Problem analysis and solutions of the B-ultrasound-guided peripherally inserted central catheter process
2016-12-21ZuYanFanTianTianWangYunXiaoYangEnZhangDongHaoWuZhiHuanLinDanChunWuJinXiangLin
Zu-Yan Fan,Tian-Tian Wang,Yun Xiao,Yang-En Zhang,Dong-Hao Wu,Zhi-Huan Lin, Dan-Chun Wu,Jin-Xiang Lin
Department of Medical Oncology,The Third Affiliated Hospital of Sun Yat-sen University,Guangzhou,Guangdong 510630,China
Original Article
Problem analysis and solutions of the B-ultrasound-guided peripherally inserted central catheter process
Zu-Yan Fan,Tian-Tian Wang,Yun Xiao,Yang-En Zhang,Dong-Hao Wu,Zhi-Huan Lin, Dan-Chun Wu,Jin-Xiang Lin*
Department of Medical Oncology,The Third Affiliated Hospital of Sun Yat-sen University,Guangzhou,Guangdong 510630,China
A R T I C L E I N F O
Article history:
Received 4 April 2016
Received in revised form
3 June 2016
Accepted 13 July 2016
Available online 5 October 2016
B-ultrasound
PICC
Seldinger approach
Problems
Analysis
Nurse
Objective:The purpose of this study was to address the issues that occur during the B-ultrasound guided peripherally inserted central catheter(PICC)process and to give a summary of the effective management to these issues accordingly.
Methods:The information was collected retrospectively on all of the 1950 PICCs inserted during the 2-year period from July 2013 to July 2015.PICC catheter insertion was performed using the Seldinger approach and was delivered from the basilic vein to the superior vena cava in a B-ultrasound guided manner.Moreover,the point raised during the PICC process would be treated immediately.
Results:All of the PICCs were inserted successfully.The problems encountered are shown in the inserted central catheter(PICC)process,such as failures of venipuncture,the problem of inserting guide wire,the catheter was difficult to be delivered etc.
Conclusions:The B-ultrasound guided approach enhanced the average success regarding the PICC insertion,particularly for the subset with a poor condition in the elbow superficial vein.Due to the items that emerged in the PICC process,the effective prevention prior to surgery and treatment during the operation would be necessary.
©2016 Shanxi Medical Periodical Press.Publishing services by Elsevier B.V.This is an open access article under the CC BY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
1.Introduction
Peripherally inserted central catheter(PICC)is a venipuncture technique that delivers a catheter from the basilic vein to the superior vena cava,which has been widely used in patients who need chronic venous access.1The most common way of delivering a catheter is to operate carefully under direct vision.However,this approach sometimes fails because of the poor elbow superficial vein status.A B-ultrasound guided approach offers an opportunity to change this situation.2This technique originated in the 1990s and has shown great advantages in many aspects,including a much simpler step,a shorter operating time,a lower complexity and so on.3We retrospectively collected all of the 1950 PICCs that were inserted during the 2-year period from July 2013 to July 2015.All of the PICCs were inserted with 100%success,and in addition,we discuss several common problems during the operation and provide the methods to solve these problems.
2.Methods
2.1.Clinical material
A total of 1950 patients were enrolled,including patients with poor vascular condition as well as those who needed long-term intravenous nutrition or adjuvant chemotherapy.Among the patients,males(1057)between theageof0.8and75yearsmadeupthe large majority.The catheter models used were a 3F catheter,4F catheters(1367),and 5F catheter(568).PICCs were successfully delivered to all of the patients,including 31 with leukemia,125 with lymphoma,259 with breast cancer,603 with colon cancer,53 with ovarian cancer,13 with cervical cancer,191 with gastric cancer,15 withesophagealcancer,84withnasopharyngealcarcinoma,411with lung cancer,13 with prostate cancer,36 with liver cancer,12 with fungalmeningitis,41withseverepneumonia,16withpepticulcer,28 with cerebrovascular accident and 19 with myocardial infarction.
2.2.Methods
The B-ultrasound guided PICC process was provided forall of the patients.Beforethe operation,weevaluated the vascular status byaB-ultrasound and,then,conducted the following steps in sequence, disinfection,whisk onto the patient's operative region,establish a sterile area,scan the cross-section of the vein and find the largest vein in the 1/3 distal upper arm and put it right in the middle of the horizontal staff.Next,we chose the right acuductor and pierced the puncture needle through it and threaded the guide wire to guide the wire.Then,lidocaine was injected at the venipuncture site,the skin was incised with a knife,and the body cavity was pierced. Finally,the conduit and Coleus were withdrawn,and the PICC was inserted into the vein.
3.Result
All of the PICCs were inserted with 100%success.In the inserted central catheter(PICC)process,the problems encountered are shown in Table 1.
4.Analysis of the cause of common problems and solutions
4.1.Failures of venipuncture
4.1.1.Cause analysis
Patient's factors:Uncooperative patients,resulting in displacement of the probe in the venipuncture,such as in infants and fidget patients.
Instrument factors:an inappropriate acuductor model was selected.
Operating factors:(1)There were great differences between the traditional PICC cathetering method and venipuncture under ultrasound and the micro intubation sheath.Beginners may fail frequently as a result of the poor hand-eye cooperation.(2)The speed of venipuncture was too fast that the needle pierced the blood vessel.
4.1.2.Solutions
Treatment of patient's factors:Explain before puncturing and provide mental nursing to avoid the tense and noncooperation of the patients.If the patients are infants,it is advisable to puncture after sedation.
Treatment ofinstrumentfactors:Beforeskindegerming, examine the blood vessels by ultrasound to identify the venipuncturesites and acuductor models.Before the puncture,examine the vessel again with the probe and verify the acuductor model.If there is any discrepancy from the first examination,examine carefullyonce again and choose the acuductor model onthe basis of the last examination.The choice of acuductor is vital to the success of the PICC intubation under the guidance of ultrasound.
Operating skills:(1)Provide more training to beginners,especially training on hand-eye cooperation.(2)The preferred venipuncture site is the basilica vein approximately 4 cm-10 cm above the elbow because the basilica veins there are relatively superficial and will be much easier for the ultrasound probe to reach.Moreover,its dissection position is usually unchanged,it is relatively straight,and its diameter is medium,which is easy for changing dressings and invulnerable to the flexion of the elbow. Moreover,it is easier to fix the probe to reduce the failure caused by displacement of the probe.(3)After the skin degerming,whisk the Drapes as large as possible and extend the puncturing limb to an angle of 90°to expose it fully.While adjusting the limb to make it easier for puncturing,it should also be comfortable for the patient to cooperate fully and move less.(4)The fixing of the acuductor should be firm.After fixing the acuductor,it should be checked and a close connection of the punctureneedle and the acuductor should be ensured to avoid failures caused by their detachment.(5)While puncturing,the puncturing limb of the patient and the chest of the operator should be at the same horizontal level.The operator should be a supporting point for the left hand,which holds the probe.In this way,it could notonly prevent the displacement of the probe but also avoid squashing the vessel and displacement of the vessel.(6)Puncture slowly and while inserting the needle,observe the b-scan screen and avoid staring at the needle.When the puncture can be felt or there are light-spots on the vascular image, the puncturing should be stopped.Wait for a while and there will be blood return.If the blood return gets faster and drops,this symbolizes the success of puncturing.
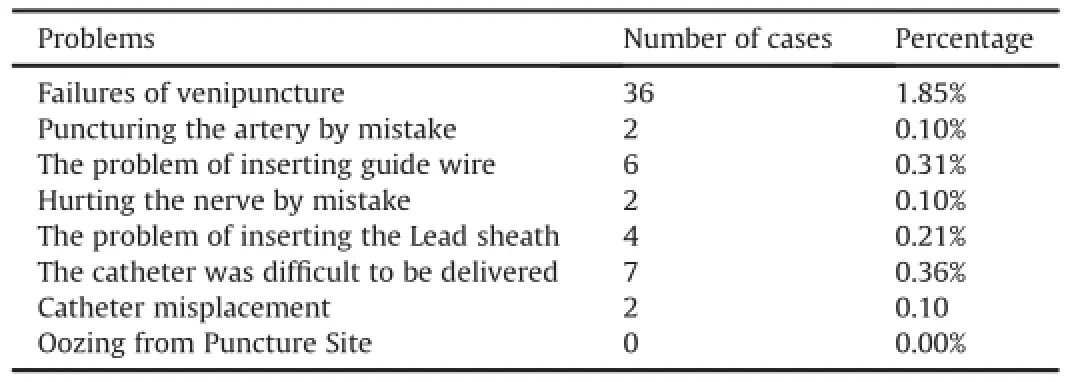
Table 1Problems encountered in the process of central catheter(PICC)insertion.
4.2.Puncturing the artery by mistake
4.2.1.Cause analysis
Patient's factors:Uncooperative patients maycause the probe to shift while puncturing,especially when puncturing the brachial artery,because the brachial artery and the brachial vein are in parallel.
Operating factors:Inaccurate examination before the puncture.
4.2.2.Solutions
Treatment of patient's factors:If it is an uncooperative patient, such as an infant or a fidgeting adult suffering cerebrovascular disease,we should try to avoid puncturing the brachial vein.
Operating skills:A detailed assessment of the blood vessels before puncturing and checking the vessel before inserting the needle are vital steps to avoid puncturing the artery by mistake.By pressing the cross section of the blood vessel using the probe during the assessing process,it could be observed that the blood flow in the vein almost stopped and there is no pulse,while the blood flow in artery was unblocked and generally there was a pulse. Whenpuncturing,if the blood squirted,the blood flow in the artery was unblocked and generally there was a pulse.If the blood squirts back,this symbolizes the mistake of puncturing the artery.In this case,the operator should withdraw the puncture needle immediately and carry out effective hemostasis by compression.
4.3.The problem in inserting the guide wire
4.3.1.Cause analysis
Patient's factors:The condition of blood vessel is poor,which usually manifests as more in the venous valve,vascular fibrosis and luminal stenosis.4
Operating factors:(1)Incorrect placement of the bevel of the puncture needle.(2)Loosening the tourniquet too early after the puncturing.If the tourniquet is loosened as soon as the puncture needle is inserted,the limbs of the patient move and the bounce of the vascular increases,and then,the puncture needle would be ejected from the vessel lumen,and the guide wire could not be inserted.(3)The probe oppressed the vessel while inserting the guide wire.(4)If the acuductor separated too early,the needle would also be ejected from the vessel lumen.
4.3.2.Solutions
Treatment of the patient's factors:In addition to assessing the cross section of the vessel before puncturing,the condition of the blood flow also needs to be assessed from the longitudinal section. Through a comprehensive evaluation,we can choose blood vessels with good elasticity,rich blood and a venous valve.
Operating skills:(1)At the time of the puncturing of a blood vessel,the bevel of the needle should be directed to the heart direction,otherwise the guide wire cannot be inserted along the vessel.(2)Insert the guide wire as soon as the puncture succeeds. Reduce the angle of the ultrasonic sensor by 5-10°while inserting it and avoid oppressing the skin above the puncture site.(3)Once it is ensured that the guide wire can be inserted into the vessel for 5-10 cm,separate the acuductor and the needle,and finally, remove the ultrasonic sensor and loosen the tourniquet.
4.4.Hurting the nerve by mistake
4.4.1.Cause analysis
Vascular factors:(1)There are rich circular nerves around the brachial vein.(2)The venous valve is penetrated,and the valve nerves are affected.
Operating factors:puncturing was too deep that peripheral nerves were affected.
4.4.2.Solutions
Operating skills:(1)Avoid puncturing too deep.(2)Avoid puncturing the venous valve.(3)Avoid penetrating the brachial vein.(4)Once symptoms of nerve injury are observed,withdraw the puncture needle quickly and apply hot packs,and then,puncture on the other upper limb.
4.5.The problem of inserting the lead sheath
4.5.1.Cause analysis
Operating factors:The coupling agent of the sheath was not cleaned completely,and thus,the left hand of the operator slipped and the skin was not tightened,and the lead sheath slid into the subcutaneous tissue.
4.5.2.Solutions
Operating skills:Before extending the skin,press the puncture site completely until the bleeding stops and clean the bloodstain and coupling agent around the puncture site.When inserting the lead sheath,tighten the skin to avoid the situation of the sheath from sliding off the blood vessel.
4.6.The catheter is difficult to deliver
4.6.1.Cause analyses
Vascular factors:It is related to obstacles in the blood vessel, such as vascular stenosis,encountering venous valve,vascular branching,and a medical history of a repeated puncture,drug damage,elderly patients,severe dehydration,hypertension,low body temperature,poor lying posture,local anesthetic reactions and venous spasm.
Operating factors:When withdrawing the guide wire and the needle core,the introducer sheath coat is not firmly fixed and,thus, slides off the blood vessel.
4.6.2.Solutions
Treatment of vascular factors:(1)Before the puncture,learn more about the detailed medical history and examine the body as well as the chest,avoiding the puncture on the side of body with a historyof trauma.(2)If the patient is nervous with cold extremities, in addition to trying to comfort and relax them,give them a hot water bottle to keep them warm.If the patient has severe dehydration,provide hydration through the peripheral vein.(3)In the event of a venous obstruction or vascular stenosis,one operator uses a 20 ml syringe connecting to the catheter with a bolus of 0.9% sodium chloride injection.5Additionally,the other operator conducts a little retracement of the catheter and,then,rotates the delivery tube with the slow injection meanwhile.Ensuring that all of the above considerations have been carried out,the catheter should be delivered successfully.6
Operating skills:Before the withdrawal of the guide wire,push and press the introducer sheath with the left thumb to fix it,and the other four fingers should press the blood vessel in the front end of the introducer sheath at the same time so that it not only stops the bleeding but also prevents the prolapse of the introducer sheath coat off the blood vessel.
4.7.Catheter misplacement
4.7.1.Cause analysis
Vascular factors:A medical history of subclavian vein intubation or peripheral vein chemotherapy leads to fiber formation on the vein wall and a narrow vein cavity.
4.7.2.Solutions
Operating skills:(1)When the catheter is delivered into 10-20 cm,assist the patient to lie in a horizontal posture without a pillowand turn the patient's lower mandible tothe operated side of the bodyand press against the shoulder.(2)After inserting the PICC tube,check the jugular vein with the b-ultrasound.Once the catheter is placed into the jugular vein,withdraw it immediately and oppress the jugular vein with the ultrasound probe and then insert the catheter again.
4.8.Oozing from the puncture site
4.8.1.Cause analysis
Patient's factors:Blood coagulation dysfunction of the patient.
Operating factors:Damage to the blood vessels during the process of cutting the skin.
4.8.2.Solutions
Treatment of the patient's factors:(1)Give a strict preoperative evaluation,especially on the blood coagulation function and the platelet count of the patient.(2)After the preoperative,if the patient has a bleeding tendency it can be pressed to stop the bleeding.
Operating skills:(1)When the skin is incised,avoid cutting too deep or at too large of an angle in case of a blood vessel injury.(2) When there is a severe postoperative hemorrhage,stop the bleeding and use a gelatin sponge or an alginate dressing to press the puncture site for 24 h in case of rebleeding.
5.Discussions
By using an intravascular ultrasound,the manipulator can have a clear observation of the blood vessels and a better judgment on the state of the blood vessels,which is a key point in reducing the tissue damage and increasing the success rate of a one-time puncture.7Meanwhile,using an intravascular ultrasound in the vascular assessment before the puncture can help to avoid situations in the venous valves and branch vein.Puncturing a large veincan cause possible obstacles and unpredictable stenosis.A smooth delivery of the catheter8also reduces the incidence of phlebitis and thrombus.6
In terms of the problems involving accidental artery and nerve injury,we suggest a serious assessment before puncturing and selecting the basilica vein to catheterize,keeping away from the arteries and nerves nearby.In regard to the difficulty in the insertion of the catheter,Song et al9believe that the loss of access is associated with vasospasm due to the patients'overstrain.Therefore,to overcome the difficulties in our group,we keep the arm warm and slowly inject physical saline while inserting the catheter, which was reported by Li et al10Although Shi et al proposed that the success rate of inserting a catheter was only 50%by adjusting position and injecting physiological saline.11For the patients with an ectopic catheter in our group,a careful assessment of the jugular vein by the B ultrasound was performed immediately after inserting the catheter.Once the ectopic catheter was found in the jugular vein,part of the catheter was retreated,and the B ultrasound probe was applied to press the jugular vein and the catheter was reinserted at the same time,making it easy and precise to reach the superior vena cava.Whereas sometimes errhysis in the puncture area occurs.REPTILASE,12alginate dressing,13thrombin14and Yunnan Baiyao powder15dressing the wound could staunch the bleeding.In our opinion,wetting and an external application do not keep the wound dry and clean but instead increase the risk of infection.Thus,we do not advocate any hemostatic methods except for gauze pressing on the wounds of the patients receiving the PICC. Only when the bleeding is serious enough do we use a gelatin sponge or Sorbalgon to press the puncture area.After close observation,all of the patients in our group did not have serious bleeding in the wound.
To insert a PICC under the guidance of ultrasound,first,psychological nursing is very important.Patients need to cooperate with the doctors and under the guidance of the psychological nurses.Meanwhile,an assessment before the puncture,methods of the puncturing and skills dealing with all of the possible problems are also keys to a successful catheterization.During the process of inserting a PICC,the two most common problems are puncture failure and guide wire insertion,especially for beginners.Being familiar with the skills to solve these problems will certainly improve the success rate of PICC.
In conclusion,PICC,under the guidance of ultrasound,should be fully utilized clinically because patients can benefit greatly from its advantages.However,it must be realized that there are still difficulties to be overcome.Only when the doctors are proficient can they provide a high quality service to the patients.
Conflicts of interest
All contributing authors declare no conflicts of interest.
1.Meng CY.Peripherally inserted central catheter care 25 cases.Chin J Pract Nurs. 2003;19:46-47(in Chinese).
2.Hu JE,Gong L,Tang YX,Zhang Q,Zhou ZF.Color doppler flow imaging-guided PICC venous catheter.J Nurs Sci.2007;22:39-40(in Chinese).
3.Tian Q,Yan YL,Zhang YX,Huang DF.Peripherally inserted central catheter Groshong®PICC catheter complications Cause Analysis and Countermeasures. J Nurs Sci.2006;21:44-45(in Chinese).
4.Zhang XH,Zhou J.Three-way valve type of PICC Catheter people ectopic surgery observation and care.Chin Nurs Res.2010;24:1904-1905(in Chinese).
5.Schweickert WD,Herlitz J,Pohlman AS,Gehlbach BK,Hall JB,Kress JP. A randomized,controlled trial evaluating postinsertion neck ultrasound in peripherally inserted central catheter procedures.Crit Care Med.2009;37: 1217-1221.
6.Polak JF,Anderson D,Hagspiel K,Mungovan J.Peripherally inserted central venous catheters:factors affecting patient satisfaction.AJR Am J Roentgenol. 1998;170:1609-1611.
7.Nichols I,Humphrey JP.The efficacy of upper arm placement of peripherally inserted central catheters using bedside ultrasound and microintroducer technique.J Infus Nurs.2008;31:165-173.
8.LaRue GD.Efficacy of ultrasonography in peripheral venous cannulation. J Intraven Nurs.2000;23:29-34.
9.Song QP,Qi HX.The cancer patients PICC catheter difficulties and countermeasures.Nurs Prac Res.2009;6:77-78(in Chinese).
10.Li XL,Li XY,Zhan YY,Yuan Z,Liu XY.Peripherally central venous catheter tube 23 cases of ectopic reason analysis and treatment.Contemp Nurse(College Ed). 2010;11:145-146(in Chinese).
11.Shi Y,Li YH,Yi JH,Li LY.PICC catheter ectopic progress in prevention and treatment of abnormal position.J Nurs.2012;19:21-24(in Chinese).
12.Jiang Z,Guo HY.REPTILASE after PICC catheter hemostatic effect was observed. Qilu Nurs.2005;11:1039-1040(in Chinese).
13.Cai CL,Huang YL,Li Q,Tan JH,Zhang JL,Wang H.Alginate dressing for the prevention and care microcannula sheath under the effect of ultrasoundguided PICC aided puncture site bleeding.Chin J Noso.2012;22:3574-3575 (in Chinese).
14.Liang RR,Qiu LQ,Yue LQ,Wu L.Blood diseases PICC management application. Tianjin J Nurs.2005;13:1-2(in Chinese).
15.Zhao J,Zhang XH,Xiao CX,Zhao F.Leukemia patients improved PICC nursing 96 cases.Chin J Pract Nurs.2003;19:11-12(in Chinese).
How to cite this article:Fan Z-Y,Wang T-T,Xiao Y,et al.Problem analysis and solutions of the B-ultrasound-guided peripherally inserted central catheter process.Chin Nurs Res.2016;3:142-145. http://dx.doi.org/10.1016/j.cnre.2016.10.001
*Corresponding author.
E-mail address:13247389981@163.com(J.-X.Lin).
Peer review under responsibility of Shanxi Medical Periodical Press.
http://dx.doi.org/10.1016/j.cnre.2016.10.001
2095-7718/©2016 Shanxi Medical Periodical Press.Publishing services by Elsevier B.V.This is an open access article under the CC BY-NC-ND license(http://creativecommons. org/licenses/by-nc-nd/4.0/).
杂志排行
Frontiers of Nursing的其它文章
- Effects of music therapy on mood,language,behavior,and social skills in children with autism:A meta-analysis
- Exploration of a reasonable dialysate temperature setting in hemodialysis for patients with hypertension
- The effectiveness of a high-fidelity teaching simulation based on an NLN/Jeffries simulation in the nursing education theoretical framework and its influencing factors☆
- An investigation of the health value and self-care capabilities of the elderly in urban-rural fringe area nursing homes and the related influencing factors☆
- GUIDE FOR AUTHORS
- Research progress in nursing subspecialization