing follow up from acute stage to chronic state should be performed to clarify the pathogenic mechanism.
In conclusion, using DTI, we investigated the OR state in aneurismal SAH. Results from this study demonstrated that the values of FA and ADC parameters were consistent with OR injury. Therefore, we recommend a thorough examination to evaluate OR injury in patients with aneurismal SAH. To the best of our knowledge, this is the first DTI study addressing OR injury in patients with aneurismal SAH. However, limitations of this study should be considered. First, DTI analysis is operator dependent and it may cause false negative or false positive results for the fiber tracks due to fiber complexity or crossing fiber effect (Yamada, 2009). Second, the lack of clinical dataregarding ocular or OR injury, such as visual field study, which could not be included because we conducted this study retrospectively. Third, we recruited a small number of patients from patients with SAH who had been admitted for rehabilitation.Therefore, there is a possibility that among all patients with SAH, we recruited patients with severe clinical manifestations.Further prospective studies involving larger numbers of patients and including clinical evaluations of OR injury should be performed. In addition, in-depth DTI studies on the anterior visual pathway such as optic nerve, optic chiasm, and optic tract should also be encouraged.

Table 2 Data on diffusion tensor imaging parameters of the optic radiation in patients with aneurismal SAH and normal control subjects
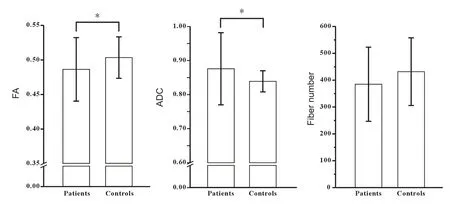
Figure 2 Comparison of diffusion tensor imaging parameters between patients with aneurismal subarachnoid hemorrhage and normal controls.
Author contributions:SHJ conceived and designed the study, was responsible for fundraising, data acquisition, manuscript development and writing. CHC,YJJ, SHK and JPS were in charge of data acquisition. JPS contributed to paper development, writing and authorization. All authors approved the final version of this paper.
Con flicts of interest:None declared.
Financial support:This work was supported by the National Research Foundation (NRF) of Korea Grant funded by the Korean Government (MSIP)(2015R1A2A2A01004073).
Research ethics:The study was approved by the institutional review board of Yeungnam University Hospital (approval No. 2014-01-425). The study followed the Declaration of Helsinki and relevant ethical principles.
Declaration of participant consent:The authors certify that they have obtained all appropriate participant consent form. In the form, participants have given their consent for their images and other clinical information to be reported in the journal. The participants understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Data sharing statement:Datasets analyzed during the current study are available from the corresponding author on reasonable request.
Plagiarism check:Checked twice by iThenticate.
Peer review:Externally peer reviewed.
Open access statement:This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under identical terms.
Assaf Y, Pasternak O (2008) Diffusion tensor imaging (DTI)-based white matter mapping in brain research: a review. J Mol Neurosci 34:51-61.
Berman JI, Glass HC, Miller SP, Mukherjee P, Ferriero DM, Barkovich AJ,Vigneron DB, Henry RG (2009) Quantitative fiber tracking analysis of the optic radiation correlated with visual performance in premature newborns. AJNR Am J Neuroradiol 30:120-124.
Chan JW, Hoyt WF, Ellis WG, Gress D (1997) Pathogenesis of acute monocular blindness from leaking anterior communicating artery aneurysms:report of six cases. Neurology 48:680-683.
Chua CO, Chahboune H, Braun A, Dummula K, Chua CE, Yu J, Ungvari Z,Sherbany AA, Hyder F, Ballabh P (2009) Consequences of intraventricular hemorrhage in a rabbit pup model. Stroke 40:3369-3377.
Fisher CM, Kistler JP, Davis JM (1980) Relation of cerebral vasospasm to subarachnoid hemorrhage visualized by computerized tomographic scanning. Neurosurgery 6:1-9.
Gall C, Franke GH, Sabel BA (2010) Vision-related quality of life in first stroke patients with homonymous visual field defects. Health Qual Life Outcomes 8:33.
Glass HC, Berman JI, Norcia AM, Rogers EE, Henry RG, Hou C, Barkovich AJ, Good WV (2010) Quantitative fiber tracking of the optic radiation is correlated with visual-evoked potential amplitude in preterm infants.AJNR Am J Neuroradiol 31:1424-1429.
Hara N, Mukuno K, Ohtaka H, Shimizu K (2003) Ischemic optic neuropathy associated with subarachnoid hemorrhage after rupture of anterior communicating artery aneurysm. Ophthalmologica 217:79-84.
Hofer S, Karaus A, Frahm J (2010) Reconstruction and dissection of the entire human visual pathway using diffusion tensor MRI. Front Neuroanat 4:15.
Jang SH, Seo JP (2015) Damage to the optic radiation in patients with mild traumatic brain injury. J Neuroophthalmol 35:270-273.
Jang SH, Jang WH (2016) Change of the corticospinal tract in the unaffected hemisphere by change of the dominant hand following stroke: a cohort study. Medicine (Baltimore) 95:e2620.
Jiang H, van Zijl PC, Kim J, Pearlson GD, Mori S (2006) DtiStudio: resource program for diffusion tensor computation and fiber bundle tracking.Comput Methods Programs Biomed 81:106-116.
Kan S, Matsubayashi T (1978) CT in homonymous hemianopia. Neuroradiology 16:299-301.
Liu Y, Soppi V, Mustonen T, Kononen M, Koivisto T, Koskela A, Rinne J,Vanninen RL (2007) Subarachnoid hemorrhage in the subacute stage:elevated apparent diffusion coefficient in normal-appearing brain tissue after treatment. Radiology 242:518-525.
Mizrachi IB, Schmaier AH, Trobe JD (2005) Homonymous hemianopia caused by occipital lobe infarction in heparin-induced thrombocytopenia and thrombosis syndrome. J Neuroophthalmol 25:193-197.
Neil JJ (2008) Diffusion imaging concepts for clinicians. J Magn Reson Imaging 27:1-7.
Obuchowska I, Kochanowicz J, Mariak Z (2010) Early changes in the visual system connected with brain’s aneurysm rupture. Klin Oczna 112:120-123.
Obuchowska I, Turek G, Mariak Z, Kochanowicz J (2011) Late ophthalmological assessment of patients with subarachnoid hemorrhage and clipping of cerebral aneurysm. Acta Neurochir (Wien) 153:2127-2136.
Polonara G, Salvolini S, Fabri M, Mascioli G, Cavola GL, Neri P, Mariotti C,Giovannini A, Salvolini U (2011) Unilateral visual loss due to ischaemic injury in the right calcarine region: a functional magnetic resonance imaging and diffusion tension imaging follow-up study. Int Ophthalmol 31:129-134.
Rabinstein AA (2013) Subarachnoid hemorrhage. Neurology 80:e56-59.
Sarner M, Rose FC (1967) Clinical presentation of ruptured intracranial aneurysm. J Neurol Neurosurg Psychiatry 30:67-70.
Schweizer TA, Al-Khindi T, Loch Macdonald R (2012) Diffusion tensor imaging as a surrogate marker for outcome after perimesencephalic subarachnoid hemorrhage. Clin Neurol Neurosurg 114:798-800.
Seo JP, Choi BY, Chang CH, Jung YJ, Byun WM, Kim SH, Kwon YH, Jang SH (2013) Diffusion tensor imaging findings of optic radiation in patients with putaminal hemorrhage. Eur Neurol 69:236-241.
Seo YS, Kim SH, Jang SH (2015) Bilateral homonymous quadrantanopsia due to optic radiation injury in a patient with traumatic brain injury. Am J Phys Med Rehabil 94:e116.
Smith SM, Jenkinson M, Woolrich MW, Beckmann CF, Behrens TE, Johansen-Berg H, Bannister PR, De Luca M, Drobnjak I, Flitney DE, Niazy RK, Saunders J, Vickers J, Zhang Y, De Stefano N, Brady JM, Matthews PM (2004) Advances in functional and structural MR image analysis and implementation as FSL. Neuroimage 23 Suppl 1:S208-219.
Tsementzis SA, Williams A (1984) Ophthalmological signs and prognosis in patients with a subarachnoid haemorrhage. Neurochirurgia (Stuttg)27:133-135.
van Gijn J, Kerr RS, Rinkel GJ (2007) Subarachnoid haemorrhage. Lancet 369:306-318.
van Gijn J, van Dongen KJ, Vermeulen M, Hijdra A (1985) Perimesencephalic hemorrhage: a nonaneurysmal and benign form of subarachnoid hemorrhage. Neurology 35:493-497.
Walkden A, Brennan P (2012) Sudden onset loss of vision following subarachnoid haemorrhage. BMJ Case Rep 2012.
Werring DJ, Clark CA, Parker GJ, Miller DH, Thompson AJ, Barker GJ(1999) A direct demonstration of both structure and function in the visual system: combining diffusion tensor imaging with functional magnetic resonance imaging. Neuroimage 9:352-361.
Xie S, Gong GL, Xiao JX, Ye JT, Liu HH, Gan XL, Jiang ZT, Jiang XX (2007)Underdevelopment of optic radiation in children with amblyopia: a tractography study. Am J Ophthalmol 143:642-646.
Yamada K (2009) Diffusion tensor tractography should be used with caution. Proc Natl Acad Sci U S A 106:E14; author reply E15.
Yeo SS, Kim SH, Kim OL, Kim MS, Jang SH (2012a) Optic radiation injury in a patient with traumatic brain injury. Brain Inj 26:891-895.
Yeo SS, Choi BY, Chang CH, Kim SH, Jung YJ, Jang SH (2012b) Evidence of corticospinal tract injury at midbrain in patients with subarachnoid hemorrhage. Stroke 43:2239-2241.
Yoshida M, Ida M, Nguyen TH, Iba-Zizen MT, Bellinger L, Stievenart JL,Nagao T, Kikuchi S, Hara T, Shiba T, Kitahara K, Cabanis EA (2006) Resolution of homonymous visual field loss documented with functional magnetic resonance and diffusion tensor imaging. J Neuroophthalmol 26:11-17.
Zhang X, Kedar S, Lynn MJ, Newman NJ, Biousse V (2006) Homonymous hemianopia in stroke. J Neuroophthalmol 26:180-183.
杂志排行

中国神经再生研究(英文版)的其它文章
- The biological clock: future of neurological disorders therapy
- Cerebral ischemia and neuroregeneration
- SNARE complex in axonal guidance and neuroregeneration
- Heterozygous carriers of galactocerebrosidase mutations that cause Krabbe disease have impaired microglial function and defective repair of myelin damage
- The relaxin peptide family – potential future hope for neuroprotective therapy? A short review
- Roles of neural regeneration in memory pharmacology