An investigation of the health value and self-care capabilities of the elderly in urban-rural fringe area nursing homes and the related influencing factors☆
2016-12-21JuYingLuoLingLinKongZhiXiZhngYnShengYeCuiYuBoLiJunTuZhenYng
Ju-Ying Luo,Ling-Lin Kong,*,Zhi-Xi Zhng,Yn-Sheng Ye,Cui-Yu Bo, Li-Jun Tu,Y-Zhen Yng
aNursing School,Hubei University of Science and Technology,Xianning,Hubei 437100,China
bCommunity Health Center of Xianning City,Xianning,Huibei 437100,China
cPeople's Hospital of Chibi,Chibi,Hubei 437300,China
Original Article
An investigation of the health value and self-care capabilities of the elderly in urban-rural fringe area nursing homes and the related influencing factors☆
Ju-Ying Luoa,Ling-Lin Konga,*,Zhi-Xia Zhanga,Yan-Sheng Yea,Cui-Yu Baoa, Li-Juan Tub,Ya-Zhen Yangc
aNursing School,Hubei University of Science and Technology,Xianning,Hubei 437100,China
bCommunity Health Center of Xianning City,Xianning,Huibei 437100,China
cPeople's Hospital of Chibi,Chibi,Hubei 437300,China
A R T I C L E I N F O
Article history:
Received 11 October 2015
Received in revised form
2 February 2016
Accepted 17 June 2016
Available online 15 September 2016
Urban-rural fringe area
Elderly
Health value
Self-care capability
Objective:To investigate the health value and self-care capabilities of the elderly living in urban-rural fringe area nursing homes and the factors that influence these variables.
Methods:A cluster sampling method was used to select 280 elderly individuals from seven urban-rural fringe communities in Xianning to complete a survey regarding their health value and self-care capabilities.
Results:The total health value and self-care capability scores of the elderly were 7.45±1.45 and 100.25±22.56,respectively.Both of these scores significantly differed by age,education level,marital status,and income(P<0.05,P<0.01).Self-care capability was correlated with health value(r=0.521).A multivariate linear regression analysis showed that health value,marital status,and age predicted selfcare capability.
Conclusions:Elderly people living in the urban-rural fringe area with higher health values also had higher self-care capabilities.The self-care capabilities of the elderly can be enhanced by improving their health value using the“knowing-trusting-acting”model.
©2016 Shanxi Medical Periodical Press.Publishing services by Elsevier B.V.This is an open access article under the CC BY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
1.Introduction
Aging has increasingly become a serious social problem in China,and the severity of the pension problem has become increasingly obvious.1Rapid growth,the“empty nest”tendency, the large population base,and advanced age are the major aging trends in China.2The pension problem associated with the elderly living in urban-rural fringe communities differs from that of the elderly living in either urban or rural regions.This problem is generated byand has developed with the process of urbanization in China.These areas are the intermediate link in the evolution from countrysideto citiesand representthetransition from anagricultural civilization to an industrial civilization.As this process advances,numerous rural populations are changing into urban populations.Thus,the pension issue associated with the elderly in these particular areas,especially empty nesters,is worthy of concern.With increasingly improved community functions,the pension model that includes nursing homes has emerged and became important.The health value and self-care capabilities of the elderly in these nursing homes are important health-related concepts.To understand the health value and self-care capabilities of the elderly in urban-rural fringe area nursing homes and their related influencing factors,280 elderly people from this area were selected to complete a survey.
2.Participants and methods
2.1.Participants
Using cluster sampling,the elderly people in the nursing homes of seven communities located in the urban-rural fringe area of outer Xianning City were selected in July 2014 to participate in thissurvey.The inclusion criteria were the elderly(1)with the ability to express and easily communicate their conscious thinking;(2)with the ability to express independent judgment and cognitive ability; (3)above 60 years old;and(4)with an understanding and willingness to cooperate in the study.Participants were excluded if they(1)showed associated mental or related disorders;(2)were in the end stage of a disease;or(3)were diagnosed with the onset of an acute or chronic disease.
2.2.Methods
2.2.1.Survey
The survey was divided into three sections that recorded the general information,health value,and self-care capabilities of the elderly.(1)Self-prepared general information questionnaire-This section of the survey addressed demographic characteristics such as age,gender,income level,education level,marital status,and retirement date.(2)Health value questionnaire-This section of the survey was primarily used to investigate the health value of the elderly.This questionnaire consisted of 10 items:passionate life, comfortable life,independence and freedom,happiness,good health,harmonious mood,relaxed and happy life,sense of accomplishment,self-esteem,and social recognition.This questionnaire was sorted based on the importance of the respondents' entries.The highest score was 10,and scores of 1-4,5-7,and 8-10 represented low,medium,and high levels according to the literature.3(3)Self-care capability questionnaire-This section of the survey was used to assess the self-care capabilities of the elderly.It includes 43 items and consists of four dimensions of self-care:responsibility,self-care knowledge,self-care skills,and self-concept. The score for each entry ranges from 0 to 4,and the total score is a maximum of 172.Higher scores denote stronger self-care capabilities.The percentage of the participants'real scores that account for the total score on the questionnaire reflects the self-care capabilities of the respondents.Actual score proportions that represent 66%-100%,33%-66%,or 0-33%of the total score denote high, medium,or low levels of self-care capability,respectively.This survey has a validity coefficient of 0.88 and a reliability coefficient of 0.724 when it is used in China.4
2.2.2.Survey methods
The survey personnel received a standardized training that included knowledge about the assessment,communication skills, and relevant standardization for the investigation.After obtaining consent from the participants and their nursing homes,the survey was conducted via face-to-face interviews.The self-report method was used.The investigator applied oral questioning for the elderly participants who were unable to write their answers,and the questionnaire was completed by the investigator.In sum,300 questionnaires were distributed,and 280 valid questionnaires were collected,providing an effective recovery rate of 93.33%.
2.2.3.Statistical methods
All the data were input using SPSS 13.0 to establish a database, and descriptive statistics were performed.The self-care capabilities and health value of the elderly were compared across different characteristics using independent-samples t-tests and analyses of variance.The correlation between the health value and the selfcare capability scores of the elderly was analyzed using Pearson's correlation analysis and a multivariate linear regression.
3.Results
3.1.General information of the elderly in the urban-rural fringe areas
A total of 280 elderly people from seven nursing homes were selected as the participants,including 118 males(42.14%)and 162 females(57.86%).The participants ranged in age from 60 to 91 years (76.45±11.34);64 people were over 80 years old(22.86%),157 people were 70-80 years old(50.07%),and 59 people were 60-70 years old(27.07%).The education levels of the sample were college or above(56 people;20.00%),junior high and high school(99 people;35.36%),and elementary school or below(125 people; 44.64%).The marital statuses of the sample were unmarried, divorced,or widowed(129 people;46.07%)and married(151 people;53.93%).The average incomes were 2500 yuan or higher (55 people;19.64%),1500-2500 yuan(124 people;44.28%),and 1500 yuan or below(101 people;36.08%).
3.2.Health value and self-care capabilities of the elderly
According to our survey,the average overall health value score of the elderly living in the urban-rural fringe area was 7.45±1.45.A total of 159 people were in the high level,87 people were in the medium level,and 34 people were in the low level.The total selfcare score was 100.25±22.56,and the actual score accounted for 58.14%of the total score;thus,the overall self-care capability was medium,although 49 people werein the lowlevel,164 people were in the medium level,and 67 people were in the high level.
3.3.Comparison of the health value and self-care capabilities of the elderly across different categories(Table 1)
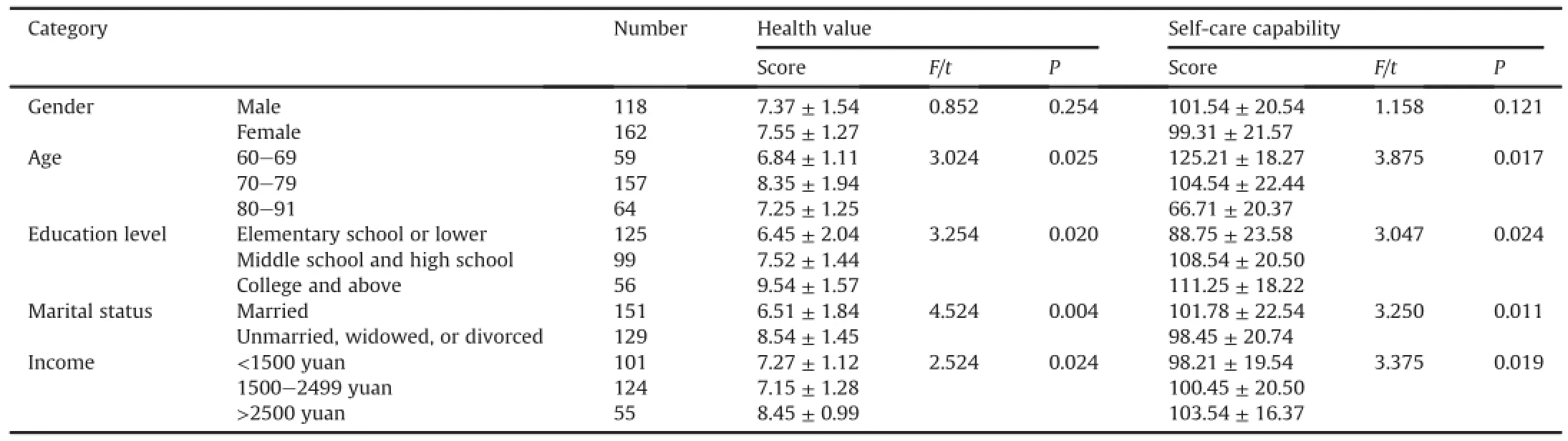
Table 1Comparisons of the health value and self-care capabilities of the elderly across different categories.

Table 2A multivariate linear regression analysis of the main factors that influence the self-assessed self-care score of the elderly living in the urban-rural fringe area.
3.4.Correlation of the health value and self-care capabilities of the elderly living in the urban-rural fringe area
The Pearson's correlation coefficient between the health value score and the self-care capability score of the elderly was r=0.521. Using the self-care capability score of the elderly as the dependent variable and the health value and related sociodemographic factors of the elderly as the independent variables,a multivariate linear regression analysis was performed.The results showed that the health value score,education level,and age predicted self-care capability(see Table 2).
4.Discussion
4.1.Analysis of the health value of the elderly living in the urbanrural fringe area across different categories
The results of this study show that the health value score of the elderly was 7.45±1.45,and the high and medium level groups accounted for 56.78%and 31.07%of the total,respectively.The health value of the elderly in this study can be considered as relatively high.With regard to the different categories,the health value level of the elderly with a high level of education was greater than that with a low level of education.The health value level of the elderly in the high income group was greater than that of the elderly in the low income group.Finally,the health value level of the elderly differed the most by marital status:i.e.,the elderly who were unmarried,widowed,or divorced had a significantly higher health value than those who were married.Regarding the effect of the demographic factors on the health value of the elderly,the results of previous studies are consistent with the findings of the current study.Muhlenkamp et al.5showed that education level affected the health value such that higher education levels predicted higher health value levels.Gao et al.1also came to the same conclusion.It is generally believed that a higher education level leads to a correspondingly better family financial condition,and this population also pays more attention to their health.Moreover, the elderly with high education levels are more concerned about their health management and more easily accept community health education and advertising.In addition,widowed and unmarried statuses are considered as significant and negative life events among the elderly;however,such life events might generate certain positive effects.For example,losing a spouse might increase their concern regarding their own health and therefore improve their health value level.This supposition might explain the different health values based on marital status.6
4.2.Analysis of the self-care capabilities of the elderly living in the urban-rural fringe areas across different categories
The overall self-care capability level of the elderly in this region was at a medium level,and this result is similar to the finding of the on-site cross-sectional study conducted by the researchers in the urban pension agency.7The self-care capabilities of elderly people with low education levels were worse than those of the elderly with high education levels;furthermore,the self-care capabilities of the older elderly were worse than those of the younger elderly.Importantly,the self-care capabilities of the participants also differed by financial situation.In addition, the elderly differed by type of family.The self-care capabilities of the elderly who were widowed or divorced were worse than those of who were married.Men did not significantly differ from women.Regarding the research on self-care capability,the selfcare theory of Orem is an important theoretical model,and manyresearchers have performed a significantamount of research using this theoretical model.Some researchers have suggested that income,education level,and marital status are the important factors that affect self-care capabilities.4,8Foreign researchers investigated 235 community-dwelling elderly people and found that social support,marital status,age,education level,and income affect their self-care capabilities.9Orem's selfcare theory indicates that self-care is composed of self-care behaviors,and these behaviors play important roles in individual maintenance,health promotion,and living a comfortable life,all of which are affected by multiple individual and social factors. The results of this study support this theory.
4.3.Analysis of the relationship between health value and self-care capability
According to our results,Pearson's correlation coefficient describing the relationship between the health value and self-care capabilities of the elderly was r=0.521.An additional regression analysis showed that health value,marital status,and age predicted self-care capability.Health value positively predicted self-care capability.This result suggests that the elderly living in the urban-rural fringe area with higher health values generally had better self-care capabilities.Furthermore,increasing the health value of the elderly positively improves the self-care capabilities of these patients.The“knowing-trusting-acting”model,a core of health education theory,is one possible explanation.This model addresses health-related behaviors,and the self-care capabilities of the elderly can be improved by strengthening their self-health behaviors.This process of change can be divided into three continuous processes:health knowledge access,the generation of the health beliefs,and the formation of health behaviors(i.e., knowing-trusting-acting).10Therefore,we conclude that improving health value of the elderly will positively enhance their self-care capabilities,representing the process from “trusting”to“acting”in the“knowing-trusting-acting”model.
Conflicts of interest
All contributing authors declare no conflicts of interest.
1.Gao XQ,Ding SZ,Wang J,Han L.Correlation between health promoting lifestyles and health value in the elderly.Chin J Health Psych.2015;23:769-771(in Chinese).
2.Zhang YX,Ma J,Gui Y,Li XP.Quality of life in the elderly with regard to the community pension models across different regions and their influencing factors.Chin J Gerontol.2014;34:1334-1336(in Chinese).
3.Pender NJ.Health Promotion in Nursing Practice.2nd ed.Stamford,Connecticut: Appleton&Lange;1987:165-166.
4.Yang ZL,Sun JP.Study of the Self-care Capabilities of the Elderly in an Urban Area of Fenyang City and its Related Factors.Taiyuan:Shanxi Medical University; 2007:3-4(in Chinese).
5.Muhlenkamp AF,Broerman NA.Health beliefs,health value,and positive health behaviors.West J Nurs Res.1988;10:637-646.
6.Tang T.Study on the Post-traumatic Situation of cancer Patients and the Influencing Factors.Chongqing:Third Military Medical University;2013:22-23 (in Chinese).
7.Liu YB,Meng W,Chu QQ,et al.Survey of elderly health literacy and self-care capability in the nursing homes of Urumqi.J Nurs Sci.2013;28:80-82 (in Chinese).
8.Geng GL,Liang T,Yuan YL.Logistic regression analysis of the factors influencing the self-care of stroke patients.J Centr Univ Natl.2006;15:315-318(in Chinese).
9.Callaghan D.Healthy behaviors,self-efficacy,self-care,and basic conditioning factors in older adults.J Community Health Nurs.2005;22:169-178.
10.Kong MZ.Effect of the“knowing-trusting-acting”health education mode on the disease knowledge and compliance behavior of patients with coronary artery disease.Mod Clin Nurs.2011;10:43-45(in Chinese).
How to cite this article:Luo J-Y,Kong L-L,Zhang Z-X,et al.An investigation of the health value and self-care capabilities of the elderly in urban-rural fringe area nursing homes and the related influencing factors.Chin Nurs Res.2016;3:125-128.http:// dx.doi.org/10.1016/j.cnre.2016.06.015
☆This project was supported by 2014 Humanities and Social Science Research Projects,Department of Education of Hubei Province(No.14D069);2014 Humanities and Social Science Research Projects,Department of Education of Hubei Province (No.14Q106).
*Corresponding author.
E-mail address:50678088@qq.com(L.-L.Kong).
Peer review under responsibility of Shanxi Medical Periodical Press.
http://dx.doi.org/10.1016/j.cnre.2016.06.015
2095-7718/©2016 Shanxi Medical Periodical Press.Publishing services by Elsevier B.V.This is an open access article under the CC BY-NC-ND license(http://creativecommons. org/licenses/by-nc-nd/4.0/).
杂志排行
Frontiers of Nursing的其它文章
- Problem analysis and solutions of the B-ultrasound-guided peripherally inserted central catheter process
- Effects of music therapy on mood,language,behavior,and social skills in children with autism:A meta-analysis
- Exploration of a reasonable dialysate temperature setting in hemodialysis for patients with hypertension
- The effectiveness of a high-fidelity teaching simulation based on an NLN/Jeffries simulation in the nursing education theoretical framework and its influencing factors☆
- GUIDE FOR AUTHORS
- Research progress in nursing subspecialization