瞬时弹性成像技术检测肝脾硬度值对乙肝肝硬化患者食管静脉曲张破裂出血的预测价值
2017-04-20朱清静万十千
刘 丹 朱清静* 万十千
瞬时弹性成像技术检测肝脾硬度值对乙肝肝硬化患者食管静脉曲张破裂出血的预测价值
刘 丹①朱清静①*万十千①
目的:探讨FibroScan瞬时弹性成像技术检测肝脾硬度值对乙肝肝硬化患者食管静脉曲张(EV)破裂出血(EVB)的预测价值。方法:选取100例乙肝肝硬化患者,患者食管静脉曲张程度为无静脉曲张18例,轻度静脉曲张30例、中度静脉曲张28例和重度静脉曲张24例;患者中无出血52例,单次出血28例,多次出血20例;患者Child-Pugh分级A级34例,B级30例,C级36例;100例患者均采用FibroScan瞬时弹性成像技术检测肝脾硬度,比较患者不同Child-Pugh分级、不同EV程度和不同EVB情况的肝脾硬度值。结果:Child-Pugh C级患者肝脏和脾脏硬度值明显高于Child-Pugh A级和Child-Pugh B级患者,其差异有统计学意义(t=21.13,t=12.04,t=11.24,t=9.741;P<0.05),随着患者EV严重程度加重,肝脾硬度值明显升高,不同EV程度患者肝脏硬度值和脾脏硬度值均存在明显差异,有统计学意义(F=7.494,F=8.129;P<0.05);多次出血患者肝脏和脾脏硬度值明显高于无出血和单次出血患者,差异有统计学意义(t=13.13,t=18.14,t=12.15,t=17.46;P<0.05)。结论:FibroScan瞬时弹性成像技术检测肝脾硬度值预测乙肝肝硬化患者EVB具有较高的临床价值,其操作简单,可重复性好,是一种较为成熟的无创检查。
乙肝肝硬化;食管静脉曲张;瞬时弹性成像技术;食管静脉曲张破裂出血
食管静脉曲张(esophageal varices,EV)是乙肝肝硬化患者的常见并发症,而食管静脉曲张出血(esophageal varices bleeding,EVB)是导致患者死亡的重要原因,早期确诊并积极治疗EV可有效降低乙肝肝硬化患者发生EVB的概率[1-2]。FibroScan瞬时弹性成像技术是通过肝脏硬度测量(1iver stiffness measurement,LSM)和脾脏硬度测量(spleen stiffness measurement, SSM)判断患者肝硬化严重程度的检测技术,具有操作简单、无创伤性及可反复多次检测等优点,目前已逐渐应用于临床[3]。然而,目前尚缺少采用此技术检测肝脾硬度预测胃底EVB风险性的相关报道。为此,本研究拟探讨FibroScan瞬时弹性成像技术检测肝脾硬度对乙肝肝硬化患者EVB的预测价值。
1 资料与方法
1.1 一般资料
回顾性分析2015年2月至2106年5月武汉市医疗救治中心住院或门诊治疗的100例乙型肝炎肝硬化患者病例资料,其中男性75例,女性25例;平均年龄为(47.1±11.2)岁;病程为8~22年。根据电子胃内窥镜检查所示,EV严重程度患者中无静脉曲张18例,轻度静脉曲张30例,中度静脉曲张28例,重度静脉曲张24例;所有乙型肝炎肝硬化患者根据血清总胆红素、白蛋白表达水平、凝血酶原时间、肝性脑病严重程度以及是否出现腹腔积液等情况的Child-Pugh分级A级34例,B级30例,C级36例;患者既往病史中出现EVB无出血52例,单次出血28例,多次出血20例。所有患者均已签署知情同意书,研究方案已通过医院伦理委员会批准。
1.2 纳入与排除标准
(1)纳入标准:所有患者经临床症状体征、实验室及影像学检查均符合乙肝肝硬化诊断标准[4]。
(2)排除标准:①腹腔大量积液,脾脏厚度<4 cm或脾脏已外科切除;②已采取EV相应治疗及伴随出现肝癌者。
1.3 仪器设备
采用FibroScan502型肝脏瞬时弹性检测仪(法国eCHOSENS公司)检测肝脾硬度。
本病案患者上呼吸道感染的诱因,起病较急,病情快速恶化,既往患有糖尿病,长期口服降糖药,但血糖控制不理想,无慢性中耳炎病史,CT检查发现提示右侧中耳乳突炎症,部分乳突及鼓室天盖欠连续;血液及耳分泌物细菌培养,结果培养出A族链球菌GAS。诊断为急性化脓性中耳炎,GAS脑膜炎,GAS败血症,2型糖尿病。
1.4 检测方法
所有患者入院后均进行肝脾硬度检测。患者取仰卧位为检查体位,右臂置于头部并充分暴露肋间隙,检测区域为右侧腋前线至腋中线间的第7~9肋间隙;检测脾脏硬度时患者取仰卧位为检查体位,左臂置于头部并充分暴露肋间隙,检测区域为左腋后线第9~11肋间隙,检测过程中探头需垂直于皮肤表面,根据TM、A模式确定检查位置无误后进行检测,所有患者均检测10次,取中位数为最终检查结果。检查期间需注意肝脾组织有足够的厚度,且不存在大血管组织结构,距离肝脾组织边缘也较远,若操作成功率<6次或检查结果偏差大于中位数1/3则需重新检查。
1.5 观察与评价指标
分别比较患者不同Child-Pugh分级、不同EV程度和不同EVB情况的肝脾硬度值。
1.6 统计学方法
采用SPSS16.0统计学软件对数据进行分析处理,计量资料以均数±标准差(x-±s)表示,组间两两比较采用t检验,多组间比较采用单因素方差分析,以P<0.05为差异有统计学意义。
表1 不同Child-Pugh分级患者肝脾硬度值比较(±s)

表1 不同Child-Pugh分级患者肝脾硬度值比较(±s)
Child-Pugh分级例数肝脏硬度值t值P值脾脏硬度值t值P值A级346.3±2.321.13<0.0520.5±7.8--B级3019.1±4.512.04<0.0541.7±14.511.24<0.05 C级3633.5±9.6--52.4±16.49.74<0.05
表2 不同EV程度患者肝脾硬度值比较(±s)
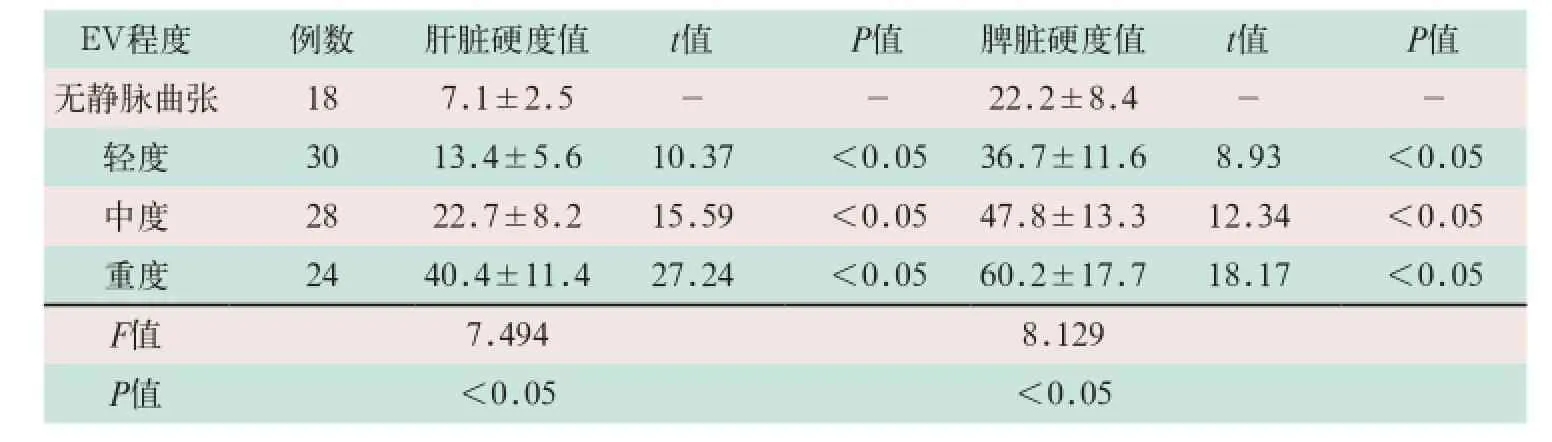
表2 不同EV程度患者肝脾硬度值比较(±s)
EV程度例数肝脏硬度值t值P值脾脏硬度值t值P值无静脉曲张187.1±2.5--22.2±8.4--轻度3013.4±5.610.37<0.0536.7±11.68.93<0.05中度2822.7±8.215.59<0.0547.8±13.312.34<0.05重度2440.4±11.427.24<0.0560.2±17.718.17<0.05 F值7.4948.129 P值<0.05<0.05
2 结果
2.1 不同Child-Pugh分级患者肝脾硬度值比较
Child-Pugh C级患者肝脏硬度值明显高于Child-Pugh A级和B级患者,其差异有统计学意义(t=21.13,t=12.04;P<0.05),而Child-Pugh B级和C级患者脾脏硬度值明显高于Child-Pugh A级患者,其差异有统计学意义(t=11.24,t=9.741;P<0.05),见表1。
2.2 不同EV程度患者肝脾硬度值比较
不同EV程度患者肝脏和脾脏硬度值随着曲张严重程度加重均存在明显的差异性,肝脏和脾脏硬度值明显升高,其差异有统计学意义(F=7.494,F=8.129;P<0.05)。肝脏硬度值EV轻度、中度和重度患者与无静脉曲张患者比较,差异有统计学意义(t=10.37,t=15.59,t=27.24;P<0.05);脾脏硬度值EV轻度、中度和重度患者与无静脉曲张患者比较,差异有统计学意义(t=8.93,t=12.34,t=18.17;P<0.05),见表2。
2.3 不同出血情况患者肝脾硬度值比较
(1)多次EVB情况患者肝脾硬度值明显高于无出血和单次出血患者;无出血患者与单次出血和多次出血患者肝脏硬度值比较,差异有统计学意义(t=13.13,t=18.14;P<0.05);无出血患者与单次出血和多次出血患者脾脏硬度值比较,差异有统计学意义(t=12.15,t=17.46;P<0.05),见表3。
(2)FibroScan瞬时弹性成像检测LSM和SSM硬度值如图1、图2所示。
图1 肝脏硬度值为33.0 kPa的FibroScan瞬时弹性成像
图2 脾脏硬度值为45.0 kPa的FibroScan瞬时弹性成像
表3 不同出血情况患者肝脾硬度值比较(±s)

表3 不同出血情况患者肝脾硬度值比较(±s)
出血情况例数肝脏硬度值t值P值脾脏硬度值t值P值无出血528.4±2.9--30.4±11.3--单次出血2822.7±8.713.13<0.0547.5±15.812.15<0.05多次出血2030.2±12.418.14<0.0558.8±17.417.46<0.05
3 讨论
EVB是乙肝肝硬化患者发展至晚期阶段的常见并发症,也是导致患者死亡的主要原因。目前,胃镜检查是临床用于评估EV严重程度的金标准,但此方法可对患者造成一定损伤,部分患者拒绝接受,故寻找一种可替代胃镜检查的无创检测指标显得极为重要[5]。FibroScan瞬时弹性成像是近些年逐渐应用于临床的无创检查方法,可通过测定LSM而评估肝硬化患者的肝纤维化严重程度,其作用机制主要为:通过FibroScan瞬时弹性成像探头振动轴释放出低频弹性波,进而在肝硬化患者机体内进行传播,同时超声换能器也发射超声波,可跟踪弹性波在患者机体内的传播并且对传播速度予以精确测量,最后显示相应图像,FibroScan瞬时弹性成像检测仪器根据相应软件可将弹性波传播速率转变为硬度值[6]。FibroScan瞬时弹性成像检测值是一个客观的物理学参数,与组织硬度有着直接的相关性关系,在理论上适用于各种类型所致的肝硬化患者。此外,FibroScan瞬时弹性成像不会对患者机体造成任何损伤,可反复多次进行检测,故可广泛用于动态监测患者肝硬化发展趋势,还可用于指导医务人员的临床治疗[7-8]。有研究证实,FibroScan瞬时弹性成像不但可用于评估肝硬化患者肝纤维化的严重程度,还可以预测门静脉高压症及EVB等严重并发症发生的风险性[9]。
乙肝肝硬化患者发展至疾病晚期阶段均存在不同程度的脾脏肿大现象,患者多合并有门静脉高压症,进而导致脾脏明显充血,并使得脾脏组织异常增生并呈纤维化病理改变,最终导致脾脏内部密度出现显著性改变。近年来,有研究通过SSM从而反映肝硬化患者肝纤维化严重程度,以及判断与EV的相关性,其检测优势在于不会受到肝脏炎症反应,以及谷丙转氨酶、谷草转氨酶及总胆红素出现异常等多种因素的影响[10-11]。相关研究证实,SSM检测值与肝硬化患者发生EV的风险性具有明显的相关性关系,且显著性优于LSM[12-13]。Colecchia等[14]研究认为,脾脏瞬时弹性成像值可动态监测肝硬化患者门静脉压力变化情况,还可准确预测EV的发生风险性。Colecchia等[15]的前瞻性研究结果显示,脾脏瞬时弹性成像值和MELD评分建立的模型可替代肝静脉压力梯度,可准确预测肝硬化患者的疾病预后情况。
本研究结果显示,Child-Pugh C级患者肝脾硬度值明显高于Child-Pugh A级和B级,而Child-Pugh B级患者肝脾硬度值明显高于Child-Pugh A级;不同食管静脉曲张程度患者肝脾硬度值均存在明显的差异性,且随着曲张严重程度加重,肝脾硬度值明显升高;多次出血患者肝脾硬度值明显高于无出血患者和单次出血患者,而单次出血患者肝脾硬度值明显高于无出血患者。由此表明,FibroScan瞬时弹性成像检测肝脾硬度、预测乙肝肝硬化患者EVB具有较高的临床价值。
[1]Chen YI,Ghali P.Prevention and management of gastroesophageal varices in cirrhosis[J].Int J Hepato1,2012,2012:750150.
[2]Xu Xiu-hua,Xiang Xiao-xing,Zhou Nianlan.The analysis of risk factors of acute esophageal varices bleeding in patients with liver cirrhosis[J].Chinese Hepatology,2014,19(1): 24-27.
[3]Guo Chun-mei,Wu Jing,Liu Kui-lian,et al. The predictive value of transient elastography for esophageal varices in hepatocirrhosis and its correlation with liver function classification[J]. Chin J Gastoenterol Hepatol,2016,25(3):314-317.
[4]中华医学会肝病学分会,中华医学会感染病学分会.慢性乙型肝炎防治指南(2010年版)[J].中华肝脏病杂志,2011,19(1):13-24.
[5]Liu Fang,Li Jun,Han Tao,et al.Assessment of the presence of esophageal varices bleeding in patients with hepatitis B virus-related cirrhosis by a noninvasive score system[J].Chin J Intect Dis,2014,32(2):111-115.
[6]Xuan JQ,Li MX,Su S,et al.Evaluation of degree of liver fibrosis and liver functional reserve in patients with chronic hepatitis B using fibroScan score[J].J Clini Hepatol,2012,28(4):285-288.
[7]Chen YP,Zhang Q,Dai L,et al.Is transient elastography valuable for high-risk esophageal varices prediction in patients with hepatitis-B-related cirrhosis[J].J Gastroenterol Hepatol,2012, 27(3):533-539.
[8]王红霞,辛晓梅,张丽娟,等.瞬时弹性波诊断仪在监测慢性乙型肝炎疾病进展中的应用价值分析[J].中国医学装备,2016,13(7):61-63.
[9]Wang JH,Chuah SK,Lu SN,et al.Transient elastography and simple blood markers in the diagnosis of esophageal varices for compensated patients with hepatitis B virus-related cirrhosis[J].J Gastroenterol Hepatol,2012,27(7): 1213-1218.
[10]Stefanescu H,Radu C,Procopet B,et al.Noninvasive menage a trois for the prediction of high-risk varices:stepwise algorithm using lok score,liver and spleen stiffiaess[J].Liver Int,2015,35(2):317-325.
[11]Zhang W,Wang L,Wang L,et al.Liver stiffness measurement,better than APRI,Fibroindex,Fib-4,and NBI gastroscopy,predicts portal hypertension in patients with cirrhosis[J].Cell Biochem Biophys,2015,71(2):865-873.
[12]Fraquelli M,Giunta M,Pozzi R,et al.Feasibility and reproducibility of spleen transient elastography and its role in combination with liver transient elastography for predicting the severity of chronic viral hepatitis[J].J V-tral Hepat,2014,21(2):90-98.
[13]Singh S,Eaton JE,Murad MH,et al.Accuracy of spleen stiffness measurement in detection of esophageal varices in patients with chronic liver disease:systematic review and meta-analysis[J]. Clin Gastroenterol Hepatol,2014,12(6):935-945.
[14]Colecchia A,Montrone L,Scaioli E,et al.Measurement of spleen stiffness to evaluate portal hypertension and the presence of esophageal varices in patients with HCV-related cirrhosis[J].Gastroenterology,2012,143(3):646-654.
[15]Colecchia A,Coli A,Casazza G,et al.Spleen stiffness measurement can predict clinical complications in compensated HCV-related cirrhosis:A prospective study[J].J Heptol,2014,60(6):1158-1164.
The predictive value of liver and spleen stiffness detected by transient elasticity imaging technology on esophageal varices bleeding of patients with hepatitis B cirrhosis
LIU Dan, ZHU Qing-jing, WAN Shi-qian//
China Medical Equipment,2017,14(4):80-83.
Objective: To discuss the predictive value of liver and spleen stiffness detected by transientelasticity imaging technology on esophageal varices bleeding (EVB) of patients with hepatitis B cirrhosis. Methods: 100 patients with hepatitis B cirrhosis (18 cases were no EV, 30 cases were mild EV, 28 cases were moderate EV and 24 cases were severe EV) were selected. In these patients, 52 cases were no bleeding, 28 cases were single hemorrhage and 20 cases were multiple hemorrhage. As the Child-Pugh grading, there were 34 cases were A grade, 30 cases were B grade and 36 cases were C grade. All of the liver and spleen stiffness of these patients were detected by instantaneous elasticity imaging technology, and to compare different Child-Pugh grading of patients, different EV degree, and liver and spleen stiffness on different EVB situation. Results: The liver and spleen stiffness of patients in Child-Pugh C stage were significantly higher than that in Child-Pugh A stage and B stage, respectively (t=21.13, t=12.04, t=11.24, t=9.741; P<0.05). With the aggravating of the severe degree of EV, the liver and spleen stiffness were significant increasing, and there were significant differences between different EV degree patients for liver stiffness and spleen stiffness, respectively (F=7.494, F=8.129, P<0.05). The liver and spleen stiffness of multiple hemorrhage group were significant higher than that of no-hemorrhage group and single hemorrhage group, respectively (t=13.13, t=18.14, t=12.15, t=17.46; P<0.05). Conclusion: By using instantaneous elasticity imaging technology to detect liver and spleen stiffness can predict EVB of patient with hepatitis B cirrhosis and it has higher clinical value, therefore, it is a sophisticated noninvasive examination with simple operation and better repeatability.
Hepatitis B cirrhosis; Esophageal varices; Transient elasticity imaging technology; Esophageal varices bleeding
10.3969/J.ISSN.1672-8270.2017.04.021
1672-8270(2017)04-0080-04
R575.2
A

2017-01-17
①武汉市医疗救治中心北六病区 湖北 武汉 430000
*通讯作者:zhuqing@163.com
[First-author’s address] The Sixth Area of North, The Medical Emergence Centre of Wuhan, Wuhan 430000, China.
