术中冲洗液在结直肠癌术后切口感染预防中的应用*
2017-11-02彭联明蔡晶晶何亚光黄天磊
彭联明,蔡晶晶,何亚光,黄天磊
(浙江省宁波市第九医院 肛肠外科,浙江 宁波 315000)
术中冲洗液在结直肠癌术后切口感染预防中的应用*
彭联明,蔡晶晶,何亚光,黄天磊
(浙江省宁波市第九医院 肛肠外科,浙江 宁波 315000)
目的探讨术中冲洗液对结直肠癌术后切口感染预防中的应用。方法选取该院2012年1月-2015年12月行结直肠癌腹腔镜手术病例350例,随机分组,对患者术中分别使用无菌生理盐水、0.50%甲硝唑组、0.50%聚维酮碘液组,同时部分冲洗液在使用前进行加温至37 ~ 38℃,记录手术时间、手术部位,术后观察患者的切口感染情况,发生切口感染的患者,及时送分泌物做病原学检查;统计上采用单因素分析和Logistic多因素回归分析,分别对年龄、手术时间、手术部位、冲洗液种类、冲洗液温度行统计学分析。结果患者年龄≥60岁、手术时间≥2 h的切口感染率均高于年龄<60岁、手术时间<2 h的患者,差异有统计学意义(P<0.05);生理盐水组、0.50%甲硝唑、0.50%聚维酮碘液组,两两组间比较,0.50%甲硝唑和0.50%聚维酮碘液组的感染率分别为7.69%和8.55%,明显低于生理盐水组的16.38%;使用加温后的冲洗液的感染率低于常温冲洗液,分别为7.22%和14.71%,差异有统计学意义(P<0.05)。结论患者年龄≥60岁、手术时间≥2 h均是结直肠癌行腹腔镜手术后切口感染的危险因素,而选择0.50%甲硝唑、0.50%聚维酮碘液组和加温的冲洗液,是手术切口感染的保护性因素,可以应用到预防腹腔镜手术后切口感染中。
腹腔镜;结直肠癌;年龄;冲洗液
术后切口感染是结直肠癌术后常见的并发症,发生率约为4.00%~30.00%[1]。手术切口感染(incisional surgical site infection,ISSI),是手术后3 d以内发生的切口皮肤、皮下组织或深部软组织的感染[2]。已有一些临床研究证实,体质指数、手术方式、手术时间和术中大量出血等是术后切口感染预后的独立影响因素[3-5]。其中腹腔镜手术是术后切口感染预后的保护性因素[6]。不断对腹腔镜手术技术的改进,如单切口腹腔镜的开展等[7],是对术后预防感染的有效措施。在此基础上,对手术中使用的冲洗液进行选择,包括冲洗液的种类和温度,希望能进一步预防术后切口的感染。
1 资料与方法
1.1 一般资料
本研究行前瞻性研究,选取本院2012年1月-2015年12月行结直肠癌腹腔镜手术的病例。病例数共350例,随机分为3组,根据手术中使用冲洗液的不同分别为生理盐水组、0.50%甲硝唑组和0.50%聚维酮碘液组。纳入标准:①术前行肠镜病理标本证实为结直肠腺癌;②符合腹腔镜手术适应证;③患者及家属同意接受手术治疗。排除标准:其他结直肠肿瘤(如神经内分泌肿瘤、间质瘤和黑色素瘤等),合并严重基础疾病(如严重高血压,心脏病等),有多器官的恶性肿瘤转移(腹膜转移、肺转移等)。一般资料情况如下,患者年龄29~70岁,平均年龄(58.0±9.8)岁。同时,取部分常温组冲洗液和加温至37~38℃。根据切口感染标准,分为感染组(38例)和非感染组(312例)。本研究通过医院伦理委员会的批准。
1.2 方法
患者术前1 d服用复方聚乙二醇电解质散冲服至清水样便,口服甲硝唑片,行充分的肠道准备。预防性应用抗生素,于手术前30 min静脉滴注头孢类抗生素。行全身麻醉后,经腹行腹腔镜切除结直肠肿瘤部位,缝合肠管或造瘘后,应用生理盐水冲洗腹腔后,3组分别再用生理盐水、0.50%甲硝唑和0.50%聚维酮碘液冲洗腹腔,留置引流管,分层缝合切口,敷上纱布。术中记录手术部位、手术时间和出血量等。病变部位送病理科。术后观察切口愈合情况,常规拔除引流管,有切口感染或腹腔感染患者可根据情况适当延长时间。如出现切口感染,未使用抗感染治疗前,取分泌物做病原学检查,指导抗生素的使用。
切口感染诊断标准:手术后30 d内,切口处皮肤和皮下组织,见红、肿、热、痛或有脓性分泌物,或深部切口引流出脓性分泌物,体温≥38℃,局部疼痛,病原学检查或组织病理学或影像学检查发现切口感染等证据。
1.3 统计学方法
采用SPSS 19.0统计学软件,根据年龄、性别、手术部位、手术时间、术中冲洗液种类、冲洗液温度这些因素,对术后切口感染的可能影响因素采用单因素分析,当P<0.05时,组间比较差异有统计学意义。两两组间比较,采用kap分析。将年龄≥60岁、手术时间>2 h、术中用0.50%甲硝唑溶液、用0.50%聚维酮碘液冲洗和用加温的冲洗液,这些因素采用Logistic多因素回归分析,P<0.05为差异有统计学意义。
2 结果
2.1 研究对象的单因素分析
在腹腔镜下行结直肠癌术,年龄≥60岁发生切口感染率为15.00%,高于年龄<60岁的患者5.33%的切口感染率;手术时间≥2 h的感染率为14.00%高于手术时间<2 h组;差异有统计学意义(P<0.05)。术中使用0.50%甲硝唑和0.50%聚维酮碘液的切口感染发生率分别为7.69%和8.55%,均低于单纯使用生理盐水作为冲洗液的感染发生率16.38%;加温的冲洗液的感染发生率低于使用常温的冲洗液,分别为7.22%和14.71%,差异均有统计学意义(P=0.012,P=0.024)。见表 1。
2.2 Logistic多因素回归分析
将上述可能对切口感染影响的因素进行Logistic多因素回归分析(表2)。年龄≥60岁是影响切口感染的主要因素之一(P=0.001)。将0.50%甲硝唑和0.50%聚维酮碘液作为冲洗液,或对冲洗液进行加温,都是切口感染是保护性因素之一,P<0.05,OR^<1.0。
2.3 病原学检查
患者共350例,腹腔镜下行结直肠癌手术后,发生切口感染38例,感染率为10.86%,34例检出病原菌,阳性率达89.47%,均采集切口分泌物行病原学检查,培养出病原菌38株,以大肠埃希菌、粪肠球菌为主。见表3。
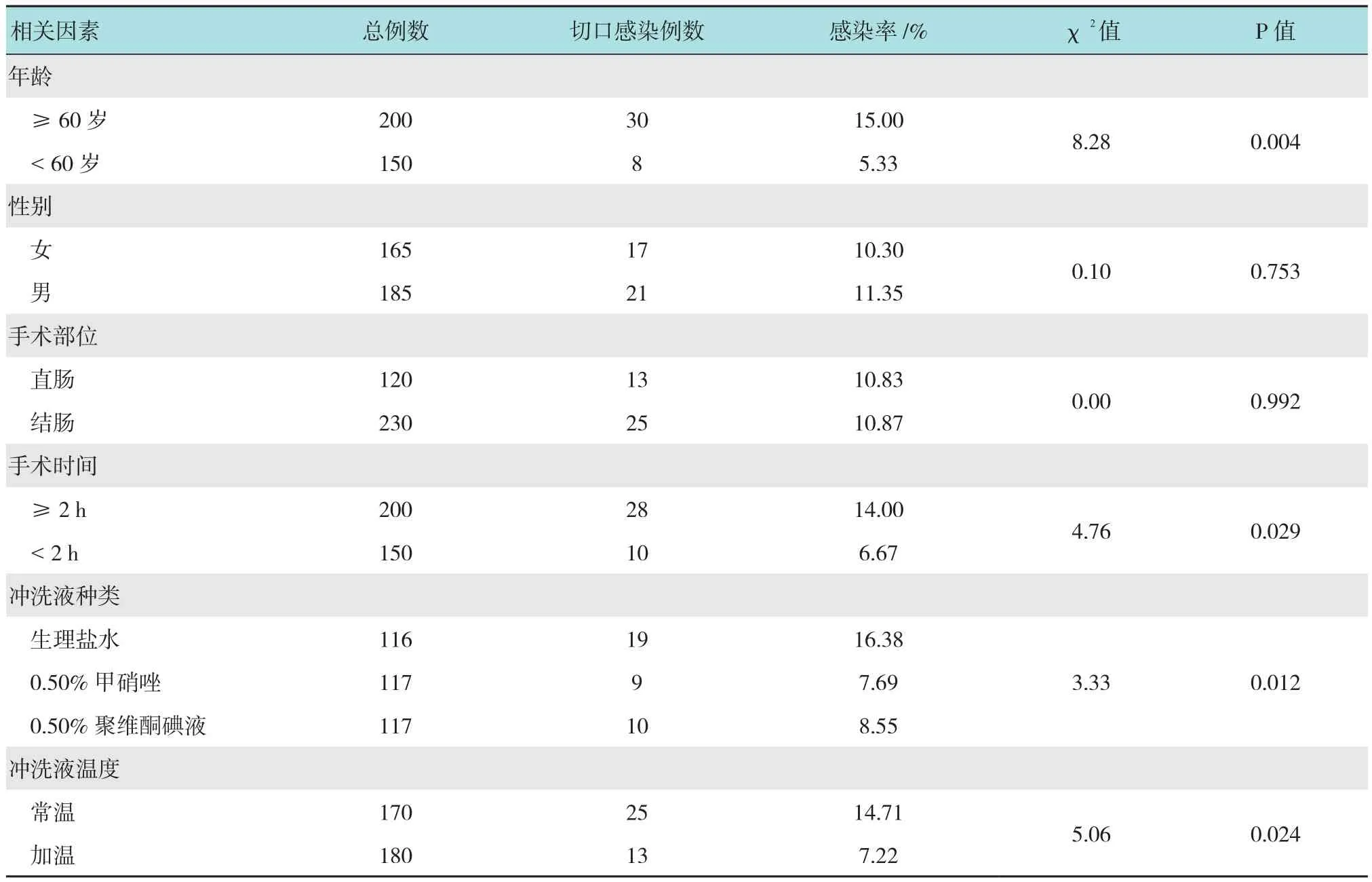
表1 结直肠癌患者根治术后手术部位感染的单因素分析及感染率Table 1 Univariate analysis of the risk factors for the postoperative surgical site infections in the colorectal cancer patients undergoing the radical surgery and the infection rates
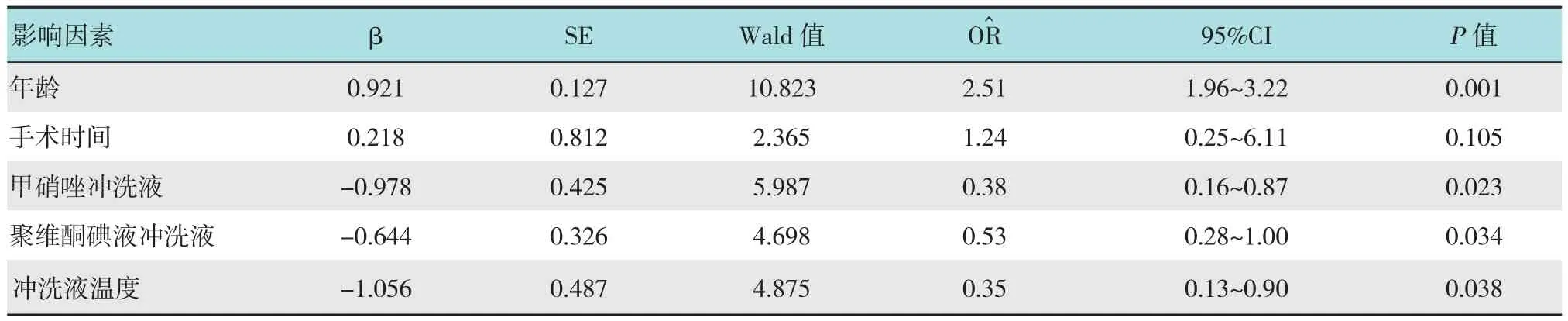
表2 影响结直肠癌手术患者切口感染的多因素回归分析Table 2 Multivariate regression analysis of the factors for incision infection in the patients with colorectal cancer

表3 患者术后切口感染病原菌构成比Table 3 Constituent ratios of the pathogens causing the postoperative incision infections
3 讨论
术后发生切口感染,不仅会延长患者的住院时间,也会影响患者的术后恢复,将会增加医疗费用。在结合了已有的研究文献,术后的切口感染主要发生在浅表部位。研究结果显示,共有38例患者发生了切口处感染,感染率为10.86%,年龄、手术时间长、术中冲洗液的选择为发生感染的相关危险因素(P<0.05)。说明手术切口部位的感染在结直肠癌行腹腔镜手术患者中有一定的发生率,患者的临床特征和手术中的一些操作等因素均跟切口感染有密切的关系[8]。引起切口感染的原因很多,但切口污染病原微生物是最主要的原因。因此,病原微生物寄生的环境是影响是否发生感染的重要原因[9]。研究表明,单个细菌进入腹腔内,以8 min倍增的速度来计算,24 h后其数量可达2 144个,远超过机体的清除能力[10]。所以彻底清除有利于细菌生长的污染物,防治细菌植入腹腔和切口处,是预防切口感染的关键。
冲洗液用来冲洗腹腔和切口,是预防切口感染的主要方法之一。聚维酮碘,又称碘伏,是一种广谱、无毒、稳定性好的消毒杀菌剂,对皮肤无刺激性和无黄染,可在水中溶解,释放出游离碘,菌蛋白与碘结合后可变性坏死,使细菌变性坏死[11]。术中冲洗可以快速灭菌,同时保持切口洁净,清洁污染物[12]。甲硝唑是抗厌氧菌性的药物,是预防和治疗厌氧菌感染的首选药物,切口感染的病原菌种以厌氧菌为主,临床上已有报道采用抗厌氧菌感染的治疗后,外科手术感染率明显下降[13-14]。
手术时间的延长,可能使无菌的腹内环境暴露于空气的时间延长,同时时间较长的患者病情较重、出血量较多,均会引起患者免疫力的下降[15-16],尤其针对结直肠癌这种恶性肿瘤,患者随着年龄的增长,手术创伤应激可导致患者对营养物质的吸收能力下降,也是引起切口感染的高危因素。
保温对于机体的恢复有一定保护性作用[17],将冲洗液加温至人正常体温36~37℃,可减少患者围手术期的体温散失。本研究显示,使用加温的冲洗液对比常温的冲洗液可明显降低切口感染率至7.22%,牟德芹[18]就围手术期保温采取了加温冲洗液、手术室温度恒定等措施,研究也说明在围手术期对机体行保温措施可降低切口的感染率。有文献显示在围手术期采用合适的保温措施,如将冲洗液加温等,可以明显降低手术部位感染的发生率[18-19]。
本研究显示,切口感染的病原菌包括大肠埃希菌、粪肠球菌、金黄色葡萄球菌、表皮葡萄球菌和铜绿假单胞菌。在正常肠道中存在的细菌主要为革兰阴性菌,以大肠埃希菌、粪肠球菌为主[20],提示切口感染的病原菌主要来源于内源性肠道。其他研究中也显示胃肠道手术的切口感染中以内源性肠道细菌为主[21]。而金黄色葡萄球菌和表皮葡萄球菌来源于皮肤正常定植菌,铜绿假单胞菌是医源性感染的主要病原菌。
[1]GROSSO G, BIONDI A, MARVENTANO S, et al. Major postoperative complications and survival for colon cancer elderly patients[J]. BMC Surg, 2012, 12(Suppl 1): S20.
[2]TIMMERMANS L, DEERENBERG E B, LAMME B, et al.Parastomal hernia is an independent risk factor for incisional hernia in patients with end colostomy[J]. Surgery, 2014, 155(1):178-183.
[3]郑晖, 池畔, 林惠铭, 等. 结直肠癌术后手术部位切口感染的预后因素分析[J]. 中华外科杂志, 2016, 54(6): 424-428.
[3]ZHENG H, CHI P, LIN H M, et al. Prognostic factors of postoperative incisional surgical site infections for colorectal cancer[J]. Chinese Journal of Surgery, 2016, 54(6): 424-428.Chinese
[4]薛春丽, 万琼, 郭欣. 结直肠癌患者手术切口感染因素及预防对策[J]. 中华医院感染学杂志, 2013, 23(16): 3937-3938.
[4]XUE C L, WAN Q, GUO X. Risk factors for surgical incision infection in colorectal cancer patients and prevention counter measures[J]. Chinese Journal of Nosocomiology, 2013, 23(16):3937-3938. Chinese
[5]杨玉波, 关铁军, 王斌, 等. 直肠癌手术切口感染的危险因素分析与预防对策[J]. 中华医院感染学杂志, 2015, 25(1): 183-186.
[5]YANG Y B, GUAN T J, WANG B, et al. Risk factors for incision infections in patients underging rectal cancer surgery and prevention countermeasures[J]. Chinese Journal of Nosocomiology,2015, 25(1): 183-186. Chinese
[6]薛小军, 聂凯, 陈锦荣, 等. 腹腔镜与开腹远端胃切除术后手术部位感染的Meta分析[J]. 中国内镜杂志, 2016, 22(3): 46-50.
[6]XUE X J, NIE K, CHEN J R, et al. Comparison of surgical site infection between laparoscopic distal gastrectomy and open distal gastrectomy for gastric cancer: A Meta-analysis[J]. China Journal of Endoscopy, 2016, 22(3): 46-50. Chinese
[7]KELLER D S, FLORES-GONZALEZ J R, IBARRA S, et al.Review of 500 single incision laparoscopic colorectal surgery cases - lessons learned[J]. World J Gastroenterol, 2016, 22(2): 659-667.
[8]CHEN Z, HE X, HUANG J, et al. Short-term outcomes between laparoscopy-assisted and open colorectomy for colorectal cancer in elderly patients: A case-matched control study[J]. Mol Clin Oncol,2015, 3(5): 1155-1159.
[9]KATSUNO G, FUKUNAGA M, NAGAKARI K, et al. Short-term and long-term outcomes of single-incision versus multi-incision laparoscopic resection for colorectal cancer: A propensity-scorematched analysis of 214 cases[J]. Surg Endosc, 2016, 30(4): 1317-1325.
[10]MICHALOPOULOS A, SPAROS L. Post-operative wound infections[J]. Nurs Stand, 2003, 17(44): 53-60.
[11]成健, 杨洋. 0.50%聚维酮碘联合0.50%甲硝唑预防miles术后切口感染[J]. 解放军护理杂志, 2015, 32(7): 47-48.
[11]CHENG J, YANG Y. 0.50% Povidone -iodine combined 0.50%Metronidazole in preventing incision infection after Miles surgery[J]. Nurs J Chin PLA, 2015, 32(7): 47-48. Chinese
[12]邓永强, 邢启德, 孙阳阳, 等. 聚维酮碘的特性与临床应用[J].中华医院感染学杂志, 2016, 26(3): 627-629.
[12]DENG Y Q, XING Q D, SUN Y Y, et al. Properties and clinicial applications of povidone iodine[J]. Chinese Journal of Nosocomiology, 2016, 26(3): 627-629. Chinese
[13]李柘黄, 韦峰, 许南方, 等. 稀碘伏溶液浸泡术野对降低术后脊柱手术切口感染风险的效果[J]. 中国脊柱脊髓杂志, 2016,26(3): 244-248.
[13]LI Z H, WEI F, XU N F, et al. Evaluation of dilute betadine immersion in reducing postoperative surgical site infection after spine surgery[J]. Chinese Journal of Spine and Spinal Cord, 2016,26(3): 244-248. Chinese
[14]顾伟平, 徐耀庭, 李杜渐, 等. 冲洗液控温对经尿道前列腺电切术患者血浆D二聚体、选择素P和选择素E的影响[J]. 中国内镜杂志, 2013, 19(11): 1126-1129.
[14]GU W P, XU Y T, LI D J, et al. Effects of perioperative hypothermia on change of the serum level of D-dimer, P-selectin and E-selectin during TURP[J]. China Journal of Endoscopy,2013, 19(11): 1126-1129. Chinese
[15]RAMIREZ M F, AI D, BAUER M, et al. Innate immune function after breast, lung, and colorectal cancer surgery[J]. J Surg Res,2015, 194(1): 185-193.
[16]王世芳, 杨先智, 赵旋, 等. 胃肠道手术患者术前免疫功能及手术时间对术后切口感染的风险评价[J]. 中华医院感染学杂志, 2016, 26(17): 4023-4025.
[16]WANG S F, YANG X Z, ZHAO X, et al. In fl uence of preoperative immune function and operation duration on postoperative incision infections in patients undergoing gastrointestianl tract surgery[J].Chinese Journal of Nosocomiology, 2016, 26(17): 4023-4025.Chinese
[17]ERDLING A, JOHANSSON A. Core temperature-the intraoperative difference between esophageal versus nasopharyngeal temperatures and the impact of prewarming, age, and weight: a randomized clinical trial[J]. AANA J, 2015, 83(2): 99-105.
[18]牟德芹. 围术期保温对结直肠癌手术切口感染影响的观察[J].中华医院感染学杂志, 2012, 22(3): 523-524.
[18]MU D Q. Effect of heat preservation on surgical incision in colorectal cancer operation during perioperative period[J].Chinese Journal of Nosocomiology, 2012, 22(3): 523-524.Chinese
[19]何文英, 先疆燕, 王忠, 等. 围手术期保温措施对患者手术部位感染影响的荟萃分析[J]. 中华医院感染学杂志, 2016,26(12): 2858-2861.
[19]HE W Y, XIAN J Y, WANG Z, et al. In fl uence of perioperative insulation measures on surgical site infections: a meta-analysis[J].Chinese Journal of Nosocomiology, 2016, 26(12): 2858-2861.Chinese
[20]GU S, CHEN D, ZHANG J N, et al. Bacterial community mapping of the mouse gastrointestinal tract[J]. PLoS One, 2013, 8(10):e74957.
[21]汪青, 王雨, 方俊, 等. 结直肠癌患者手术部位感染的病原菌分析[J]. 中华医院感染学杂志, 2016, 26(13): 2930-2932.
[21]WANG Q, WANG Y, FANG J, et al. Distribution of pathogenic bacteria causing surgical site infections in patients with colorectal cancer[J]. Chinese Journal of Nosocomiology, 2016, 26(13):2930-2932. Chinese
Application of washing f uid in preventing postoperative incisional infection of colorectal cancer*
Lian-ming Peng, Jing-jing Cai, Ya-guang He, Tian-lei Huang
(Department of Anorectal Surgery, the Ninth Hospital, Ningbo, Zhejiang 315000, China)
ObjectiveTo explore the application of washing fl uid in the prevention of postoperative incision infection of colorectal cancer.Methods350 patients with colorectal cancer underwent colorectal surgery from Jan.2012 to Dec. 2015 were randomly divided into three groups: sterile saline, 0.50% metronidazole, 0.50% Povidoneiodine solution group, while part of the rinse liquid heated to 37 ~38℃ before use, then record the operation time,surgical site, postoperative incision infection, incision infection, timely delivery statistical analysis was performed by using single factor analysis and logistic multivariate regression analysis. Age, operation time, surgical site, type of irrigating fl uid and temperature of fl ushing fl uid were analyzed statistically.ResultsThe incision infection rate of the patients ≥60 years old and the operation time ≥2 h was higher than the age <60 years, and the operation time was less than 2 h,P< 0.05, the difference was statistically significant; 0.50% metronidazole, 0.50% Povidoneiodine solution group, the infection rates of 0.50% metronidazole and 0.50% povidone-iodine group were 7.69% and 8.55%, respectively, which were signi fi cantly lower than those of the saline group 16.38% The infection rate of the rinsing fl uid after heating was 7.22% and 14.71%, respectively, lower than that of the normal temperature rinsing solution (P< 0.05), the difference was statistically signi fi cant.ConclusionsThe risk factors of incisional infection in colorectal cancer patients with colorectal cancer were : ≥60 years of age and ≥2 h of operation, while 0.50%metronidazole, 0.50% povidone-iodine solution and heated washing fl uid were protective factors. It can be applied to prevent incision infection after laparoscopic surgery.
laparoscopy; colorectal cancer; age; washing fl uid
R735.34
A
10.3969/j.issn.1007-1989.2017.08.004
1007-1989(2017)08-0018-05
2017-01-17
宁波市医学科技计划项目(No:2016A34)
(彭薇 编辑)
