DWl在宫腔积脓和宫腔积液鉴别诊断中的价值
2017-09-29赵宏伟翟泽清付立平王艳莉
赵宏伟,翟泽清,付立平,王艳莉
DWl在宫腔积脓和宫腔积液鉴别诊断中的价值
赵宏伟1,翟泽清1,付立平2*,王艳莉1
作者单位:1. 葛洲坝集团中心医院放射科,宜昌443000 2. 武汉大学中南医院三峡医院放射科,宜昌 443000
目的 探讨DWI序列对宫腔积脓和宫腔积液的鉴别诊断价值。材料与方法 回顾分析44例经手术病理或临床证实的宫腔积脓和宫腔积液患者的宫腔DWI信号特征,测量其表观扩散系数(apparent diffusion coef ficient,ADC),比较其差异,并绘制受试者工作特征(receiver operating characteristic,ROC)曲线。结果 20例宫腔积脓在DWI上18例呈高信号,1例呈不均匀高信号,1例呈低信号,平均ADC值为(0.78±0.21)×10-3mm2/s;24例宫腔积液在DWI上22例呈低信号,2例呈高信号,平均ADC值为(1.81±0.38)×10-3mm2/s。两者ADC值差异有统计学意义(P<0.001),且ADC值鉴别子宫腔积脓和积液的最佳截断点为1.20×10-3mm2/s,敏感性为91.7%,特异性为95.0%。结论 ADC值可以用于宫腔积脓和宫腔积液的鉴别,其诊断临界值为1.20×10-3mm2/s。
宫腔积脓;子宫疾病;弥散磁共振成像
子宫腔积脓和积液是盆腔常见病,常规CT和MRI检查对其定位和定性诊断有重要价值,但有时鉴别诊断有一定困难。磁共振扩散加权成像(diffusion weighted imaging,DWI)是反映活体组织中水分子扩散特性,并进行水分子扩散测量与成像的方法,已用于盆腔脓肿和盆腔肿瘤的诊断和鉴别诊断,在宫腔积脓和宫腔积液的鉴别诊断中也有不少报道。笔者对44例子宫腔积脓和积液的DWI信号特征和表观扩散系数(apparent diffusion coefficient,ADC)值进行分析,旨在探讨DWI和ADC值在宫腔积脓和积液鉴别诊断中的价值。
1 材料与方法
1.1 研究对象
2013年5月至2016年5月间纳入46例经盆腔超声或CT检查发现宫腔积脓或积液并欲行盆腔MR检查患者。临床表现:腹痛40例,发热23例,血常规白细胞及中性粒细胞升高25例。纳入标准:(1)盆腔超声或CT检查发现的最小积脓和积液体积为0.5 cm×1.0 cm×2.0 cm;(2) MRI检查后短期内经病理或临床分析宫腔液体性质,其中20例宫腔积脓患者及21例宫腔积液患者经探宫引流并病理细胞学检查确诊,3例宫腔积液未经特殊处理,短期影像随访后积液消失;(3)无幽闭恐惧症、心脏起搏器、人工耳蜗植入等MRI检查禁忌证,无子宫节育器及腰骶部金属植入史。本研究经伦理委员会批准,且所有受检者均已签署知情同意书。
1.2 检查设备及技术
1.2.1 检查设备及对比剂
检查设备:西门子公司Magnetom ESSENZA 1.5 T超导型MR机,体部正交线圈。对比剂为非离子型钆喷替酸葡甲胺(Gd-DTPA)(469.01 mg/ml),剂量0.1 mmol/kg。
1.2.2 扫描技术
平扫:均行横断面T1WI、T1WI-FS、T2WIFS、DWI、矢状面及冠状面T2WI扫描。T1WI采用自旋回波序列,T1WI-FS采用FL2D-FS序列,T2WI采用快速自旋回波序列;扫描参数:T1WI TR 700 ms,TE 8 ms;T2WI TR 2800 ms,TE 112 ms;T2WI-FS TR 3800 ms,TE 94 ms;DWI单次激发SE-EPI序列,TR 4000 ms,TE 94 ms,b值取0和1000 s/mm2,以0 s/mm2和1000 s/mm2DWI图通过计算机自动生成ADC图。图像扫描层厚5 mm,间隔0.5 mm,视野30 cm×35 cm,矩阵352×296;增强扫描对比剂为Gd-TDPA,剂量0.1 mmol/kg,注射对比剂后行横断面、矢状面、冠状面脂肪抑制T1WI扫描,扫描序列与T1WI-FS平扫的参数相同。
1.2.3 盆腔DWI后处理
由1名有5年MRI后处理经验的放射科医师行盆腔DWI后处理,且事先并不知晓患者临床信息,勾画类圆形感兴趣区(region of interest,ROI)置于子宫腔内积液区,并注意避开周围子宫内膜及肌层;对每一病例于ADC图上测量出病变的ADC值,取三次测量平均值,每个ROI大小约200~300像素,并依据积液区DWI信号强度与正常臀大肌对比,定为低、等或高信号。
1.3 统计分析
所得数据经SPSS 19.0统计软件处理。两组实验ADC值均以表示,两组病变间ADC值比较采用两样本均数差别的t检验,以P<0.05为差异有统计学意义。通过绘制受试者工作特征(receiver operating characteristic,ROC)曲线,计算诊断试验的敏感性、特异度及曲线下的面积(area under curve,AUC)。
2 结果
排除幽闭恐惧症者1例及未行临床宫腔积液性质分析者1例,实验共纳入44位受试者,包括宫腔积脓20例,平均年龄(61.9±5.2)岁,宫腔积液24例,平均年龄(44.6±6.3)岁。其中,急性或慢性子宫内膜炎并宫颈管阻塞造成的宫腔积脓有8例,占40.0%,老年性阴道炎并宫颈萎缩所致宫腔积脓5例,占25.0%,子宫内膜癌患者3例,占15.0%,晚期宫颈癌放射治疗后4例,占20.0%。24例宫腔积液患者中,排卵期前后的生理性宫腔积液3例,占12.5%,子宫恶性肿瘤放射治疗后的宫腔积液10例,占41.7%,宫外孕及黄体破裂后的宫腔积液4例,占16.7%,子宫肌瘤所致宫腔积液7例,占29.1%。
常规MRI和DWI表现:20例宫腔积脓MRI表现为脓液在T1WI及T1WI+FS均呈低信号,T2WI及T2WI+FS均呈高信号,18例积脓DWI呈显著高信号(图1A~C),1例DWI高信号中混有低信号,1例DWI呈低信号。增强扫描积脓未见强化,邻近的子宫内膜及肌层明显强化。24例宫腔积液MRI表现为在T1WI及T1WI+FS均呈低信号,T2WI及T2WI+FS均呈高信号,22例宫腔积液DWI呈低信号(图1D~F),2例宫腔积液DWI呈高信号或部分呈高信号。增强扫描积液未见强化,邻近的子宫内膜轻度至中度强化。宫腔积脓与积液ADC值不同,差异存在统计学意义(t=14.79,P<0.001;表1)。

表1 宫腔积脓和宫腔积液ADC值比较Tab. 1 Comparison of the ADC value of uterine empyema and uterine cavity fluid
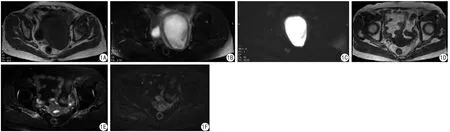
图1 A~C为宫腔积脓。A:T1WI横断面,脓液呈低信号;B:脂肪抑制T2WI横断面,脓液呈高信号;C:DWI (b=1000 s/mm2),脓液呈明显高信号。D~F为宫腔积液。D:T1WI横断面,积液呈低信号;E:脂肪抑制T2WI横断面,积液呈高信号;F:DWI (b=1000 s/mm2),积液呈低信号Fig. 1 A—C: Uterine empyema. A: Axial T1WI, purulent fluid showed low signal. B: Axia STIR/T2WI, purulent fluid showed high signal. C: DWI (b=1000 s/mm2), purulent fluid showed high signal. D—F: Uterine cavity fluid. D: Axia T1WI, uterine cavity fluid showed low signal. E: Axia STIR/T2WI, uterine cavity fluid showed high signal. F: DWI (b=1000 s/mm2), uterine cavity fluid showed low signal.

图2 宫腔积脓和宫腔积液ADC值的ROC曲线Fig. 2 ROC plots of ADC value of uterine empyema and uterine cavity fluid.
通过分析宫腔积脓和宫腔积液ADC值的ROC曲线(图2)显示,ADC值的曲线下的面积为0.968,95%置信区间为0.919~1.000,约登指数最大值为0.87,其对应的ADC值最佳截断点为1.20×10-3mm2/s,提供的敏感性为91.7%,特异性为95.0%。
3 讨论
宫腔积脓和积液治疗有所不同,前者采用探宫引流加抗生素治疗,而后者采用对症处理治疗,虽然经宫颈管探宫引流是一种并发症少、操作安全的手术,但也有引起子宫穿孔和引起感染等并发症的风险[1-2]。子宫腔积脓较多时,子宫可球状增大[3-4],子宫壁受压变薄,若不及时治疗可造成子宫穿孔及腹盆腔内感染[5-7]。因此鉴别宫腔积脓和积液的性质和病因是病人治疗的关键。宫腔积脓和宫腔积液的临床及影像表现有相似之处,其常规MRI表现有时不易鉴别。本研究显示宫腔积脓行磁共振Gd-DTPA增强扫描延迟期子宫内膜及肌层强化程度较宫腔积液更明显,但是不足以把两者有效地区分开。
DWI在鉴别细胞毒性水肿和血管源性水肿之间、囊性肿瘤和脓肿之间已有广泛应用[8],在宫腔积脓和宫腔积液的诊断中也有很多报道。本研究结果显示19例宫腔积脓(19/20) DWI呈高信号,ADC值降低;22例宫腔积液(22/24) DWI呈低信号,ADC值升高。宫腔积脓多因为子宫内膜粘连使宫腔部分或全部闭锁,或子宫颈管狭窄闭锁,或阴道粘连[9],再合并宫腔内感染引起,脓液中含有大量细菌、炎性细胞、细胞碎屑和蛋白复合物,可呈凝胶状,黏滞度高[10-11],脓液中水分子可与大分子物质相结合,水分子的扩散受到限制[12],故DWI呈高信号,ADC值降低。宫腔积脓有时可向输卵管、卵巢及腹盆腔蔓延,造成输卵管卵巢脓肿或盆腔脂肪浸润,本组20病例宫腔积脓中有1例并发输卵管卵巢脓肿,在DWI上输卵管亦呈高信号,提示盆腔DWI可监测病情进展。宫腔积液可分为生理性及病理性积液。生理性的宫腔积液,多发生在排卵后或早孕期,大多可自然消失。病理性的宫腔积液多发生于盆腔肿瘤放疗后、子宫肌瘤、宫外孕破裂及黄体破裂等[13]。宫腔积液所含的黏滞性物质少[14],炎性细胞少,液体内蛋白含量也较低,对水分子的扩散阻抗少,水分子扩散运动相对自由,水分子扩散加快,DWI呈低信号,ADC值升高。但宫腔内液体的DWI信号强度还与黏液成分及有无出血有关[15],本研究中有一例宫腔积脓的脓液内混有红细胞,造成局部DWI信号不均匀,提示单凭DWI信号强度不足以鉴别宫腔积液或积脓,需要测量ADC值进行鉴别,ADC值测量时应避开DWI信号不均匀的区域,这例患者测得的平均ADC值为1.03×10-3mm2/s,低于最佳截断点1.20×10-3mm2/s。进一步统计分析显示,宫腔积脓和宫腔积液ADC值不同,其最佳截断点为1.20×10-3mm2/s,提供的敏感性为91.7%,特异性为95.0%,表明盆腔DWI通过测量ADC值进行定量参数分析,为鉴别宫腔积脓和宫腔积液提供一个有效的无创检查手段。
综上所述,盆腔DWI的ADC值测量对子宫腔积脓和积液的鉴别诊断具有重要作用,能有效鉴别宫腔积脓和宫腔积液。
[References]
[1] Shi L. The treatment experience of 74 cases of patients with uterine empyema. Chin Continuing Med Education, 2015, (11): 81-82.石磊. 74例子宫积脓患者的治疗体会. 中国继续医学教育, 2015,(11): 81-82.
[2] Fu R, Mei CQ, Lu BF, et al. To explore the elderly pyometra misdiagnosis (Incidental report of nine cases). Clin Misdiagn Mistherapy, 2015, 28(12): 43-45.付蓉, 梅长青, 鲁必芬, 等. 老年宫腔积脓漏误诊原因探究(附九例报告). 临床误诊误治, 2015, 28(12): 43-45.
[3] Hayati F, Ahrari-Kha fiMS, Hassankhani M, et al. A rare radiographic appearance of a calcified uterus in a queen with pyometra: a case report. Veterinární Med, 2016, 61(6): 357-360.
[4] Guo YF, Guo YH, Zhang FQ. Pyometra imaging manifestations (a report of 3 cases). Chin Imaging J Integr Tradit West Med, 2006,4(5): 396-397.郭玉峰, 郭玉华, 张芳芹. 宫腔积脓影像学表现(附3例报告). 中国中西医结合影像学杂志, 2006, 4(5): 396-397.
[5] Niu AQ. Misdiagnosis reason analysis of uterine empyema complicated with perforation of the uterus in women after menopause. Clin Med Chin, 2015, 31(7): 656-658.牛爱琴. 绝经后妇女宫腔积脓并子宫穿孔20例临床分析. 中国综合临床, 2015, 31(7): 656-658.
[6] Tian KG, Qiao LY, Dong LG, et al. Etiology and clinical treatment of pelvic and abdominal abscess. Chin J Hospit Infect, 2007, 17(1): 42-44.田可歌, 乔丽雅, 董立国, 等. 盆腔、腹腔脓肿的病原学分析与临床处理. 中华医院感染学杂志, 2007, 17(1): 42-44.
[7] Xie X, Gou WL. Gynecotokology. 8th ed. Beijing: People's Medical Publishing House, 2013: 37-68.谢幸, 苟文丽. 妇产科学. 8版. 北京: 人民卫生出版社, 2013: 37-68
[8] Liu H, Cui SM. Application of diffusion weighted imaging in the evaluation of peritumoral edema of brain tumors. J Tianjin Med University (Master Thesis), 2007: 202-205.刘卉, 崔世民. 弥散加权成像技术在评价脑肿瘤瘤周水肿中的应用. 天津医科大学(硕士论文), 2007: 202-205.
[9] Sato A, Uchida A, Yamanaka Y, et al. A case of vaginal adhesion and pyometra undergone hysterectomy after methotrexate-associated lymphoproliferative disorders (MTX-LPD). J Reproduct Immunol,2016, 11(118): 125-126.
[10] Wei J, Ma QH, Ye JJ, et al. Diagnostic value of magnetic resonance DWI combined with conventional MRI in the diagnosis of abdominal and pelvic abscess. Radiol Pract, 2009, 24(4): 418-421.韦骏, 马强华, 叶建军, 等. 磁共振DWI结合常规MRI对腹盆腔脓肿的诊断价值. 放射学实践, 2009, 24(4): 418-421.
[11] Yamashita Y, Namimoto T, Mitsuzaki K, et al. Mucin-producing tumor of the pancreas: diagnostic value of diffusion-weighted echoplanar MR imaging. Radiology, 2015, 20(8): 605-609.
[12] Chan JH, Tsui EY, Luk SH, et al. Diffusion-weighted MR imaging of the liver: distinguishing hepatic abscess from cystic or necrotic tumor. Abdom Imaging, 2014, 2(6): 161-165.
[13] Jiang M, Zhao W, Yi GF, et al. MRI features of uterine leiomyomas and high intensity focused ultrasound ablation. J Intervent Radiol,2014, 23(4):314-319.姜曼, 赵卫, 易根发, 等. 子宫肌瘤MRI特征与高强度聚焦超声消融疗效. 介入放射学杂志, 2014, 23(4): 314-319.
[14] Ma SK, Gao JZ, Wu LY et al. Clinical analysis of 151 cases of uterine cavity effusion after radiotherapy for cervical cancer. Chin J Radiat Oncol, 2007, 16(6): 451-454.马绍康, 高菊珍, 吴令英, 等. 子宫颈癌放疗后子宫腔积液151例临床分析. 中华放射肿瘤学杂志, 2007, 16(6): 451-454.
[15] Kim SH, Yang DM, et al. Unusual causes of tubo-ovarian abscess:CT and MR imanging findings. Radiographics, 2014, 24(6):1575-1589.
Value of DWI in differential diagnosis of uterine empyema and uterine cavity fluid
ZHAO Hong-wei1, ZHAI Ze-qing1, FU Li-ping2*, WANG Yan-li1
1Department of Radiology, Central Hospital of Gezhouba group, Yichang 443000,China
2Department of Radiology, Three Gorges branch of hospital, Zhongnan Hospital of Wuhan University, Yichang 443000, China
*Fu LP, E-mail: gzbmr_000@163.com
Objective: To investigate the value of DWI sequence in the differential diagnosis of uterine empyema and uterine cavity fluid. Materials and Methods:Forty-four cases of DWI signal of uterine empyema and uterine cavity fluid were retrospectively analyzed, these cases were con firmed by pathology or clinic. Afterwards the apparent diffusion coefficient (ADC) was measured and the receiver operating characteristic (ROC) curve of the ADC value was drawn. Results: In DWI, 20 cases of uterine empyema, 18 cases showed high signal, 1 case showed inhomogeneous high signal, 1 case showed low signal, mean ADC value was (0.78±0.21)×10-3mm2/s. In DWI, 24 cases of uterine cavity fluid, 22 cases showed low signal, 2 cases showed high signal, mean ADC value was (1.81±0.38)×10-3mm2/s. There was signi ficant difference in ADC value between the two groups (P<0.001), the optimum cutoff point for ADC values was 1.20×10-3mm2/s, the sensitivity was 91.7% and the speci ficity was 95.0%.Conclusions: The ADC value can be used to identify the uterine empyema and uterine cavity fluid, and the cutoff value was 1.20×10-3mm2/s.
Pyometra; Uterine diseases; Diffusion magnetic resonance imaging
Received 13 Jan 2017, Accepted 6 Apr 2017
付立平,E-mail:gzbmr_000@163.com
2017-01-13
2017-04-06
R445.2;R711.32
A
10.12015/issn.1674-8034.2017.05.008
赵宏伟, 翟泽清, 付立平, 等. DWI在宫腔积脓和宫腔积液鉴别诊断中的价值.磁共振成像, 2017, 8(5): 359-362.
