多层螺旋CT(MSCT)在肝癌经导管肝动脉化疗栓塞术(TACE)疗效分型、评估的应用价值研究
2017-06-05侯江平黄晓兵湖北省京山县人民医院放射科湖北荆门431800
侯江平,黄晓兵(湖北省京山县人民医院放射科,湖北 荆门 431800)
多层螺旋CT(MSCT)在肝癌经导管肝动脉化疗栓塞术(TACE)疗效分型、评估的应用价值研究
侯江平,黄晓兵
(湖北省京山县人民医院放射科,湖北 荆门 431800)
目的 研究于肝癌经导管肝动脉化疗栓塞手术(Transcatheter Arterial Chemoembolization,TACE)中应用多层螺旋CT(Multisliecs helieal CT,MSCT)对疗效分型和评估的价值。方法 选取采用TACE治疗80例肝癌患者临床资料进行分析,于手术前和手术后1个月均应用MSCT平扫与多期增强扫描,对治疗前后MSCT图像和手术后的碘油沉积状况予以对比分析,且按照MSCT图像分析TACE治疗后疗效分型和评估价值。结果 手术后1个月结节型肝癌MSCT扫描Ⅰ型碘油沉积所占比例76.67%比肿块型28.00%高,Ⅱ型碘油沉积所占比例20.00%比肿块型54.00%低(P<0.01);结节型肝癌者手术后完全缓解型所占比例80.00%比肿块型28.00%高;两者治疗有效概率对比差异无统计学意义(P<0.01)。结论 MSCT应用于肝癌TACE疗效分型和评估中的价值高,能够对手术疗效与预后作出客观评价,且指导患者下一步的治疗,促进患者预后改善,具一定临床推广及应用价值。
肝癌;多层螺旋CT;经导管肝动脉化疗栓塞术;疗效分型
肝癌为肝脏常见血供病变,具高发病率与死亡率等特点,临床一般采取手术切除,且TACE为临床公认的对不能手术直接切除肝癌的一种首选方法,但对手术后疗效情况如何科学评估一直是临床关注焦点;伴随CT技术不断发展,MSCT于手术前后通过平扫和增强扫描能够准确评估临床疗效[1-3]。为此,本研究对采用TACE治疗80例肝癌患者临床资料进行分析,旨在强化手术治疗效果,改善患者预后,且为临床疾病治疗提供借鉴,作如下报告。
1 资料与方法
1.1 临床资料 选取2014年8月~2016年8月湖北省京山县人民医院收治的选择TACE治疗80例肝癌患者临床资料予以分析,本研究对象提交的方案均通过医学伦理委员会批准,参与研究的人员均签署知情同意书,均通过临床与穿刺活检及影像学确诊,临床资料完整,均是单发病灶,将存在手术禁忌症与精神障碍者排除,且均符合肝癌临床相关诊断标准[4]。其中男女比例50∶30,年龄28~76岁,平均(50.54±2.10)岁,肝癌类型:30例结节型,50例肿块型。
1.2 研究方法 均选择TACE治疗,于手术前和手术后1个月进行MSCT检查,选择CT为美国Philips 128层 brilliance及MR为德国Siemens 1.5T magentom,具体操作:扫描范围为膈顶-肚脐,参数设置为1.15 mm螺距,5 mm层厚,先采取MSCT常规平扫方式,后予以多期增强式扫描,且触发点为腹腔的起始位置腹主动脉面,100 Hu触发阈值,分别对动静脉期与延时期进行扫描,待触发后5 s扫描动脉期,动脉期结束后24s进行门脉期扫描,门脉时结束后60 s予以岩石期扫描,扫描过程中对比剂为非离子型碘佛醇[泰科医疗器材国际贸易(上海)有限公司,JX20020104,50 mL:33.90 g],总量为1.20~1.50 mL/kg,经患者肘部置静脉留置针,型号为20GX/29 mm,利用团注方法,3~3.50 mL/s注射速率,检查结束后将数据予减薄处理(1 mm减薄层厚),并传至工作站予以血管造影、多平面重建等。
1.3 观察指标和评判标准[5]观察结节、肿块型肝癌患者手术后疗效分型和评估价值。评判标准:碘油沉积分型,瘤内碘油沉积无为Ⅳ型,碘油呈现斑块或者簇装沉积为Ⅲ型;存在碘油填充明显缺损区为Ⅱ型,碘油完全沉积,且边缘完整为Ⅰ型。参照世界卫生组织实性肿瘤疗效标准,将MSCT扫描和TACE治疗后效果分为进展型、暂时稳定型、部分与完全缓解型,肿瘤内的碘油沉积为Ⅳ型,范围≤10%,且有新生病灶出现为进展型;瘤内碘油沉积为Ⅲ型,未出现新生病灶(维持时间超过4周),且瘤内强化面积≥25%,肿块缩小范围<25%为暂时稳定型;瘤内碘油沉积为Ⅱ型,瘤内强化面积≤25%,且肿块缩小范围<75%为部分缓解型;瘤内碘油沉积为Ⅰ型,瘤内无强化,且肿块缩小范围>75%或者消失为完全缓解型,有效概率=(暂时稳定型+部分缓解型+完全缓解型)/总例数×100%。
1.4 统计学方法 数据借助SPSS22.0软件处理及分析,计数资料用“n,%”表示,组间比较采用χ2检验,P<0.05为差异有统计学意义。
2 结果
2.1 结节和肿块型肝癌MSCT扫描碘油沉积情况 手术后1个月结节型肝癌MSCT扫描Ⅰ型碘油沉积所占比较肿块型高,Ⅱ型碘油沉积所占比较肿块型低(P<0.01);两者Ⅲ、Ⅳ型碘油沉积所占比例对比差异均无统计学意义。见表1。
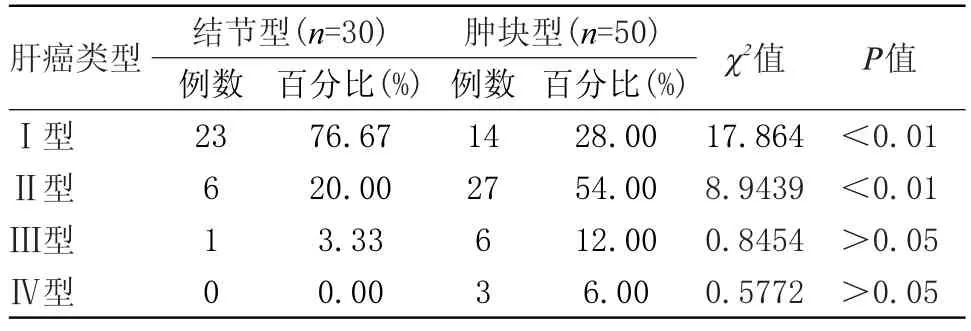
表1 结节和肿块型肝癌MSCT扫描碘油沉积情况(n)Table 1 Nodules and masses type liver cancer MSCT scanning iodine oil deposition(n)
2.2 结节和肿块型肝癌缓解情况 结节型肝癌者手术后完全缓解型所占比较肿块型高,部分缓解型所占比较肿块型低(P<0.01);两者治疗有效概率对比差异无统计学意义。见表2。

表2 结节和肿块型肝癌缓解情况(n)Table 2 Type nodules and masses ease of liver cancer(n)
3 讨论
肝癌属于临床常见肿瘤疾病,我国肝癌患病率较高,于全球肝癌中约占40%~45%,且此类疾病发病率呈不断上升趋势,对患者生命安全造成威胁,需积极采取有效治疗措施;TACE因具创伤小和疗效佳等特点得到临床普遍应用,但单次TACE效果欠佳,需多次手术,且进一步医治措施实施为基于对肿瘤活性准确判断[6-8]。伴随临床诊断技术不断发展,MSCT和磁共振成像为肝癌患者TACE治疗后随访常用方法,但临床对MSCT诊断价值仍存在争议[9-10]。为强化TACE临床疗效,本研究观察和分析手术治疗前后应用MSCT检查对疗效分型和评估的价值。本研究结果显示:手术后1个月结节和肿块型肝癌MSCT扫描Ⅲ、Ⅳ型碘油沉积所占比例及治疗有效概率比较差异均无统计学意义;结节型肝癌Ⅰ型碘油沉积所占比76.67%较肿块型28.00%高,Ⅱ型碘油沉积所占比较肿块型低;结节型肝癌者手术后完全缓解型所占比80.00%较肿块型28.00%高,部分缓解型所占比较肿块型低,和相关文献报道结果一致[11],提示:MSCT应用于肝癌TACE疗效分型和评估中具有较高价值,有利于对手术疗效及预后作出客观评价,可明确肝癌类型,促进病情缓解。肝癌TACE首次治疗后碘油沉积的类型、各型比例和肝癌类型密切相关,结节型肝癌无Ⅳ型碘油沉积,考虑肿瘤小和供血动脉少及通常不存在寄生动脉,便于手术操作;肿块型肝癌Ⅱ型碘油沉积较多,可能为肿瘤组织存在局部残留,需进行TACE二次治疗。此外,MSCT具扫描层薄、扫描快和图像后处理技术强大,能够对图像进行及时快速且多形式重组,将肿瘤形态、大小、瘤内碘油沉积及供血动脉清晰显示,便于精准测量;扫描中借助对比剂触发技术予以多期增强扫描,使临床疗效评估更科学、准确。关于MSCT应用于肝癌TACE治疗中和进一步治疗后对患者生活质量提高的影响,本研究考虑受样本例数、外部环境及时间等因素制约,需增加样本量、优化外部环境、延长时间等进行深入研究及做合理改善。
总结上文,临床于肝癌TACE治疗中应用MSCT对疗效分型和评估的价值高,能够明确疾病类型,有利于碘油沉积和病情缓解,是一种对手术疗效与预后作出客观评价的检查方法,对患者治疗起到指导性作用,可强化临床治疗效果,改善患者预后,临床推广及应用价值高。
[1] 郁义星,林晓珠,陈克敏,等.CT能谱成像在鉴别肝癌和局灶性结节增生中的价值[J].中华放射学杂志,2013,47(2):121-126.
[2] Sahar Darvish-Molla,Alia Al-Ebraheem,Michael J.Farquharson et al.The Identification and Differentiation of Secondary Colorectal Cancer in Human Liver TissueUsingX-rayFluorescence,CoherentScatter Spectroscopy,and Multivariate Analysis[J].Applied Spectroscopy:Society for Applied Spectroscopy,2014, 68(1):79-87.
[3] Stephany Y Tzeng,Luke J Higgins,Martin G Pomper,et al.Student award winner in the Ph.D.category for the 2013 society for biomaterials annual meeting and exposition,april 10-13, 2013,Boston,Massachusetts:biomaterial-mediated cancer-specific DNA delivery to liver cell cultures using synthetic poly (beta-amino ester)s[J].Journal of biomedical materials research,Part A,2013,101A(7):1837-1845.
[4] 沈珏,林小军,崔伯康,等.血必净注射液预处理对肝癌切除术后缺血/再灌注损伤及凝血功能紊乱的保护作用研究[J].中华危重病急救医学,2013,25(12):743-748.
[5] 于志海,成科,王海涛.奥沙利铂联合表柔比星介入治疗原发性肝癌的临床研究[J].中华全科医学,2016,14(2):326-327.
[6] 赵群,李勇,胡子龙,等.多层螺旋CT对胃癌术前分期及肿瘤最长径的评估价值[J].中华胃肠外科杂志,2015,18(3):227-231.
[7] Gulec SA,Pennington K,Wheeler J,et al.Yttrium-90 microsphere-selective internal radiation therapy with chemotherapy(Chemo-SIRT)forcolorectalcancer livermetastases:Aninvivodouble-arm-controlled phase II trial[J].American Journal of Clinical Oncology:Cancer Clinical Trials,2013,36(5):455-460.
[8] Vogl TJ,Freier V,Nour-Eldin NEA,et al.Magnetic resonance-guided laser-induced interstitial thermotherapy of breast cancer liver metastases and other noncolorectal cancer liver metastases:An analysis ofprognostic factorsfor long-termsurvivaland progression-free survival[J].Investigative radiology,2013,48(6):406-412.
[9] 张晓丹,王文红,李鹏,等.MSCT对直肠癌术后肠梗阻的诊断价值及临床意义[J].中华普通外科杂志,2015,30(1):27-30.
[10]Vogl TJ,Gruber-Rouh T,Eichler K,et al.Response to comment on"repetitive transarterial chemoembolization(TACE)of liver metastases from gastric cancer: Local control and survival results":Will there be clinical implications in the future?[J].European Journal of Radiology,2013,82(9):1592-1594.
[11]Chapiro Julius,Duran Rafael,Lin MingDe,et al.Early survival prediction after intra-arterial therapies:a 3D quantitative MRI assessment of tumour response after TACE or radioembolization of colorectal cancer metastases to the liver[J].European radiology,2015,25(7):1993-2003.
Value of Multislice Spiral CT(MSCT)in the Evaluation of Hepatocellular Carcinoma by TranscatheterArterial
Chemoembolization(TACE)
Hou Jiang-ping,Huang Xiao-bing
(Department of Radiology of Jingshan People’s Hospital,Jingmen,Hubei,431800,China)
Objective To study the value of multi-slice spiral CT(MSCT)in the curative effect classification and assessment of transcatheter arterial chemoembolization(TACE)for hepatocellular carcinoma.Methods The clinical data of 80 HCC patients who had
TACE were analyzed.MSCT plain scan and multi-phase enhanced scan were given to these patients before and one month after the surgery.The MSCT images before and after surgery,and the lipiodol deposition after surgery were comparatively analyzed,and value of TACE for the curative effect classfication and assessment was analyzed based on the MSCT image results.Results One month after the surgery,Grade I lipiodol deposition of nodular hepatocellular carcinoma shown by the MSCT scan accounted for more than 76.67%,higher than that of the mass type,which was 28.00%;Grade II lipiodol deposition accounted for 20.00%,lower than that of the mass type,which was 54.00%(P<0.01);Relapsing-Remitting nodular hepatocellular carcinoma acconted for 80.00%after surgery,higher than the 28.00%in terms of mass type(P<0.01);no significant difference was shown in the effective rate for these two types of hepatocellular carcinoma.Conclusion MSCT is with high application value for the analysis of curative effect classification and assessment of TACE for hepatocellular carcinoma.It can provide an objective evaluation for the surgical effect and prognosis,and guide the patients to take the necessary treatment steps and improve the prognosis of the patients;therefore,it is with certain value to be popularized in clinical application.
Hepatocellular Carcinoma;Multi-slice Spiral CT;TranscatheterArterial Chemoembolization;Curative Effect Classification
10.3969/j.issn.1009-4393.2017.10.011
侯江平,E-amil:373299567@qq.com