Changing trends and in fluencing factors of the quality of life of chemotherapy patients with breast cancer*
2017-07-05ZhongPingAiXioLnGoJinFengLiJinRongZhouYouFengWu
Zhong-Ping Ai,Xio-Ln Go,Jin-Feng Li,Jin-Rong Zhou,You-Feng Wu
aIntensive Care Unit,The Af fi liated Hospital of Southwest Medical University,Luzhou,Sichuan 646000,China
bDepartment of Emergency,The Af fi liated Hospital of Southwest Medical University,Luzhou,Sichuan 646000,China
cSchool of Nursing,Chongqing Medical University,Chongqing 400016,China
dDepartment of Endocrine Surgery,The First Af fi liated Hospital of Chongqing Medical University,Chongqing 400016,China
Changing trends and in fluencing factors of the quality of life of chemotherapy patients with breast cancer*
Zhong-Ping Aia,*,Xiao-Lan Gaoa,Jin-Feng Lib,Jian-Rong Zhouc,You-Feng Wud
aIntensive Care Unit,The Af fi liated Hospital of Southwest Medical University,Luzhou,Sichuan 646000,China
bDepartment of Emergency,The Af fi liated Hospital of Southwest Medical University,Luzhou,Sichuan 646000,China
cSchool of Nursing,Chongqing Medical University,Chongqing 400016,China
dDepartment of Endocrine Surgery,The First Af fi liated Hospital of Chongqing Medical University,Chongqing 400016,China
a r t i c l e i n f o
Article history:
Breast cancer
Chemotherapy
Quality of life
Changing trajectory
In fluencing factor
Objective:To understand the changing trajectory of quality of life(QOL)during the treatment courses of breast cancer patients during chemotherapy and to investigate the factors in each treatment course that affect QOL.
Methods:The M.D.Anderson Symptom Inventory Scale,the Hospital Anxiety and Depression Scale (HADS),and the Functional Assessment of Cancer Therapy-Breast(FACT-B)scale were used to perform a survey on 174 breast cancer patients who received the TAC(docetaxel,Adriamycin,and cyclophosphamide)chemotherapy regimen before postoperative chemotherapy and 5e7 days after each chemotherapy course.
Results:The QOL scores of the breast cancer patients were the lowest before the postoperative chemotherapy(81.2±19.6)and the highest after the second chemotherapy course(94.5±14.4).After the fourth and fi fth chemotherapy courses,the scores were much lower again,with values of 82.7±13.9 and 82.6± 13.1,respectively.The scores improved again after the sixth chemotherapy course (93.9±18.7).Furthermore,each treatment course had different related symptoms that affected the QOL of the patients.
Conclusions:More attention should be paid to the changing trajectory of QOL of patients in alltreatment courses and to the in fluence of treatment-related symptoms on the QOL of patients;moreover,interventions should be adopted by medical care personnel to increase QOL in cancer patients.
©2017 Shanxi Medical Periodical Press.Publishing services by Elsevier B.V.This is an open access article under the CC BY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
1.Introduction
Currently,quality of life(QOL)assessment is considered the most sensitive and powerful indicator of breast cancer outcomes. Studies on QOL can help health care and related personnel better understand the demands of patients;in addition,they can help guide medical decision making and increase treatment effects.1Breast cancer has a high disease incidence,a long survival time, and special lesion sites;therefore,breast cancer patients not only face the fear of cancer recurrence and all types of treatment side effects after surgery,but they also face a damaged body;these factors severely affect the QOL of breast cancer patients.Currently, there is no domestic or foreign study targeting the changing trajectory of QOL of breast cancer patients during the period of chemotherapy.This study described the changing trajectory of the QOL of breast cancer patients during chemotherapy and investigated the relevant factors in each treatment course that in fluenced the QOL of patients.This study aimed to provide a theoreticalbasis for clinical health care personnel to develop overall nursing care plans for breast cancer patients.
2.Subjects and methods
2.1.Surveyed subjects
A total of 194 breast cancer patients who were pathologically diagnosed in the Department of Endocrine Surgery and the Department of Oncology of the First Af fi liated Hospital ofChongqing University and the Department of General Surgery and the Department of Oncology of the Af fi liated Hospital of Luzhou Medical College between September 2013 and February 2014 were selected using the convenience sampling method.The inclusion criteria were as follows:females who were older than 18 years of age,had an elementary school and above educational level,were fi rst diagnosed with unilateralbreast cancer,had received surgical treatment and planned to receive the TAC(docetaxel,Adriamycin, and cyclophosphamide)chemotherapy regimen,received and signed informed consent for this study,and could accurately complete the surveys.The exclusion criteria were as follows:patients who died or terminated treatmentfor various reasons during the treatment process,did not want to participate in or continuously receive this survey,used other treatment methods or drugs for various reasons,had chronic sleep disorders,chronic fatigue syndrome,unstable heart,lung,or neuromuscular diseases,diabetes mellitus,sleep apnea syndromes,chronic diseases treated with steroids,chronic gastrointestinal diseases,or worked night shifts.
2.2.Survey tools
2.2.1.General information questionnaire
A homemade general information questionnaire was used to collect sociodemographic and disease information including age, marital status,educational level,medical insurance status,and surgicalmethods.
2.2.2.M.D.Anderson Symptom Inventory2
This survey was composed of2 parts.The fi rst partcontained 13 items to measure the severity and degrees of pain,fatigue(tiredness),nausea,disturbed sleep,distress,shortness of breath,problems with remembering things,lack of appetite,drowsiness (sleepiness),dry mouth,sadness,vomiting,and numbness.Zero points were given if the symptom was not present;higher scores represented more severe symptoms.The highest score was 10 points.The second part contained 10 items to measure how any relevant symptoms affected the patient's life.This study used the fi rst part of the scale to measure the relevant symptoms and adverse reactions of patients during chemotherapy.A study by Cleeland et al.2had previously con fi rmed that this scale included the majority of the discomfort symptoms of patients during the treatment period and after the treatment and that it could be used for symptom survey and clinicalresearch.
2.2.3.Hospital anxiety and depression scale(HADS)3
This scale included 2 parts:the anxiety subscale(HAD(a))and the depression subscale(HAD(d)).Each subscale contained 7 items. The sum of the measured scores of all items was the score of the subscale.When the measured score was higher,the symptoms of anxiety and depression were more severe.A study by Zheng et al.3denoted a score of 9 points as the diagnostic standard for anxiety and depression.
2.2.4.FACT-B Chinese version4
This scale was composed of 5 parts comprising 36 items that measured the physiological conditions,social/family conditions, emotional status,functional status,and speci fi c module of breast cancer patients.This scale has been applied extensively in China and has good reliability and validity.
2.3.Research methods
After 48 h of surgery,study subjects who met the inclusion criteria were recruited.After the purpose and signi fi cance of this study were described,the patients received and signed an informed consent form.General demographic information and disease information were collected.The patients fi lled out the surveys independently within 24 h of their fi rst postoperative chemotherapy course to obtain the baseline information.Afterwards,the scales were distributed during the remaining chemotherapy courses,and the patients were instructed to complete the surveys 5e7 days after being discharged from the hospital.The surveys were collected at the next chemotherapy course.
2.4.Statistical analysis
SPSS 17.0 statisticalsoftware was used for paralleldouble entry of the raw survey data to avoid errors during data entry.Measurement data are expressed as the mean±standard deviation (M±SD).The QOL level in each treatment course was analyzed using repeated measures analysis of variance.The in fluencing factors of QOL in each treatment course were analyzed using multiple stepwise regression analysis.P<0.05 was considered as having statisticalsigni fi cance.
3.Results
3.1.General information(Table 1)
The general demographic information showed that the study subjects ranged in age from 25 to 68 years,with a mean age of 48.1±7.3 years.There were 134 cases ofinvasive ductalcarcinoma, 18 cases of simple carcinoma,and 22 cases of invasive lobular carcinoma.There were 42 cases of mastectomy,104 cases of modi fi ed radical mastectomy,and 28 cases of axillary lymph node dissection.
3.2.Status and changing trend of QOL
3.2.1.The status and trend of QOL(Table 2 and Fig.1)
Table 2 and Fig.1 show thatthe totalQOL scores ofbreastcancer patients were the lowest before the postoperative chemotherapy and the highest at the second chemotherapy course.The scores then decreased after the fourth and fi fth chemotherapy courses, followed by a gradual improvement in score.
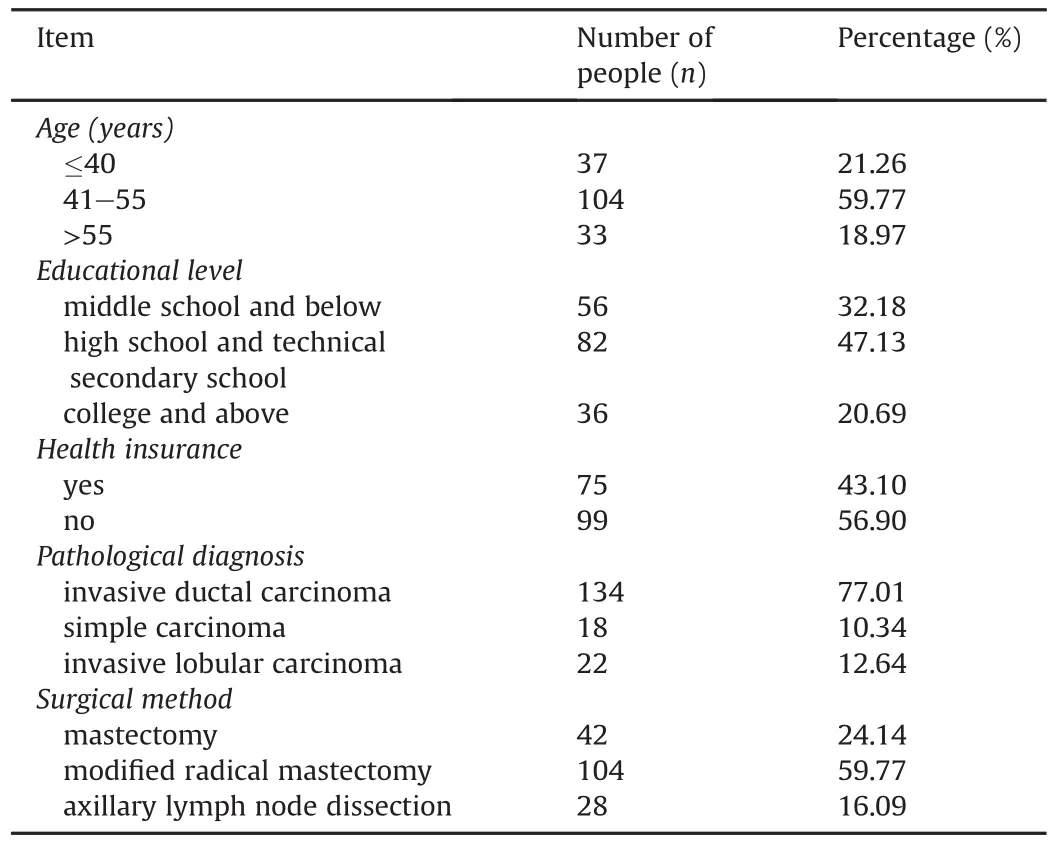
Table 1 Demographic and disease information of the study subjects(n¼174).

Table 2 QOL conditions during chemotherapy of breast cancer patients(M±SD).
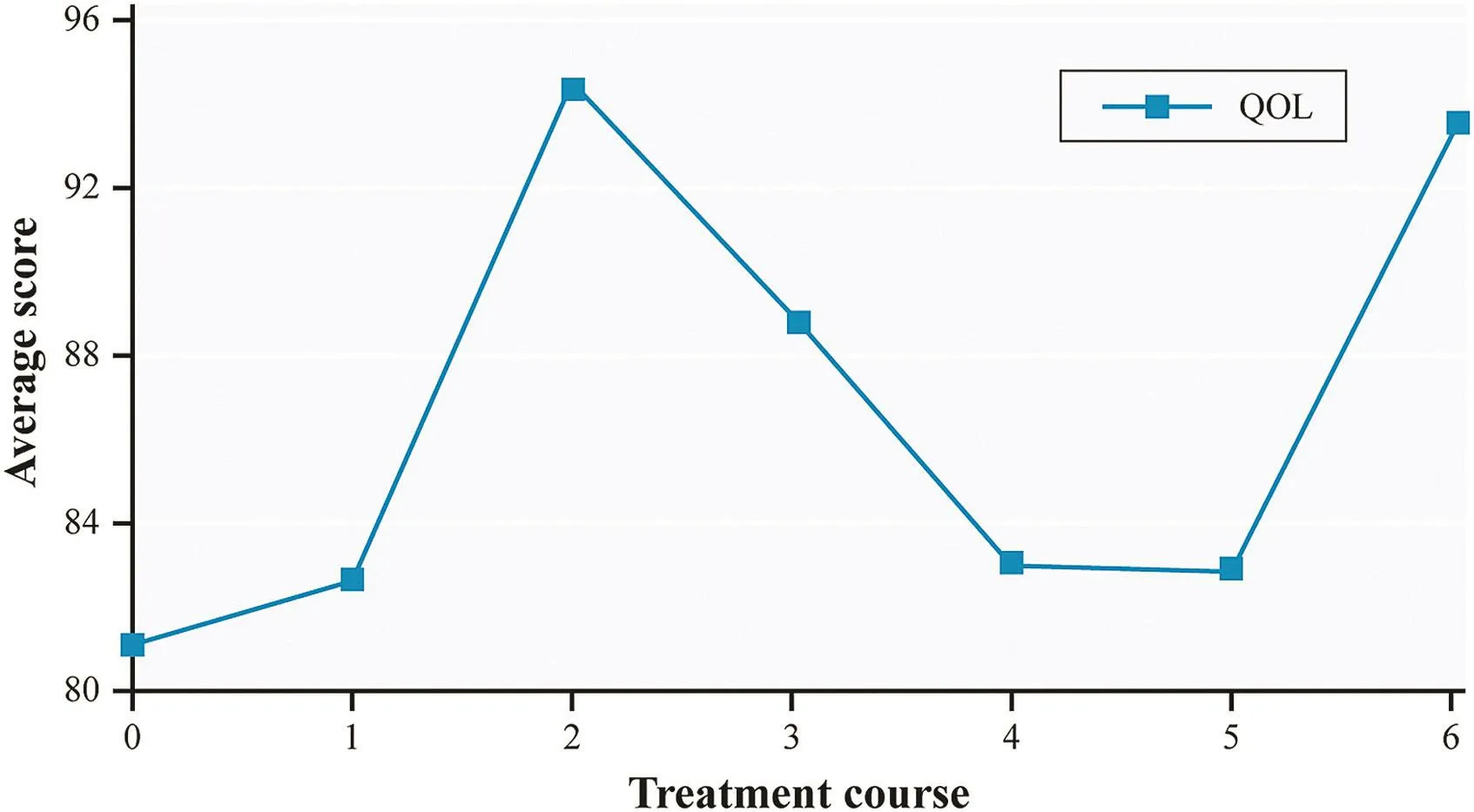
Fig.1.The changing trajectory of the total QOL scores of breast cancer patients for the treatment courses during the period of chemotherapy.Note:0:after surgery and before chemotherapy;1:after the fi rst chemotherapy course,etc.
3.2.2.Results of the pairwise comparison between total QOL scores during the period of chemotherapy
The sphericity test result ofthe repeated measures mean values of QOL showed P<0.05,indicating that correction should be performed in the test of within group effects.The corrected results reported F¼16.710 and P¼0.000,indicating that the time factor (treatment course)had statisticalsigni fi cance.
The pairwise comparison results of the repeated measures analysis of variance in Table 3 and the trend in Fig.1 show that the total QOL score of breast cancer patients was the lowest before postoperative chemotherapy;QOL improved after the fi rst chemotherapy course to a level that was signi fi cantly higher than that before postoperative chemotherapy(P<0.05).The QOL of the patients after the second chemotherapy course was the highest throughout the entire chemotherapy process and was signi fi cantly higher than that before postoperative chemotherapy(P<0.05). After the third chemotherapy course,the QOL of the patients decreased and was signi fi cantly lower than that after the second chemotherapy course but was still signi fi cantly higher than that before postoperative chemotherapy(P<0.05).After the fourth and fi fth chemotherapy courses,the QOL of the patients signi fi cantly decreased again,followed by signi fi cant improvement.After the sixth chemotherapy course,QOL improved again and was signi ficantly higher than that before chemotherapy.Fig.1 displays the changing trend of QOL in the treatment courses of patients during the chemotherapy period.
3.3.Analysis of in fluencing factors of QOL(Table 4)
Depression,pain,and poorappetite were associated with the total QOLscoresbefore postoperative chemotherapy(r¼0.913,r2¼0.834, F¼292.404,P¼0.000).After the fi rst chemotherapy course,problems with remembering things were associated with QOL(r¼0.974, r2¼0.949,F¼6.012,P¼0.000).After the second chemotherapy course,numbness,pain,disturbed sleep,and sadness were associated with QOL(r¼0.896,r2¼0.803,F¼76.130,P¼0.000).After the third chemotherapy course,depression,shortness ofbreath,nausea, anxiety,drowsy,pain,numbness,distressed,vomiting,and sadness were associated with the total QOL score(r¼0.912,r2¼0.832, F¼85.847,P¼0.000).After the fourth chemotherapy course, shortness ofbreath,anxiety,and problems with remembering things were associated with the total QOL score(r¼0.839,r2¼0.703, F¼67.503,P¼0.000).After the fi fth chemotherapy course,numbness,pain,disturbed sleep,and depression were associated with the totalQOL score(r¼0.896,r2¼0.793,F¼76.130,P¼0.000).Afterthe sixth chemotherapy course,anxiety,numbness,disturbed sleep,and being distressed were associated with the totalQOL score(r¼0.938, r2¼0.879,F¼47.950,P¼0.000).
4.Discussion
With the rapid developmentofcurrentmedicalpractice,humans will no longer be satis fi ed with merely extending survival time; instead,they will begin to focus on different aspects of QOL including physiology,psychology,and socialadaptation.Therefore, current commonly used traditional medical evaluation indicators such as the prevalence rate and cure rate can no longer comprehensively re flect the multiple hazards of diseases to people;they cannottruly re flectpatients'disease experience and comprehensive responses to treatment;they cannot comprehensively evaluate the ef fi cacy ofintervention measures;and they cannot satisfy the new demands ofpatients and society toward health.To comprehensively evaluate the in fluences of diseases and treatment on the multiple aspects of patients including physiology,psychology,and social adaptation,the medicalcommunity proposes the concept of QOL.
Studies have shown that5,6chemotherapy has a very signi fi cant negative in fluence on the QOL of cancer patients.After chemotherapy,patients have a lower general well-being,more physical discomfort symptoms,reduced motility,increased sleep,sexual dysfunction,and reduced social participation and work abilities compared to before chemotherapy.5Several studies have con fi rmed that breast cancer patients usually have anxiety, depression,7e9nervousness,uncertainty,10and reduced body and social functions.11These all in fluence the con fi dence of patients to adequately face the disease and allaspects of QOL.7e9,11
This study used scales to perform a survey and analysis on the QOL of breast cancer patients during the period of chemotherapy; these results are discussed below.
4.1.Analysis of the general information of breast cancer patients
The generalinformation showed thatthe study subjects ranged in age from25 to 68 years,witha mean age of48.1±7.3 years.Regarding surgicalmethods,104 patients received a modi fi ed radicalmastectomy,which accounted for approximately 60%of the totalpatients. Regarding education level,82 patients had a high schoolor technical secondary school education level,which accounted for approximately 47%ofthe totalpatients.A totalof20 patients were excluded from this study;the main reasons were invalid questionnaires, dropout in the middle ofthe study,and loss to follow-up.
4.2.Status and changing trajectory of the QOL of breast cancer patients during the chemotherapy period
The period before postoperative chemotherapy is the initialstage ofdisease diagnosis and treatment.Although the toxic side effects of chemotherapy are notyetpresent,patients endure the double threat ofdamaging life and femininity.After patients receive a mastectomy,their mutilated breast and changes in their fi gure signi fi cantly influence their body image and social consciousness12and damage their self-esteem;therefore,patients have anxiety and depression and are prone to have poormoods and irritability.Therefore,patients atthis stage had poorer QOL scores.Overtime,the patients gradually accepted thatthey were breastcancer patients,and their bodies also gradually recovered from the surgery.Therefore,after the second surgery,when the toxic side effects ofchemotherapy were not very severe,the QOL scores of the patients were better.However,the toxicity ofthe chemotherapeutic agents then began to accumulate in the body.After the fourth and fi fth chemotherapy courses,the patients mistakenly believed that the abruptly increased and aggravated toxic side effectswere signals ofdisease aggravation;thus,they became pessimistic and disappointed.Therefore,the QOL of the patients at this stage decreased.After the sixth and fi nal chemotherapy course,the patients viewed the end of treatment as curing the disease,and they began to face the future positively.Therefore, their QOL scores increased once again.

Table 3 Pairwise comparison of repeated measures analysis of variance of QOL levels.
4.3.In fluencing factors of the QOL of breast cancer patients during the chemotherapy period
Body recovery condition,surgical discomfort symptoms,toxic side effects of chemotherapy,and psychological status of patients all continuously change with time.The results of the multiple stepwise regression analysis in this study showed that each treatment course had different related symptoms that affected the QOL of the patients(Table 4).Pain in particular is a bad experience for cancer patients.Patients with persistent or aggravated pain are prone to be pessimistic and disappointed,which signi fi cantly damages their QOL.13With the application of chemotherapy drugs and the increase oftreatment courses,a variety oftoxic side effects of chemotherapy appear successively and gradually aggravate the patient's conditions,affecting QOL.Ma et al.14performed surveys on 200 breastcancer patients and showed thatsymptoms including a lack of energy,worry,pain,dif fi culty in sleeping,constipation, irritability,dry mouth,sweating,numbness/tingling in hands/feet, nausea,lack ofappetite,and shortness ofbreath together explained 79%of the variation in the overall QOL of breast cancer patients.
Disturbed sleep is a common symptom ofbreastcancer patients. A survey by Huang et al.15showed that 60.1%of breast cancer patients had different degrees and different types of insomnia.A study by Ma etal.14showed that73.5%ofbreastcancer patients had dif fi culty sleeping.Dif fi culty sleeping was caused by pain,worry about diseases and medical expenses,not being adapted to the hospitalenvironment,and other psychologicalfactors.16Ma et al.14performed surveys on 200 breast cancer patients and found that the incidence ofnervousness and worry were both higher than 80%,suggesting thatbreastcancer patients have psychologicalproblems including anxiety,depression,worry,and sorrow.The psychological problems of breast cancer patients were primarily associated with the following factors:(1)patients have low levels ofunderstanding of the disease;(2)patients worry about prognosis and fear death; and(3)patients worry about losing femininity because of the loss oftheir breasts.This fear becomes more obvious with the progress ofsocialcivilization:(4)patients worry about the loss ofsocialand family status because ofthe loss ofwork and economic income;(5) patients worry about losing family and friends;(6)patients experience discomfort caused by the radiotherapy and chemotherapy; and(7)patients worry about treatment expenses.These psychological problems can both reduce treatment compliance,thus in fluencing treatment effects,and produce neuroendocrine regulation disorders and induce immune system suppression and aggravation of systemic conditions to in fluence prognosis and survival.17,18The survey by Ma et al.14showed that 44%of patients had nausea and 60%of patients had a lack of appetite.These symptoms cause patients to lose patience and con fi dence regarding the treatment and are considered signals of disease aggravation, thus increase the psychological burden and affect the QOL of patients.
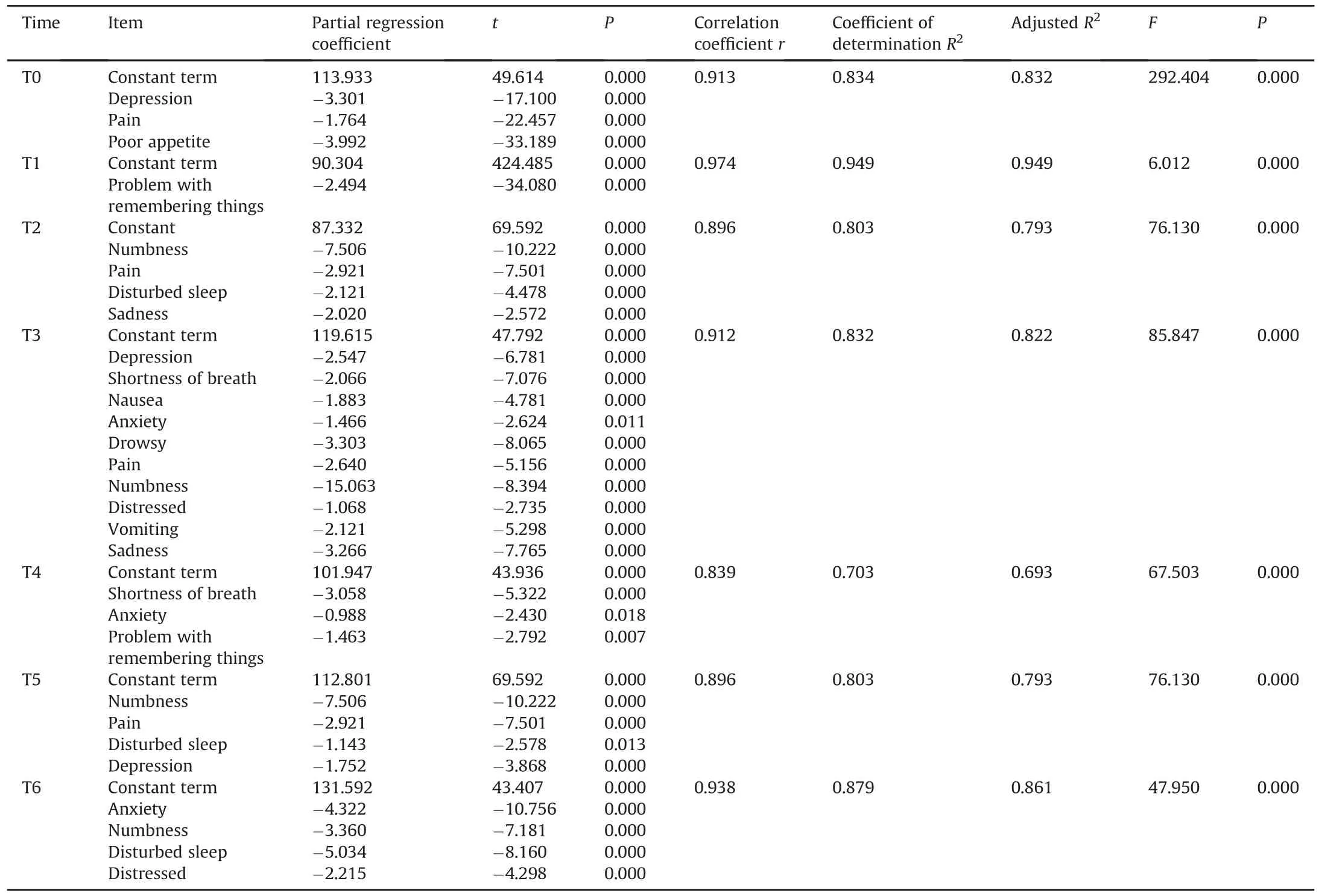
Table 4 Multiple stepwise regression analysis of in fluencing factors of the total QOL scores before postoperative chemotherapy.
Many studies have shown thatmaximally controlling symptoms is a key step in improving the QOL of patients.19The results in this study also suggested that the control of relevant symptoms was particularly important in increasing the QOL of breast cancer patients.In addition,the chemotherapy drugs and ancillary drugs used for treatment were very expensive,and the patients required several treatment courses of chemotherapy,which created a heavier economic burden on the patients.Some patients experience anxiety and depression because they cannot afford the medical expenses.Therefore,psychological counseling should be improved for breast cancer patients to relieve their psychological pressure.Pain is a very obvious adverse experience for cancer patients.Cancer patients who already bear enormous psychological pressure willconsider persistent pain or aggravated pain a signalof disease aggravation;therefore,they are more prone to experience pessimism and disappointment,which signi fi cantly damage their QOL.20Consequently,for breast cancer patients who experience pain,analgesic therapy is one of the most important measures to increase their overall QOL.
4.4.Nursing intervention strategies
To target the above in fluencing factors of the QOL of patients during the chemotherapy period,nursing personnel can adopt targeted intervention measures in clinicalpractices to increase the QOL of patients.Speci fi cally,before postoperative chemotherapy, after the fi rst chemotherapy course,and after the fourth and fi fth chemotherapy courses when patients have a poorer QOL,medical care personnel should provide special attention to patients and adopt corresponding intervention measures to increase the QOL of patients.At the early stage of disease diagnosis,medical care personnel should provide psychological interventions and psychological counseling for patients,provide social support,offer health education,help patients to correctly understand breastcancer and the progression and prognosis ofbreast cancer,and help patients establish con fi dence to conquer the disease.Before chemotherapy,Schwartz et al.21suggest that doctors conduct indepth conversations with patients on all critical issues such as the severity of the disease and the predicted life expectancy to reduce the anxiety and depression of the patients.
Severalintervention studies have already con fi rmed that intervention measures including supportive psychological care,6health education,cognitive behavioral intervention,supportive intervention,and relaxation training22have positive effects on improving the QOL of patients.A study by Rustøen et al.23showed that hope was an importantcomponentfor improving the QOL ofpatients;by contrast,hopeless was associated with a reduction in physiological health,psychological health,and QOL.Therefore,increasing the QOL of patients allows them to face the disease and maintain a positive mentality;moreover,support from different individuals including psychotherapists,family members,and friends made in the hospital is essential during this intervention process.
5.Conclusions
In summary,the QOL of breast cancer patients changed as treatment courses changed,and each treatment course had different symptoms that affected the QOL ofpatients.These results suggest that medical care personnel should focus more on the psychological and social aspects of patients before postoperative chemotherapy and after the fourth and fi fth chemotherapy courses, at which times the QOL conditions of patients were worse.Moreover,medicalcare personnel should actively take action to relieve all types of treatment-related symptoms that physically and mentally in fluence patients during this period to increase the overall QOL of patients.
Conflicts of interest
All contributing authors declare no con flicts of interest.
1.Liu Y,Yu SY.Survival prediction of patients with advanced cancer.Tumor. 2011;31:165e168(in Chinese).
2.Cleeland CS,Mendoza TR,Wang XS,et al.Assessing symptom distress in cancer patients:the M.D.Anderson Symptom Inventory.Cancer.2000;89:1634e1646.
3.Zheng LL,Wang YL,Li HC.Application of a hospital anxiety and depression scale in a general hospital:an analysis of reliability and.Shanghai Arch Psych. 2003;15:264e266(in Chinese).
4.Wan CH,Zhang DM,Tang XL.Introduction of a measurement scale of quality of life for patients with breast cancer:Chinese version of FACT-B.Bull Chin Canc. 2002;11:318e320(in Chinese).
5.Turgay AS,Khorshid L,Eser I.Effect of the fi rst chemotherapy course on the quality of life of cancer patients in Turkey.Cancer Nurs.2008;31:E19e E23.
6.Yang D.Supportive psychological intervention on breast cancer patients'psychological status and quality of life.Chin Nurs Res.2012;26:703e704(in Chinese).
7.Badger TA,Braden CJ,Mishel MH,Longman A.Depression burden,psychological adjustment,and quality of life in women with breast cancer:patterns over time.Res Nurs Health.2004;27:19e28.
8.Badger T,Segrin C,Dorros SM,Meek P,Lopez AM.Depression and anxiety in women with breast cancer and their partners.Nurs Res.2007;56:44e53.
9.Burgess C,Cornelius V,Love S,Graham J,Richards M,Ramirez A.Depression and anxiety in women with early breast cancer:fi ve year observational cohort study.BMJ.2005;330:702.
10.Sammarco A.Perceived social support,uncertainty,and quality of life of younger breast cancer survivors.Cancer Nurs.2001;24:212e219.
11.Engel J,Kerr J,Schlesinger-Raab A,Sauer H,H€olzel D.Quality of life following breast-conserving therapy or mastectomy:results of a 5-year prospective study.Breast J.2004;10:223e231.
12.Cui XF,Wang AY,Li FY.Changing tendency and in fluencing factors of anxiety and depression for patients with breast cancer during chemotherapy.JQiqihar Univ Med.2005;26:1352e1353(in Chinese).
13.Zou JJ,Zheng Y,Cao CW,et al.Effects of Depression and Pain on Quality of Life in Cancer Patients:a Survey Analysis.vol.26.Acad J Second Military Med Univ; 2005:928e930(in Chinese).
14.Ma L,Wang SP,Chung J.A survey on correlative symptoms and its in fluence on quality oflife in breast cancer patients.Chin JEvid-Based Med.2007;7:169e174 (in Chinese).
15.Huang LY.Causes of insomnia patients with breast cancer and nursing strategies.Heilongjiang Med J.2005;29:710e711(in Chinese).
16.Li JF.Investigation of quality of life of patients with breast cancer after operation and its in fluencing factors.Chin JPrac Nurs.2010;26:54e55(in Chinese).
17.Luo CM,Ren M,Zhao XB.Research progress on psychological status and psychological nursing of patients with breast cancer.Nanfang J Nurs.2004;11: 16e17(in Chinese).
18.Li HJ,Liu H,Zhang YQ,Jin J,Zhao YB.Effect of psychological rehabilitation for breast carcinoma.Chin J Clin Rehabil.2004;8:4818e4819(in Chinese).
19.Liu YW,Li XR,Chen YQ,et al.Analysis of in fluencing factors of quality of life of postoperative breast cancer patients.Chin J Breast Dis.2012;6:162e167(in Chinese).
20.Gao J,Jiang XY,Liu YY,Zhuang HZ.Investigation of quality of life of breast cancer patients who received breast conservative surgery and nursing intervention.J Fujian Med Univ.2007;41:348e350(in Chinese).
21.Schwarz R,Krauss O,H€ockel M,Meyer A,Zenger M,Hinz A.The course of anxiety and depression in patients with breast cancer and gynaecological cancer.Breast Care(Basel).2008;3:417e422.
22.Zhang J,Chen L,Wu ZH,et al.The effect of psychological intervention on level of hope and quality of life in the breast cancer patients.Chin JBehav Med Brain Sci.2010;19:341e343(in Chinese).
23.Rustøen T,Wiklund I.Hope in newly diagnosed patients with cancer.Cancer Nurs.2000;23:214e219.
How to cite this article:Ai Z-P,Gao X-L,Li J-F,et al.Changing trends and in fluencing factors of the quality of life of chemotherapy patients with breast cancer. Chin Nurs Res. 2017;4:18e23.http://dx.doi.org/10.1016/j.cnre.2017.03.006
18 June 2016
*This project was supported by a project of scienti fi c research of the Af fi liated Hospital of Luzhou Medical College(No.14039).
*Corresponding author.
E-mail address:407325659@qq.com(Z.-P.Ai).
Peer review under responsibility of Shanxi Medical Periodical Press.
http://dx.doi.org/10.1016/j.cnre.2017.03.006
2095-7718/©2017 ShanxiMedical PeriodicalPress.Publishing services by Elsevier B.V.This is an open access article under the CC BY-NC-ND license(http://creativecommons. org/licenses/by-nc-nd/4.0/).
Received in revised form 25 July 2016
Accepted 27 December 2016
Available online 15 April 2017
杂志排行

Frontiers of Nursing的其它文章
- Prevalence and associated factors of health problems among Indonesian farmers*
- Burnout and work-family con flict among nurses during the preparation for reevaluation of a grade A tertiary hospital
- Conversation with presence:A narrative inquiry into the learning experience of Chinese students studying nursing at Australian universities
- Comparative research on the prognostic ability of improved early warning and APACHE II evaluation for hospitalized patients in the emergency department*
- Training indicators and quantitative criteria for emergency nurse specialists*
- The application of the necessity-concerns framework in investigating adherence and beliefs about immunosuppressive medication among Chinese liver transplant recipients*