Pleasure Experience and Emotion Expression in Patients with Schizophrenia
2017-11-29MinyiCHUXuLIQinyuLVZhenghuiYIEricCHEUNGRaymondCHAN
Min-yi CHU, Xu LI, Qin-yu LV, Zheng-hui YI, Eric F. C. CHEUNG, Raymond C. K. CHAN,2,6*
•ORIGINAL RESEARCH ARTICLE•
Pleasure Experience and Emotion Expression in Patients with Schizophrenia
Min-yi CHU1, Xu LI2,3, Qin-yu LV4, Zheng-hui YI4, Eric F. C. CHEUNG5, Raymond C. K. CHAN1,2,6*
Emotional experience; Emotional expression; Schizophrenia
1. Introduction
It has been increasingly recognized that schizophrenia is associated with impairment in pleasure experience.[1-3]Patients with schizophrenia may be impaired in both pleasure experience and emotion expression, which may cause significant disability.[4]Although negative symptoms and affective flattening are considered core features of schizophrenia, there exists significant heterogeneity in symptom presentation in patients with schizophrenia.
Experience of pleasure could be divided into anticipatory pleasure and consummatory pleasure.[5,6]Anticipatory pleasure is linked with motivation and goal-directed behaviour, while consummatory pleasure is related to in-the-moment experience. Many studies have shown that patients with schizophrenia are impaired in anticipatory pleasure, especially abstract anticipatory pleasure, but relatively intact in consummatory pleasure experience.[7,8]However, Straus et al reported an opposite pattern in which patients with schizophrenia differed from healthy controls in consummatory pleasure but not anticipatory pleasure.[9]Gooding et al reported that individuals with high levels of social anhedonia are impaired in both anticipatory and consummatory pleasure.[10]Based on the two-factor model of the Temporal Experience of Pleasure Scale(TEPS), Chan reported a four-factor Chinese version of the TEPS that comprised abstract and contextual domains under anticipatory and consummatory pleasure.[11]Li et al further replicated this four-factor model of the TEPS in patients in different stages of schizophrenia in the Chinese setting.[12]They also found that patients with first episode and chronic schizophrenia and people with schizotypal features reported lower levels of abstract anticipatory pleasure,but not all of them reported lower levels of contextual anticipatory pleasure compared with healthy controls.
Patients with schizophrenia may not only be impaired in pleasure experience, but also in expressing emotion. A general impairment in emotion expression has been reported in schizophrenia patients.[13]Previous studies have shown that patients with schizophrenia are unable to recognize and describe their feelings(alexithymia), are less expressive (both facially and vocally) than individuals without this disorder,[14]and have diminished ability to outwardly express emotion.[15]Shi et al showed that individuals with negative schizotypal personality disorder features exhibited deficits in self-reported emotion expression, but little is known about patients with schizophrenia.[16]
Previous studies have shown that emotion impairment is correlated with clinical symptoms.[7,17]Negative symptoms are a core feature of schizophrenia.[18]Kring and Brach conceptualized the structure of negative symptoms as a two-factor model, namely diminished motivation and pleasure (anhedonia) and diminished verbal and non-verbal expression and communication(flat affect and poor speech).[4]Anhedonia represents a deficit in the "experience" of emotion, and flat affect reflects a deficit in the "expression" of emotion.[19]Some attempts have been made to examine the correlations between emotion impairments and negative symptoms. Kohler et al demonstrated that emotion recognition deficits were significantly correlated with alogia.[20]Schneider et al suggested that different aspects of emotional behaviour were impaired in subtypes of schizophrenia, and it may be meaningful to compare emotional deficits in different subgroups of patients with schizophrenia.[21]
In this study, we examined pleasure experience and emotion expression in patients with schizophrenia.In particular, we categorized patients with schizophrenia into those with prominent negative symptoms and those without using a set of wellrecognized pre-defined criteria to examine the relationship between emotion impairments (both pleasure experience and expression) and negative symptoms. We hypothesized that patients with schizophrenia would exhibit impaired anticipatory pleasure experience and reduced emotion expression,but relatively intact consummatory pleasure experience.We further hypothesized that schizophrenia patients with prominent negative symptoms would exhibit more severe deficits in abstract pleasure experience than those without prominent negative symptoms.
2. Methods
2.1. Participants
One hundred and fifty in-patients with schizophrenia fulfilling DSM-IV criteria[22]were recruited from the Beijing Huilongguan Hospital and the Shanghai Mental Health Center. Exclusion criteria included a history of (1) substance abuse or other mental disorders; (2)electroconvulsive therapy in the past three months;(3) neurological disorder; (4) head injury with loss of consciousness for more than 30 minutes; and (5)other major organ disorders. All participants were assessed by qualified psychiatrists using structural interviews to ensure the absence of any Axis I DSMIV psychiatric disorders. The average duration of illness of the participants was 5.80 years (SD=5.09 years, median=4.79 years, Quartile interval: 2.00 years-8.75 years) and the mean antipsychotic dosage in chlorpromazine equivalence was 299.83mg/day (SD=193.73mg/day, median=250.00mg/day,Quartile interval: 150mg/day-400mg/day). Participants'intelligence was estimated using a prorating method based on the Arithmetic, Similarities and Digit span subscales of the Chinese version of the Wechsler Adult Intelligence Scale-Revised.[23]
We categorized the participants into those with and without prominent negative symptoms based on scores of the Positive and Negative Syndrome Scale[24]according to the following criteria that have been established in previous studies[25]: (1) Baseline score > 4(moderate) on at least three, or > 5 (moderately severe)on at least two negative PANSS subscale items[26,27];or (2) PANSS negative subscale score > 3 on item 1(blunted affect) and at least one third of the items had a score of > 3 and a maximum of two items with a score > 3 on the positive subscale.[28]Based on these criteria, a total of 17 patients were classified as having prominent negative symptoms, while 133 patients were classified as without prominent negative symptoms.There were no differences in the estimated intelligence quotient (IQ) (t(19)=1.37, p=0.19) and antipsychotic dosage (t(16)=0.58, p=0.57) between the two groups,but patients with prominent negative symptoms had a shorter duration of illness than patients without prominent negative symptoms (t(28)=2.67, p=0.01).
We also recruited 105 healthy individuals from the community who were matched with the patients by gender, years of education and age as controls. None of them had any lifetime or family history of psychosis,or a history of substance abuse or neurological disorders. The present study was approved by the Ethics Committees of the Institute of Psychology, the Beijing Huilongguan Hospital and the Shanghai Mental Health Center. Informed consent was obtained from all participants.
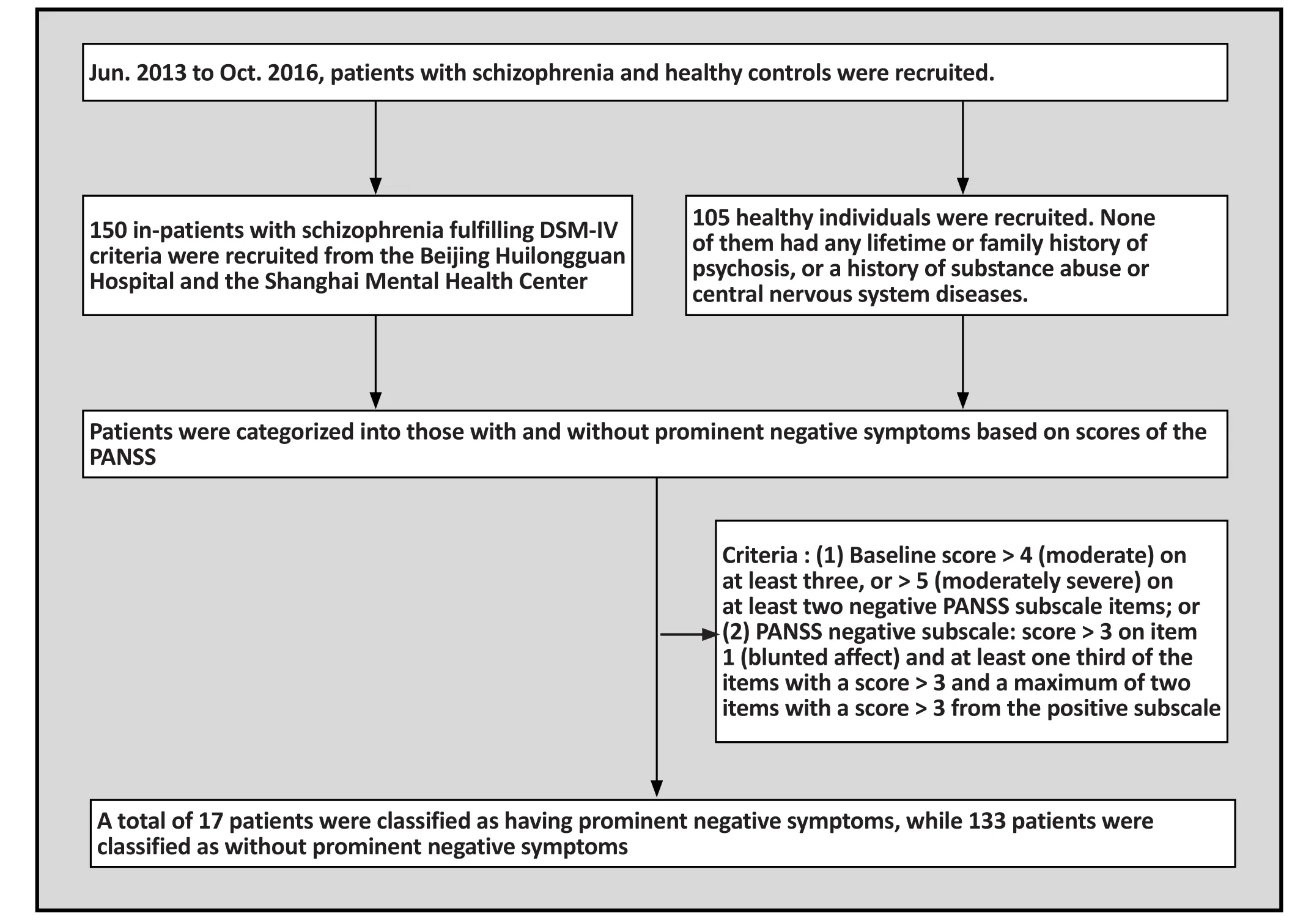
Figure 1. Flowchart of the study
2.2. Measures
2.2.1. Positive and Negative Syndrome Scale (PANSS)
Positive and Negative Syndrome Scale (PANSS)measures the positive, negative and general syndrome in schizophrenia.[24]The interview-based scale contains 30 items, and each item is scored on a seven-point Likert scale, ranging from 1 ("absent") to 7 ("extreme").The PANSS positive subscale includes seven items (e.g.delusions; conceptual disorganization); the negative subscale contains seven items (e.g. blunted affect;emotional withdrawal); and the general psychopathology subscale includes 16 items (e.g. somatic concern; anxiety).The positive, negative and general psychopathology subscales possess high internal consistency (Cronbach's alpha coefficients: 0.73, 0.78 and 0.79).
2.2.2. Temporal Experience of Pleasure Scale (TEPS)
The TEPS consists of 18 items, with a six-point Likert scale, ranging from "very false for me" to "very true for me".[29]It comprises 10 items for anticipatory pleasure and eight items for consummatory pleasure.The overall scale and subscales show good internal consistency (Cronbach's alphas: 0.79, 0.74, and 0.71 for the total score, the anticipatory subscale score and the consummatory subscale score, respectively).The Chinese version of the TEPS used in this study extended the two-factor structure into a four-factor model, consisting of 20 items.[11]The four-factor model includes abstract anticipatory pleasure, contextual anticipatory pleasure, abstract consummatory pleasure and contextual consummatory pleasure. The abstract items refer to stating something abstract or conceptual such as "Looking forward to a pleasurable experience is in itself pleasurable", while the contextual items refer to concrete and tangible events such like "When I hear about a new movie starring my favourite actor, I can't wait to see it". Good internal consistency of this Chinese version (Cronbach alphas ranging from 0.63 to 0.83) have been demonstrated in the Chinese setting.
2.2.3. Emotional Expressivity Scale (EES)
Emotional Expressivity Scale (EES) is a 17-item Likert self-reported questionnaire with a possible rating from 1 (never true) to 6 (always true).[30]It assesses individual differences in emotional expressivity and had high internal consistency and test-retest reliability. Chan et al reported a two-factor structure of the EES in the Chinese setting, namely the Expression Subscale (e.g.I can't hide the way I am feeling) and the Suppression Subscale (e.g. I keep my feelings to myself).[31]The Chinese version has been shown to have good internal consistency (Cronbach's alpha = 0.816 for the total score, 0.84 and 0.778 for the Expression and Suppression Subscale scores, respectively).
2.3. Data analysis
We used independent-samples t test to compare the TEPS and the EES scores of patients and healthy controls. One-way ANOVAs were conducted to assess group differences between patients with and without prominent negative symptoms and healthy individuals.Post-hoc analysis was conducted using the Least Square Differences (LSD) test.
3. Results
3.1. Demographics
Table 1 shows the demographic information of the patients with schizophrenia and healthy controls. There were no significant differences in gender (c2=0.76,p=0.38), years of education (t(253)=-1.38, p=0.17) and age (t(227)=0.35, p=0.73) between the two groups.However, patients with schizophrenia had significantly lower IQ estimates than healthy controls.
3.2. Comparison of TEPS and EES scores between schizophrenia patients and healthy controls
Patients with schizophrenia experienced less pleasure than healthy controls in the following domains:abstract anticipatory pleasure (t(243)=-3.86, p<0.001,Cohen's d=0.49), abstract consummatory pleasure(t(250)=-2.58, p=0.010, Cohen's d=0.32), contextual consummatory pleasure (t(248)=-3.56, p=0.001,Cohen's d=0.45), overall consummatory pleasure(t(176)=-2.91, p=0.002, Cohen's d=0.31) and TEPStotal (t(247)=-2.45, p=0.015 Cohen's d=0.38).There were no significant differences in expression of emotion between the two groups (see Table 1). In addition, in the multivariate analysis of gender and group (patient group, control group), the main effect of gender was significant, but the main effect of group and the interaction effect were not significant.
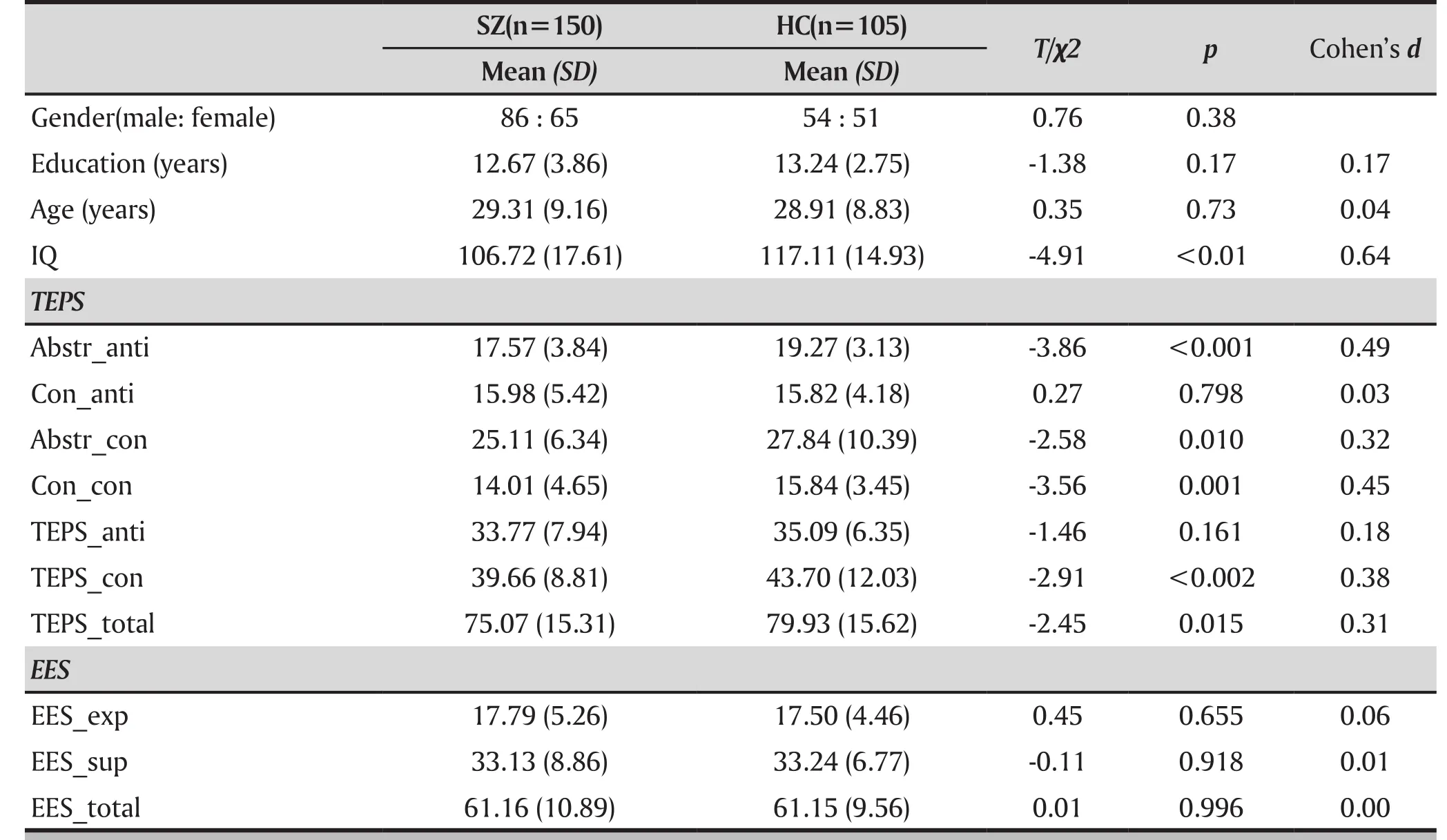
Table 1. Comparison of experiential pleasure and emotion expression between patients with schizophrenia and controls
3.3. Difference in performance on the TEPS and the EES between patients with and without prominent negative symptoms and controls
Table 2 and Figure 2 summarize the TEPS and EES scores between patients with and without prominent negative symptoms and healthy controls. The post-test of ANOVA showed that patients without prominentnegative symptoms reported experiencing significantly less abstract anticipatory pleasure (p=0.001, Cohen's d=0.44), less abstract consummatory pleasure (p=0.017,Cohen's d=0.31), less contextual consummatory pleasure(p=0.005, Cohen's d=0.38), and had a lower total score on the TEPS consummatory pleasure factor (p=0.008,Cohen's d=0.35) than healthy individuals. Patients with prominent negative symptoms had lower scores than healthy controls in the following domains: abstract anticipatory pleasure (p<0.001, Cohen's d=1.12),abstract consummatory pleasure (p=0.037, Cohen's d=0.57), contextual consummatory pleasure (p=0.008,Cohen's d=0.81), TEPS anticipatory pleasure (p=0.016,Cohen's d=0.73), and TEPS consummatory pleasure(p=0.005, Cohen's d=0.74). Compared with patients without prominent negative symptoms, patients with prominent negative symptoms had relatively lower scores on both the TEPS and the EES except for the EES total score. However, there was no significant difference between the three groups in overall EES scores.
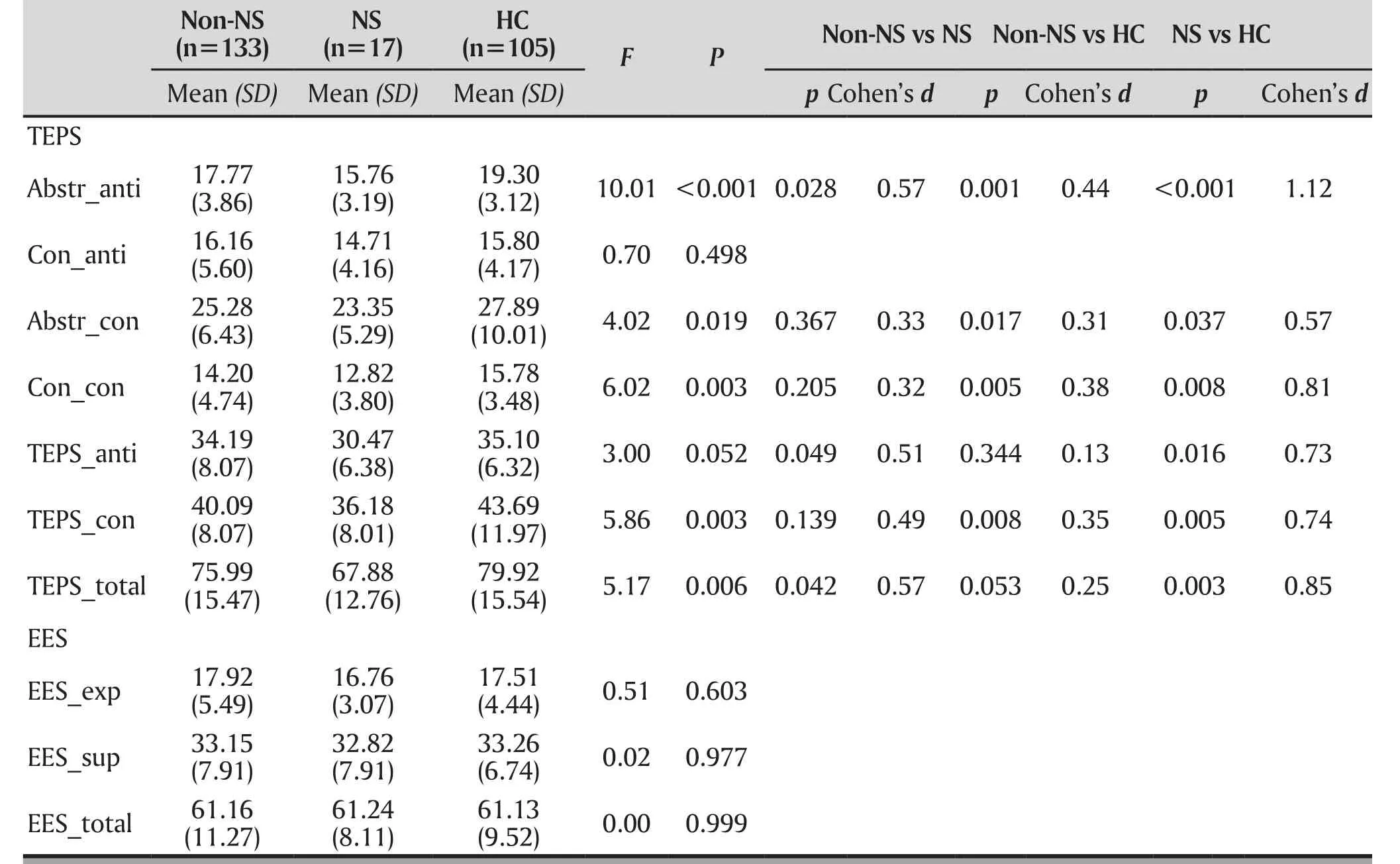
Table 2. Comparisons of experiential pleasure and emotion expression between patients with and without prominent negative symptoms, and controls.
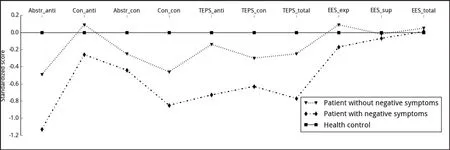
Figure 2. Experience of pleasure and expression of healthy controls and schizophrenia patients with prominent negative symptoms, schizophrenia patients without prominent negative symptoms
4. Discussion
4.1 Main findings
Our findings showed that patients with schizophrenia experienced less abstract anticipatory pleasure but not contextual anticipatory pleasure than healthy controls.This is consistent with results from Li et al.'s study,which showed that both patients with first-episode and chronic schizophrenia had deficits in abstract but not contextual anticipatory pleasure.[12]Patients with schizophrenia had difficulties in responding to the abstract anticipatory pleasure items of the TEPS,suggesting that they may have difficulty in envisioning abstract events. Contrary to our hypothesis,schizophrenia patients also exhibited deficits in consummatory pleasure, both in the abstract and contextual domains. Although most studies showed that patients were impaired in anticipatory pleasure and relatively intact in consummatory pleasure, some studies have also reported similar findings with our present results that patients were impaired in both anticipatory and consummatory pleasure experience.[10,32,33]A meta-analysis found that patients may be abnormal in regions of the brain related with consummatory pleasure.[34]However, some researchers have reported that schizophrenia patients showed less severe deficits in pleasure experience in laboratory conditions when presented with evocative stimuli directly.[35,36]An explanation of the difference is that self-reported scales(e.g. TEPS) require more cognitive engagement. Since schizophrenia patients are often cognitively impaired,they may exhibit more severe impairment in pleasure experience when assessed using self-reported scales.Moreover, it has been suggested that self-reported measures such as the TEPS are designed to capture only hypothetical situations rather than "factual situations".[37]The fact that the TEPS may not be able to measure consummatory pleasure in "hypothetical situations" may explain why our findings were different from the original anticipatory-consummatory differential deficit reported by Gard et al.[29]
We found that schizophrenia patients with prominent negative symptoms showed more deficits in anticipatory pleasure, especially in abstract anticipatory pleasure.Some previous studies have reported similar findings in patients with prominent negative symptoms or individuals with negative schizotypal personality features.[16]Patients with prominent negative symptoms may be less motivated to anticipate pleasant events, resulting in reduced pleasure when anticipating those events.One explanation may be that patients with negative symptoms are impaired in memory,[38]which leads to difficulty in processing and integrating the pleasure they experience in the moment. Hence, they may be less motivated to seek pleasure in the future (anticipatory pleasure). In addition, a previous study has reported that un-medicated schizophrenia patients and patients taking conventional antipsychotics showed reduced activation in the ventral striatum in response to reward anticipation,[39]which was significantly associated with negative symptoms. It is interesting to note that our findings also demonstrated that the deficits in anticipatory pleasure were only present in the abstract facet but not in the contextual facet. This finding is consistent with Li's findings that abstract anticipatory pleasure is impaired across all stages of the schizophrenia spectrum.[12]
Our findings in emotion expression were contrary to our expectation. There were no significant differences between schizophrenia patients and healthy controls in emotion expression, even after categorizing schizophrenia patients into those with and without prominent negative symptoms. There may be several possible explanations. First, it is commonly acknowledged that there is an "emotional paradox" in schizophrenia patients.[40]Emotional impairments may be mainly reflected in pleasure experience deficits instead of emotion expression in this clinical group. Secondly,previous studies have suggested that there may be gender differences in emotion expression, with women tending to be more emotionally expressive than men.[4,41,42]Since female patients made up nearly half of our sample, we speculated that the difference in emotion expression between genders might have attenuated the difference in the present study. However, such a speculation needs to be confirmed in future studies. Alternatively, people with schizophrenia may not be aware of their reduction in emotion expression even when these impairments in expression exist, which may not be captured using self-report scales such as the EES. Future studies should include objective measures to assess emotion expression in patients with schizophrenia.
4.2 Limitations
This study has several limitations. First, we only used self-reported scales to measure emotion experience and expression, which are relatively subjective and rely mainly on the participants' ability to recall particular experiences. Future studies should consider adopting additional objective measures such as computer-based tasks or measures to capture facial expression and speech production. Secondly, we recruited schizophrenia patients from two different areas: Beijing and Shanghai, and the assessments of clinical symptoms were completed by different clinicians. Although they were all experienced clinicians, there might have been inter-observer variation in the ratings. Thirdly, the sample of schizophrenia patients with prominent negative symptoms was small.Future studies should use a larger sample size of patients with prominent negative symptoms.
4.3 Implications
In this study, we explored the pleasure experience and emotional expression in patients with schizophrenia,especially in patients with and without prominent negative symptoms. The present findings suggest that patients with schizophrenia have deficits in pleasure experience, while their abilities to express emotion appear intact. Such deficits, in particular in abstract anticipatory pleasure, are more severe in patients with prominent negative symptoms. This could be helpful in investigating the relationship between negative symptoms and pleasure deficits in schizophrenia.
Funding statement
This study was supported in part by the National Science Fund China (81571317), the Science Foundation of Shanghai Mental Health Center (SMHCRSD01), the Beijing Training Project for the Leading Talents in S &T (Z151100000315020), and a grant from the Beijing Municipal Science & Technology Commission Grant(Z161100000216138). The authors would also like to thank the participants of the present study.
Conflicts of interest statement
The authors declare no conflict of interest related to this study
Ethical approval
The present study was approved by the Ethics Committees of the Institute of Psychology, the Beijing Huilongguan Hospital and the Shanghai Mental Health Center.
Informed consent
Informed consent was obtained from all participating patients.
Authors' contributions
Min-yi Chu was responsible for the study design,analyzed and wrote the article.
Raymond C. K. Chan generated the idea and governed the study, and commented significantly on the article
Xu li, Qin-yu Lv, Zheng-hui Yi were responsible for clinical diagnosis and rating of patients with schizophrenia
Eric F. C. Cheung commented significantly on the article
1. Berenbaum H, Oltmanns TF. Emotional experience and expression in schizophrenia and depression. J Abnorm Psychol. 1992; 101(1): 37
2. Fabien T. A review of emotion deficits in schizophrenia.Dialogues Clin Neurosci. 2006; 8(1): 59-70. doi: https://doi.org/10.1016/s0165-0173(98)00019-8
3. Kring AM, Elis O. Emotion deficits of in people with schizophrenia. Annu Rev Clin Psychol. 2013; 9: 409-433. doi:https://doi.org/10.1146/annurev-clinpsy-050212-185538
4. Kring AM, Barch DM. The motivation and pleasure dimension of negative symptoms: neural substrates and behavioral outputs. Eur Neuropsychopharmacol. 2014; 24(5):725. doi: https://doi.org/10. 1016/j.euroneuro. 2013.06.007
5. Berridge KC. The debate over dopamine's role in reward:the case for incentive salience. Psychopharmacology (Berl).2007; 191(3): 391-431. doi: https://doi.org/10.1007/s00213-006-0578-x
6. Berridge KC, Robinson TE. What is the role of dopamine in reward: hedonic impact, reward learning, or incentive salience? Brain Res Brain Res Rev. 1998; 28(3): 309. doi:https://doi.org/10.1016/s0165-0173(98)00019-8
7. Gard DE, Kring AM, Gard MG, Horan WP, Green MF.Anhedonia in schizophrenia: distinctions between anticipatory and consummatory pleasure. Schizophr Res. 2007; 93(1): 253-260. doi: https://doi.org/10.1016/j.schres.2007.03.008
8. Favrod J, Ernst F, Giuliani F, Bonsack C. Validation of the Temporal Experience of Pleasure Scale (TEPS) in a Frenchspeaking environment. L'Encephale. 2009; 35(3): 241-248.doi: https://doi.org/10.1016/j.encep.2008.02.013
9. Strauss GP, Wilbur RC, Warren KR, August SM, Gold JM.Anticipatory vs. consummatory pleasure: What is the nature of hedonic deficits in schizophrenia? Psychiatry Res. 2011; 187(1-2): 36. doi: https://doi.org/10.1016/j.psychres.2011.01.012
10. Gooding DC, Pflum MJ. The nature of diminished pleasure in individuals at risk for or affected by schizophrenia.Psychiatry Res. 2012; 198(1): 172-173. doi: https://doi.org/10.1016/j.psychres. 2011.07.029
11. Chan RC, Shi Y-f, Lai M-k, Wang Y-n, Wang Y, Kring AM. The Temporal Experience of Pleasure Scale (TEPS): exploration and confirmation of factor structure in a healthy Chinese sample. Plos ONE. 2012; 7(4): e35352. https://doi.org/10.1371/journal.pone.0035352
12. Li Z, Lui SS, Geng F-l, Li Y, Li W-x, Wang C-y, et al.Experiential pleasure deficits in different stages of schizophrenia. Schizophr Res. 2015; 166(1): 98-103. doi:https://doi.org/10.1016/j.schres. 2015.05.041
13. Mandal MK, Pandey R, Prasad AB. Facial expressions of emotions and schizophrenia: a review. Schizophr Bull. 1998;24(3): 399-412. doi: https://doi.org/10.1093/oxfordjournals.schbul.a033 335
14. Kring AM, Moran EK. Emotional response deficits in schizophrenia: insights from affective science. Schizophr Bull. 2008; 34(5): 819-834. doi: https://doi.org/10.1093/schbul/sbn071
15. Earnst KS, Kring AM. Construct validity of negative symptoms: an empirical and conceptual review. Clin Psychol Rev. 1997; 17(2): 167-189. doi: https://doi.org/10.1016/s0272-7358 (96)00052-9
16. Shi YF, Wang Y, Cao XY, Wang YN, Zong JG, Xu T, et al.Experience of pleasure and emotional expression in individuals with schizotypal personality features. Plos ONE.2012; 7(5): e34147. doi: https://doi.org/10.1371/ journal.pone.0034147
17. Chan RC, Wang Y, Huang J, Shi Y, Wang Y, Hong X, et al. Anticipatory and consummatory components of the experience of pleasure in schizophrenia: cross-cultural validation and extension. Psychiatry Res. 2010; 175(1): 181-183. doi: https://doi.org/10.1016/j.psychres.2009.01.020
18. Andreasen NC, Olsen S. Negative v positive schizophrenia:Definition and validation. Arch Gen Psychiatry.1982; 39(7): 789-794. doi: https://doi.org/10.1001/archpsyc.1982.042900700250 06
19. Oorschot M, Lataster T, Thewissen V, Lardinois M, Wichers M, Os JV, et al. Emotional experience in negative symptoms of schizophrenia--no evidence for a generalized hedonic deficit. Schizophr Bull. 2013; 39(1): 217. doi: https://doi.org/10.1093/schbul/sbr137
20. Kohler CG, Bilker W, Hagendoorn M, Gur RE, Gur RC.Emotion recognition deficit in schizophrenia: association with symptomatology and cognition. Biol Psychiatry.2000; 48(2): 127-136. doi: https://doi. org/10.1016/s0006-3223(00)00847-7
21. Schneider F, Gur RC, Gur RE, Shtasel DL. Emotional processing in schizophrenia: neurobehavioral probes in relation to psychopathology. Schizophr Res. 1995; 17(1): 67.doi: https://doi. org/10.1016/0920- 9964(95)00031-g
22. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th ed. Washington, DC: APA;1994
23. Gong YX. [Manual of Wechsler Adult Intelligence Scale-Chinese Version]. Changsha: Chinese Map Press; 1989. Chinese
24. Kay SR, Flszbein A, Opfer LA. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr Bull. 1987; 13(2): 261. doi: https://doi.org/10.1093/schbul/13.2.261
25. Rabinowitz J, Werbeloff N, Caers I, Mandel FS, Stauffer V,Menard F, et al. Negative symptoms in schizophrenia – the remarkable impact of inclusion definitions in clinical trials and their consequences. Schizophr Res. 2013; 150(2-3): 334.doi: https://doi.org/10.1016 /j.schres. 2013.06.023
26. Kinon BJ, Noordsy DL, Liu-Seifert H, Gulliver AH, Ascher-Svanum H, Kollack-Walker S. Randomized, double-blind 6-month comparison of olanzapine and quetiapine in patients with schizophrenia or schizoaffective disorder with prominent negative symptoms and poor functioning. J Clin Psychopharmacol. 2006; 26(5): 453-461. doi: https://doi.org/10.1097/01.jcp.0000236 658 .6286.25
27. Stauffer VL, Song G, Kinon BJ, Aschersvanum H, Chen L,Feldman PD, et al. Responses to antipsychotic therapy among patients with schizophrenia or schizoaffective disorder and either predominant or prominent negative symptoms. Schizophr Res. 2012; 134(2–3): 195-201. doi:https://doi.org/10.1016/j. schres.2011.09.028
28. Möller HJ, Riedel M, Müller N, Fischer W, Kohnen R. Zotepine versus placebo in the treatment of schizophrenic patients with stable primary negative symptoms: a randomized double-blind multicenter trial.Pharmacopsychiatry. 2004; 37(6): 270-278. doi: https://doi.org/10.1055/s-2004-8 32683
29. Gard DE, Gard MG, Kring AM, John OP. Anticipatory and consummatory components of the experience of pleasure: a scale development study. J Res Pers. 2006; 40(6): 1086-1102.doi: https://doi. org/10.1016/j.jrp.2005.11.001
30. Kring AM, Smith DA, Neale JM. Individual differences in dispositional expressiveness: development and validation of the Emotional Expressivity Scale. J Pers Soc Psychol. 1994;66(5): 934. doi: https://doi.org/10.1037//0022-3514.66.5.934
31. Chan RCK, Wang Y, Li H, Shi Y, Wang Y, Liu W, et al. A 2-stage factor analysis of the Emotional Expressivity Scale in the Chinese context. Psychologia. 2010; 53(1): 44-50. doi: https://doi.org/10. 2117/psysoc.2010.44
32. Martin EA, Becker TM, Cicero DC, Docherty AR, Kerns JG.Differential associations between schizotypy facets and emotion traits. Schizophr Res. 2011; 187(1–2): 94-99. doi:https://doi.org/10.1016/j.psychres.2010.12.028
33. Schlosser DA, Fisher M, Gard D, Fulford D, Loewy RL,Vinogradov S. Motivational deficits in individuals at-risk for psychosis and across the course of schizophrenia. Schizophr Res. 2014; 158(1-3): 52. doi: https://doi.org/10.1016/j.schres.2014.06.024
34. Chao Y, Tammy Y, Qi-Jing Y, Zhen J, Cheung EFC, Xun L, et al.Rostral medial prefrontal dysfunctions and consummatory pleasure in schizophrenia: a meta-analysis of functional imaging studies. Psychiatry Res. 2015; 231(3): 187. doi:https://doi.org/10.1016/j.pscychresns. 2015.01.001
35. Yan C, Cao Y, Zhang Y, Song LL, Cheung EFC, Chan RCK. Trait and state positive emotional experience in schizophrenia: A meta-analysis. Plos ONE. 2012; 7(7): e40672. doi: https://doi.org/10.1371/journa l.pone.0040672
36. Cohen AS, Minor KS. Emotional experience in patients with schizophrenia revisited: meta-analysis of laboratory studies. Schizophr Bull. 2010; 36(36): 143-150. doi: https://doi.org/10.1093/schbul/sbn061
37. Frost KH, Strauss GP. A review of anticipatory pleasure in schizophrenia. Curr Behav Neurosci Rep. 2016; 3(3): 232-247.doi: https://doi.org/10.1007/s40473-016-0082-5
38. Lee J, Park S. Working memory impairments in schizophrenia: A meta-analysis. J Abnorm Psychol.2005; 114(4): 599. doi: https://doi.org/10.1037/0021-843x.114.4.599
39. Juckel G, Schlagenhauf F, Koslowski M, Wüstenberg T,Villringer A, Knutson B, et al. Dysfunction of ventral striatal reward prediction in schizophrenia. NeuroImage.2006; 29(2): 409-416. doi: https://doi.org/10.1016/j.neuroimage.2005.07.051
40. Horan WP, Kring AM, Blanchard JJ. Anhedonia in schizophrenia: a review of assessment strategies. Schizophr Bull. 2006; 32(2): 259-273. doi: https://doi.org/10.1093/schbul/sbj009
41. Allen JG, Haccoun DM. Sex differences in emotionality: A multidimensional approach. Human Relations. 1976; 29(8):711-722. doi: https://doi.org/10.1177/001872677602900801
42. Gross JJ, John OP. Facets of emotional expressivity: Three self-report factors and their correlates. Pers Individ Dif. 1995;19(4): 555-568. doi: https://doi.org/10.1016/0191-8869(95)00055-B
精神分裂症患者的情感体验和表达
CHU MY, L I X , LV QY, YI ZH, CHEUNG E , CHAN R
情感体验;情感表达;精神分裂症
Background: Impairments in emotional experience and expression have been observed in patients with schizophrenia. However, most previous studies have been limited to either emotional experience (especially anhedonia) or expression. Few studies have examined both the experience and expression of emotion in schizophrenia patients at the same time.
Aims: The present study aimed to examine pleasure experience and emotion expression in patients with schizophrenia. In particular, we specifically examined the relationship between emotion impairments (both pleasure experience and expression) and negative symptoms.
Methods: One hundred and fifty patients completed the Temporal Experience of Pleasure Scale and Emotional Expressivity Scale.
Results: Schizophrenia patients exhibited deficits in experiencing pleasure, but showed intact reported emotion expression. Patients with prominent negative symptoms showed reduced anticipatory pleasure,especially in abstract anticipatory pleasure.
Conclusion:The present findings suggest that patients with schizophrenia have deficits in pleasure experience, while their abilities to express emotion appear intact. Such deficits are more severe in patients with prominent negative symptoms.
[Shanghai Arch Psychiatry. 2017;29(5): 268-276.
http://dx.doi.org/10.11919/j.issn.1002-0829.217072]
1Translational Neuropsychology and Applied Cognitive Neuroscience Laboratory, Shanghai Mental Health Centre, Shanghai Jiao Tong University School of Medicine, Shanghai, China
2Neuropsychology and Applied Cognitive Neuroscience Laboratory, CAS Key Laboratory of Mental Health, Institute of Psychology, Chinese Academy of Sciences, Beijing, China
3School of Psychology, Central China Normal University, Hubei, China
4Shanghai Mental Health Centre, Shanghai Jiao Tong University School of Medicine, Shanghai, China
5Castle Peak Hospital, Hong Kong Special Administration Region, China
6Department of Psychology, University of Chinese Academy of Sciences, Beijing, China
*correspondence: Raymond Chan; Mailing address: Institute of Psychology, Chinese Academy of Sciences, 16 Lincui Road, Beijing, China; Postcode:100101; E-Mail: rckchan@psych.ac.cn
背景:精神分裂症存在情感体验和表达障碍.然而,大多数以往研究往往只局限于情感体验(尤其是快感缺乏)或只针对表达.较少有同时研究精神分裂症患者情感体验和表达.
目的:本研究旨在考察精神分裂症患者的快感体验和情感表达.尤其是,特别关注精神分裂症患者的情感障碍(包括快感体验和表达)和阴性症状之间的关系.
方法:150例患者完成了愉快情绪体验量表(Temporal Experience of Pleasure Scale)和情感表达量表(Emotional Expressivity Scale)的评估.
结果:精神分裂症患者表现出快感缺乏,但情感表达的能力完整.以阴性症状为主的精神分裂症患者在期待性愉快体验,尤其是抽象性期待愉快体验上的缺损更为明显
结论:研究结果表明,精神分裂症患者存在出快感缺乏,但他们表达情感的能力似乎完好无损.快感缺乏尤以阴性症状为主的精神分裂症患者更为突出.

a bachelor's degree from Jiangsu Normal University in 2015 and is now undertaking a master's programme in neuropsychology at the Shanghai Mental Health Centre, Shanghai Jiao Tong University School of Medicine. Her main research interests are cognitive and emotional deficits in schizophrenia spectrum disorders.
猜你喜欢
杂志排行

上海精神医学的其它文章
- Mismatch Negativity in Han Chinese Patients with Schizophrenia: A Meta-Analysis
- Abnormal Concentration of GABA and Glutamate in The Prefrontal Cortex in Schizophrenia.-An in Vivo 1H-MRS Study
- Pretreatment Serum MCP-1 Level Predicts Response to Risperidone in Schizophrenia
- A Cross-Sectional Study on the Characteristics of Tardive Dyskinesia in Patients with Chronic Schizophrenia
- Multidimensional Approaches for A Case of Severe Adult Obsessive - Compulsive Disorder
- Psychiatry and Cinema: What Can We Learn from the Magical Screen?