冠脉搭桥全原位动脉桥术式探索
2017-09-06张小宁刘英超
张小宁 刘英超
基础研究
冠脉搭桥全原位动脉桥术式探索
张小宁 刘英超
科研项目:湖南省卫生厅科研基金课题(项目编号:2014C0096)
目的 采用猪进行不停跳原位动脉桥冠脉搭桥(CABG)技术训练并探索几种原位动脉桥CABG的手术方法。方法 采用体重60~70 kg的猪6只,分为3组,每组2只,在全麻不停跳下行CABG。A组分别取左、右乳内动脉(LIMA、RIMA),胃网膜右动脉(RGEA)行 LIMA-旋支(LCX)端侧吻合,RIMA-前降支(LAD)端侧吻合,RGEA-右冠(RCA)端侧吻合。B组分别取LIMA、RIMA,行LIMA-LCX侧侧吻合,再与LAD端侧吻合,RIMA-RCA端侧吻合。C组分别取LIMA、RGEA,行LIMA-LCX侧侧吻合,再与LAD端侧吻合,RGEA-RCA端侧吻合。结果 手术顺利,动脉桥血流通畅,成功建立了三种全原位动脉桥CABG术式。结论 三种全原位CABG方法均是可行的术式。行LIMA-LCX侧侧吻合后再与LAD端侧吻合,RIMA(或RGEA)-RCA端侧吻合是作者创立的全原位动脉桥CABG术式。
冠脉搭桥; 原位动脉; 左乳内动脉; 右乳内动脉; 胃网膜右动脉
回顾性研究显示,冠脉搭桥(CABG)使用双侧乳内动脉比使用单侧乳内动脉似乎能茯得更好的生存率[1]。原位左、右乳内动脉(LIMA、RIMA)10年通畅率在90%以上[2],原位骨骼肌化胃网膜右动脉桥(RGEA)4年累积通畅率为86.4%[3],原位动脉桥通畅率显著高于桡动脉桥和大隐静脉桥,取得了很好的临床效果。所以,采用原位动脉桥是临床冠脉搭桥的一个重要发展方向。采用猪进行CABG技术训练和评估CABG新技术是一种有效方法[4]。本研究采用猪进行不停跳CABG技术训练,并探索三种全原位动脉桥的手术方法。
1 材料与方法
1.1 材料 选用体重60~70 kg雄性黑毛土猪6只,分为3组,每种术式2只。戊巴比妥钠,国药集团化学试剂有限公司;氯胺酮,江苏省恒瑞股份有限公司。
1.2 麻醉 氯胺酮8 mg/kg肌注,4%戊巴比妥钠3 mg/kg静脉注射,行气管切开,动物呼吸机辅助呼吸。
1.3 分组及手术方法 所有实验动物仰卧位,取胸部正中切口,正中锯开胸骨,严格止血后,骨骼化取左、右乳内动脉(LIMA、RIMA)。获取 LIMA、RIMA时,上至第1肋间,下至第6肋间的肌膈动脉和腹壁上动脉分叉处。获取胃网膜右动脉(RGEA)时,将胸部正中切口由胸骨下角向下延伸8 cm,显露胃体,参考文献[5]报道的方法获取RGEA(图1)。各种CABG分组及术式方法如下:A组,分别取LIMA、RIMA,再将手术切口延伸到腹部,取RGEA,行LIMA-LCX端侧吻合,RIMA-LAD端侧吻合,RGEA-RCA端侧吻合。B组,分别取LIMA、RIMA,先将LIMA-LCX侧侧吻合,再与LAD端侧吻合,RIMA-RCA端侧吻合(图2)。C组,取LIMA,再将手术切口延伸到腹部,取RGEA,行LIMA-LCX侧侧吻合,再与LAD端侧吻合,RGEA-RCA端侧吻合。
1.4 术后观察 采用勒通试验法观察动脉桥血流通畅情况。按照血液通畅状况的不同,将勒通试验结果分为5个级别来判定:“+++”为通畅优良,饱满,色鲜红,可见血管搏动;“++”为通畅良好,血管饱满,色鲜红,血管搏动不明显;“+”为通畅好,血管较饱满,用显微镊夹持时从凹陷恢复到饱满过程较缓慢(3~5 s);“±”为通畅稍差,用显微镊夹持时凹陷处明显,恢复过程慢(5 s以上);“-”为通畅差,接近堵塞,血流近于停滞状态。
2 结果
手术顺利。通过勒通试验,各动脉桥血管术后通畅结果均达到“++”至“+++”,动脉桥血流通畅,成功建立了三种全原位动脉桥CABG术式。术后处死实验动物。
3 讨论
RIMA 10年总通畅率是90%,10年RIMA与旋支、右冠状动脉、后降支通畅率分别是91%、84%、86%,原位RIMA与游离RIMA 10年通畅率相似(89%比91%),10年RIMA和LIMA吻合到左前降支的通畅率分别是95%和96%,RIMA与LIMA远期通畅率相当,都显著高于桡动脉桥和大隐静脉桥,使用双侧乳内动脉CABG取得了很好的临床效果,并且不增加胸部损伤并发症,推介选择合适的患者应用[2,6-8]。在4个对比性研究中,骨骼化乳内动脉通畅率与带蒂乳内动脉通畅率相比较,骨骼化乳内动脉通畅率在两个对比性研究中更高,而且骨骼化乳内动脉可以减轻胸骨的损伤、感染,这一重要的发现促使临床CABG中更多地使用骨骼化乳内动脉技术[8,9]。我们在德国卡尔斯鲁厄心脏中心(Klinik Für Herzchirurgie Karlsruhe Gmbh) 访问时见到该中心所有CABG都使用骨骼化乳内动脉技术,所以在本研究中,各组均骨骼化获取双侧乳内动脉。
本研究A组采用全原位动脉桥,行LIMA-LCX端侧吻合,RIMA-LAD端侧吻合,RGEA-RCA端侧吻合(如图1)。Nishida等[10]对采用骨骼化双侧乳内动脉、RGEA全原位动脉桥进行了详细的临床应用研究,认为这一术式减少了手术风险、早期桥血管通畅率高、长期效果优秀。Suma等[11]重新研究124例患者远期(5~17年)通畅率,LIMA通畅率为96%(114/119)、RGEA 通畅率为 87%(108/124)、大隐静脉通畅率为68%(67/98)。20年的经验表明,在CABG中RGEA是安全、有效的动脉桥。分组分析表明,使用双侧乳内动脉桥合并使用RGEA 10年、20年的生存率分别是98.9%、68.9%,而使用双侧乳内动脉桥合并使用大隐静脉10年、20年的生存率分别是87.2%、50.3%,双侧乳内动脉桥合并使用RGEA具有更高的远期生存率,RGEA作为第三条动脉桥吻合到右冠状动脉可以提高远期生存率[12]。A组这一术式充分考虑原位动脉桥远期优秀的通畅率,但使用RGEA手术创伤大,有术后出现膈疝的报道[13],且术后胃癌发病率增加[14]。
作者在德国卡尔斯鲁厄心脏中心访问时,看到该中心在CABG术中,LIMA先与旋支侧侧吻合后再与LAD端侧吻合,但仍取大隐静脉与右冠吻合。作者在这一观察的启发下,基于RIMA良好的远期临床效果,在本研究中B组分别取LIMA、RIMA,采取先将LIMA-LCX侧侧吻合,再与LAD端侧吻合,RIMA-RCA端侧吻合的CABG术式(见图2)。A组同样采用了全原位动脉桥,而减少使用RGEA,从而也减少了使用RGEA带来的手术创伤和并发症。同时我们也基于使用RGEA安全有效的良好临床效果,建立了C组行LIMA-LCX侧侧吻合,再与LAD端侧吻合,RGEA-RCA端侧吻合的CABG术式。C组与A组对比,仅采用单侧乳内动脉即达到全原位动脉桥的目的。但我们未查到德国卡尔斯鲁厄心脏中心CABG术中LIMA先与旋支侧侧吻合后再与LAD端侧吻合,但仍取大隐静脉与右冠吻合这一术式的临床应用效果报道。我们探索建立的B组和C组两种CABG术式还需要大样本动物实验及临床试验加以验证。
CABG临床应用以来,对其各种术式进行了大量的基础和临床研究,原位动脉桥良好的临床效果得到肯定。动脉血管的内膜和外膜包绕着大量神经纤维,这些神经纤维通过分泌内分泌物质调节动脉血管的舒缩、抑制动脉血管内血栓形成和血管内膜增生。原位动脉桥之所以具有很好的远期通畅率,我们推测与原位动脉桥保持了血管的神经支配有关。本研究用黑毛土猪进行CABG训练,有益于提升个人手术技能,并创建了2种新的CABG术式。这两种CABG术式有各自的优点,在临床应用过程中可依据患者的病情灵活选用,期待取得更好的临床应用效果。
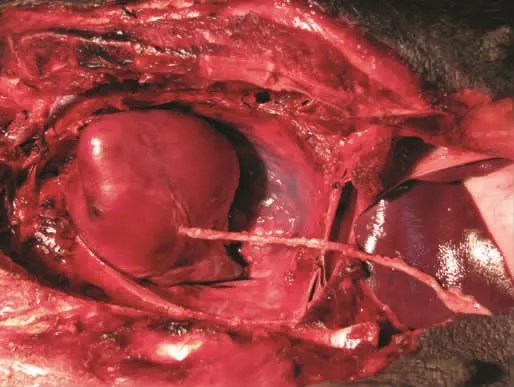
图1 RGEA-RCA端侧吻合

图2 RIMA-RCA端侧吻合,LIMA-LCX侧侧吻合后再与LAD端侧吻合
[1]Taggart DP,D′Amico R,Altman DG.Effect of arterial revascularisation on survival:a systematic review of studies comparing bilateral and single internal mammary arteries. Lancet,2001,358:870-875.
[2]Tatoulis J,Buxton BF,Fuller JA.The right internal thoracic artery:the forgotten conduit——5766 patients and 991 angiograms.Ann Thorac Surg,2011,92:9-15.
[3]Suma H,Tanabe H,Yamada J,et al.Midterm results for use of the skeletonized gastroepiploic artery graft in coronary artery bypass.Circ J,2007,71:1503-1505.
[4]Schachner T,Bonaros N,Ruttmann E,et al.Training models for coronary surgery.Heart Surg Forum,2007,10:E248-250.
[5]Formica F,Ferro O,Greco P,et al.Long-term follow-up of total arterial myocardial revascularization using exclusively pedicle bilateral internal thoracic artery and right gastroepiploic artery.Eur J Cardiothorac Surg,2004,26:1141-1148.
[6]Baradi A,Milsom PF,Merry AF,et al.Are two internal thoracic artery grafts as safe as one? Experience from Green Lane Hospital.N Z Med J,2012,125:36-41.
[7]来永强,黄方炯,杨禁非,等.双侧乳内动脉在冠状动脉搭桥中的应用.中华医学杂志,2002,82:1454-1456.
[8]张小宁,刘英超.冠脉旁路移植术中动脉桥的通畅率及基础研究进展.中国心血管病研究,2013,11:387-389.
[9]Ali E,Saso S,Ashrafian H,et al.Does a skeletonized or pedicled left internal thoracic artery give the best graft patency?Interact Cardiovasc Thorac Surg,2010,10:97-104.
[10]Nishida H,Tomizawa Y,Endo M,et al.Cornary artery bypass with only in situ bilateral internal thoracic arteries and right gastroepiploic artery.Circulation,2001,104:I76-180.
[11]Suma H,Tanabe H,Takahashi A,et al.Twenty years experience with the gastroepiploic artery graft for CABG.Circulation,2007,116:I188-1191.
[12]Glineur D,D′hoore W,Price J,et al.Survival benefit of multiple arterial grafting in a 25-year single-institutional experience:the importance of the third arterial graft.Eur J Cardiothorac Surg,2012,42:284-290.
[13]Takiuchi H,Totsugawa T,Tamaki T,et al.Intrapericardial di-aphragmatic hernia after coronary artery bypass grafting using the right gastroepiploic artery graft:report of a case.Ann Thorac Cardiovasc Surg,2011,17:624-627.
[14]Konishi Y,Suzuki K,Wada H,et al.How do we manage the gastrectomyforgastric canceraftercoronary arterybypass grafting using the right gastroepiploic artery?Report of two cases and a review of the literature.World J Surg Oncol,2007,17:54.
Study of coronary artery bypass grafting with only in situ arteries
ZHANG Xiao-ning*,LIU Ying-chao.*Department of Cardiothoracic Surgery,Hunan Zhuzhou Kind Cardiovascular Disease Hospital,Zhuzhou 412000,China
ZHANG Xiao-ning,E-mail:xiaoningzhang@msn.com
ObjectiveCoronary artery bypass grafting(CABG)with in situ artery long-term patency rate is high.This research adopts the pigs to do CABG with off-pump,CABG technique training and exploration of several in situ artery operation methods.MethodsThe 6 pigs,weight of 60-70 kg,divided into 3 groups,2 of each group,have been CABG with off-pump in general anesthesia:group A,The both internal mammary arteries(IMAs)and right gastroepiploic artery(RGEA)were harvested.Left internal mammary artery(LIMA)-left circumflex artery(LCX)end to side anastomosis.Right internal mammary artery(RIMA)-left anterior descending artery(LAD)end to side anastomosis;RGEA-right coronary artery(RCA)was end to side anastomosed.Group B,the IMAs were harvested,LIMA-LCX side-to-side anastomosis,and then to LAD end to side anastomosis;RIMARCA was end to side anastomosed.Group C,the LIMA and RGEA were harvested,LIMA and LCX side-to-side anastomosis,and then to LAD end to side anastomosis;RGEA-RCA was end to side anastomosed.ResultsSuccessfully established three kinds of in-situ arteries CABG surgery,the grafts are patency,then put to death the pigs.ConclusionCABG with all in situ Arteries is feasible.The LIMA and LCX side-to-side anastomosis,then to anterior descending branch end to side anastomosis.The RIMA(or RGEA)-RCA was end to side anastomosed are new feasible and the author created all in situ arteries CABG types.
Coronary artery bypass grafting(CABG); In situ artery; Left internal mammary artery(LIMA); Right internal mammary artery(RIMA); Right gastroepiploic artery(RGEA)
412000 湖南省株洲市,湖南株洲恺德心血管病医院心胸外科(张小宁),麻醉科(刘英超)
张小宁,E-mail:xiaoningzhang@msn.com
10.3969/j.issn.1672-5301.2017.02.024
Q95-33;R654.2
A
1672-5301(2017)02-0183-04
2016-08-06)
