Primary delusion and the sociopolitical milieu in India - A case report & short review
2016-12-09RahulSAHAAasthaSHARMA
Rahul SAHA*, Aastha SHARMA
·Case report·
Primary delusion and the sociopolitical milieu in India - A case report & short review
Rahul SAHA*, Aastha SHARMA
prodrome, primary delusion, culture, sociopolitical environment, behavior
1. Introduction
Modern psychiatry should integrate all facets of knowledge of the behavior sciences, biology,pharmacology, sociology, and anthropology to serve a scientific approach in shaping human behaviors.[1]Bleuler described that the psychopathological features,especially the contents of delusions and hallucinations,[2,3]can be shaped by creating an environment due to societal developments.[4]Klaus Conrad advanced the concept of prodromal ‘‘delusional mood’’ or ‘‘atmosphere’’,[5,6]& his views ‘‘on the origin and development of psychotic experiences’’ were considered ‘‘completely new, and a source of new ideas for research on psychopathology.’’[7]
It has been shown in many studies that subjects suffering from schizophrenia react very sensitively concerning historical events and cultural novelties.[2,3,8]Socio-demographic background of may have a significant impact on content of delusions, including delusions of persecution.[12]We are reporting a case of a young man developing a primary delusion in the backdrop of general Lok Sabha election against a national leader thus depicting the role of socio-demographic background influencing the onset of primary delusion.
2. Case history
Mr. L, 25 year old Hindu unmarried male from a middle socioeconomic status, urban background residing in Delhi, educated up to standard 6, working as an agent in the banking sector presented to adult psychiatry OPD, PGIMER, Dr Ram Manohar Lohia Hospital along with his younger brother with chief complaints of suspiciousness, abnormal beliefs and experiences,hearing voices none else can hear and decreased sleep since 1 month. Patient reported himself in the OPD as he was very distressed about his abnormal experiences.
Exploration of History revealed that the illness started on the day of General Lok Sabha Elections in Delhi on April 10, 2014, when the patient had gone to cast his vote at the local poll booth. He got into an argument with the conducting team regarding where to put his signature. After returning home, he started reporting to his family members that his activities and movements were being telecast live on various channels under the orders of Vice President of the then Ruling party. Usually an avid television and technology enthusiast, he would not watch TV or answer his phone nor allow anyone else at home to switch on any electronic appliance, fearing that the same were being used to record his activities. Patient was totally asymptomatic prior to the Election Day. From the next morning onwards, he refused to step out of the house or even go out to work. He started suspecting that people in the neighbourhood were speaking about him. His family members tried to convince him to the contrary, but to no avail. He would also repeatedly say that people in the neighbourhood were also monitoring his activities through the live telecast. He would remain hypervigilant and kept guarding the door and muttering to self even at night, picking up fights with his brother if they would try to stop him. Over a period of next 7 days his suspiciousness solidified and he became more firm in his belief. As a result of his abnormal experience, he became more confined to his room and stopped going out of his house.
Over the next few days, he also started reporting of hearing voices. He would keep muttering to self most of the day. When asked about the reason, he would say that he was replying to the voices. Frequency of the voices increased over a period of next 7 days. His self care worsened and he started picking fights with neighbours and even the family members, sometimes even without provocation. There was gradual decrease in interaction with family members, lack of initiative in doing any work, lack of involvement in any pleasurable activities, apathy. Over the course of illness, patient became withdrawn to self; he would not take bath for weeks. His sleep decreased to 1-2 hours a day. All his symptoms started and developed within 7 days.Decrease in self care was observed in next week. He came for consultation by himself as he was not able to understand the reason for the abnormal experiences.His past, family, personal history and premorbid personality were non-contributory. (See Figure 1)
Mental status examination revealed decreased psychomotor activity, adequate personal hygiene.Patient was conscious of himself and his surroundings and he was well oriented to time, place, and person.His attention was arousable, but his concentration was impaired. His affect was fearful and irritable throughout the interview. His thinking showed delusional perception, sudden delusional idea, delusion of persecution and reference. He was suspicious against the Vice president of the then ruling party. When asked how he got to know about this, he elaborated that, on the day of election, as he went to press the button on the party of his choice on the EVM (Electronic Voting Machine), the lady volunteer at the booth looked towards him and laughed, and he felt that something odd was happening. He said it was because the lady at the poll booth looked at him and smirked, and it was in that moment that he just knew. Even though he had not overheard them speaking ill of him, he said he could make out from their gestures and facial expressions. He gave a delusional meaning to the smirking of the lady at the poll booth, which is indicative of ‘delusional percept’showcasing the ‘two memberedness’ of the primary delusion. ‘Two memberedness’ in the indexed case is because of the ‘normal visual perception of the patient regarding smirking by the lady at the poll booth’ and ‘the delusional meaning of being persecuted’ given by the patient. All his delusions were well systematized.
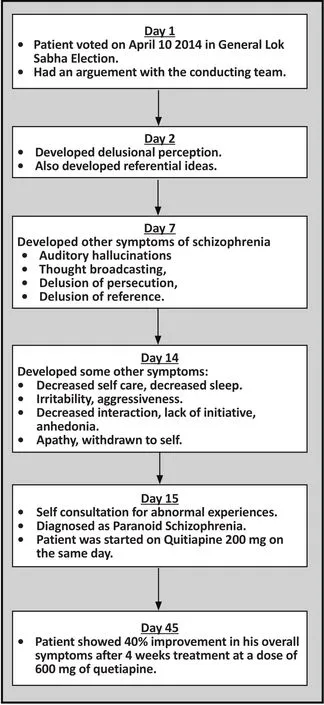
Figure 1. Flowchart depicting the onset, progression,and course of illness in the indexed patient
He would also report that his neighbours were able to read his thoughts and would plot against him.He started feeling that his thoughts were also being broadcast on TV and known to others, without his sharing it with anyone. He would not believe in contrary.Over a period of time his belief became more firm.His thinking showed thought broadcast. Over the next few days, he also started reporting hearing voices of multiple strangers, talking and discussing about him amongst themselves. He attributed these voices to some journalists who were covering his activities at the behest of the Vice President of the Ruling party.
Mental status examination also revealed auditory hallucinations- 2ndand 3rdperson auditory hallucination.The voices would discuss about killing him. He attributed the voices to the journalists and ruling party workers who would discuss about harming him. His immediate,recent and remote memory was intact. Patient had below average intelligence level. His abstract thinking was impaired. His judgment was impaired. Patient had no insight about his illness. All his routine investigations were within normal limit. Rorschach test findings were reported as follows: “psycho gram exhibited schizophrenic form psychosis”. His IQ test showed him to be of “low average intelligence [IQ= 85-90 (mental age around 12&1/2 years)]”
On the basis of history, mental status examination and Rorschach test finding he was diagnosed to be suffering from Paranoid Schizophrenia, (ICD-10,F-20.0). He was started on Quetiapine 200mg, gradually increased to 600mg and on his last visit to OPD, had shown 40% improvement. This case is described to bring to the fore an interesting presentation with a primary delusion, which is rare in the clinical settings, especially in the backdrop of the general elections.
3. Discussion
The main aim of this case report is to highlight the onset of primary delusion and the final progression to full blown symptoms of schizophrenia. We are hereby reporting the case of a 25 year old Hindu unmarried male from a middle socioeconomic status, urban background, educated up to standard 6, working as an agent in the banking sector, who presented with chief complaints of suspiciousness against the Vice President of the then Ruling Party. He developed a sudden delusional idea of being persecuted by the then Ruling Party. His delusional belief solidified over a period of time and other symptoms of schizophrenia became more evident as the illness progressed further. The onset of the delusional perception and sudden delusional idea was significantly related to the ongoing political environment at that period of time and thus having a direct temporal relation, while the auditory hallucinations, thought broadcast, delusion of persecution and delusion of reference appeared within next 7 days. It took approximately 2 weeks from the onset of prodromal symptoms and progression to full blown schizophrenia.
Specific conditions for the development of content of delusions of persecution existed in India during thattime. The ruling period of previous government changed the relationship of people, their thinking and behavior,their system of values, and religious issues. During the elections, many political issues took centre stage, which could have easily influenced the mind of a deluded patient. People were living in permanent inner tension,as everyone knew what was appropriate to say and what wasn’t, in order to not be opposed or criticized for having different political ideology. The constant inner tension during the election period could easily explain the initial PRODROMAL period, while the voting day on April 10, 2014 proved to be the trigger point for the onset of primary delusion. The excessive media hype and political interference in our day to day life can easily explain the formation of the delusion and the inclusion of ‘persecutor concerned’ into his delusional picture.
The socio-cultural background of the illness focuses mainly on medical issues within the framework of society, functioning, level of education and family status.[9,10,12]Azhar et al. found significant associations between cultural factors & symptoms and proved that culture influenced symptoms of mental illness.[11]While the frequency of major delusional themes is stable over longer periods, the specific shape of this content,for example “who is the persecutor,” “what is the reason for the persecution,” mainly depends on actual developments.[2,3,8,12]
There are two primary hypotheses for the formation of delusions, the “basic reasoning deficit hypothesis”and the “anomalous experience hypothesis”.[13]The former, and perhaps less popular, theorizes that delusions arise from a basic deficit in reasoning and illogical thinking. This hypothesis seems to explain the origin of his delusion in the indexed case discussed,. The patient developed a sudden illogical thinking against the Vice President of the then Ruling party only on the basis of predominant political environment during that period, without any evidences. This hypothesis has been criticized because, if illogical thinking were enough to cause delusions, there would presumably be more delusional thinking than is seemingly apparent in the general population.[13]However, recent epidemiologic research reveals relatively prevalent delusion-like experiences in the general population,[14,15]thereby not necessarily ruling out the reasoning deficit hypothesis.On the other hand, the anomalous experience hypothesis implicates hallucinations as an antecedent of delusions, attributing the rise of delusions to an attempt to explain anomalous perceptual experiences.[13]While this theory is insightful, it cannot explain the onset of delusion in the indexed patient as there was no evidence of any perceptual abnormality before the onset of the delusion.
In Conrad’s stage model, there is often a prodromal delusional mood prior to the onset of the delusions lasting days, months, or even years.[16,17,18]During this period, the patient experiences that something is ‘‘in the air’’ but is unable to say what has changed. The patient may feel not only excitement, ‘‘intoxicated’’anticipation, but also increasingly oppressive tension,suspiciousness, fear, depressive inhibition, guilt, a feeling of separation from others, and often a combination of these.[18]Conrad calls this initial expectational phase‘‘Trema’’ (stage fright) as the patient has the feeling that something very important is about to happen.[19]Attention is drawn toward irrelevant stimuli, thoughts,and associative connections, which are distressing and unpredictable. Everything that lies in the perceptual background or periphery to one’s attention becomes a potential threat.[16,18]The perceptual background,which remained unnoticed, now takes on a character of its own.[19]The indexed patient has described similar feeling during his initial few days of delusion formation.
Owen’s helpful definition of primary delusions includes both that one comes to believe new things(change in meaning) and arrives at such beliefs in a new way (transformation of experience).[19]The patient’s changed internal motivational-emotional state, the delusional mood, included every individual and the‘persecutor concerned’ into his delusional picture. He included the Vice President of the previous Ruling party because of the ‘Emotionally Charged Environment’created by the media during that time. As during the election period in April 2014, every discussion was related to politics, whether in social circle or family circle. So, an “EMOTIONALLY CHARGED CULTURAL AND SOCIOPOLITICAL ENVIRONMENT” was created, resulting in the onset and further solidification of his delusion.The fact that he voted against the ruling party resulted in worsening of his delusions and also precipitated other schizophrenic symptoms such as hallucinations.
4. Conclusion
Understanding patterns of emergence of delusions and hallucinations in psychotic disorders have significant relevance to nosology, prognosis, and treatment. We as psychiatrists should always keep in mind about the antecedent CULTURAL AND SOCIOPOLITICAL BACKGROUND of the patient during evaluation. This is imperative to enable us to truly appreciate the symptomatology and even plan alternative nonpharmacological treatment accordingly.
Con fl icting Interest
The authors declare that they have no conflict of interest related to this manuscript.
Funding
No funding support was obtained for preparing this case report.
Informed consent
The patient signed an informed consent form and agreed to the publication of this case report.
Authors’ contributions
Dr Rahul Saha was involved in the primary assessment,diagnosis and management of the indexed patient. The planning and execution of the article was done by me.The whole article was supervised by me and I gave my valuable input in writing the introduction and discussion and finalizing the draft. Dr Aastha Sharma was involved in the medical writing of the case report. She gave significant contribution in finalizing the manuscript. She was also involved in the initial assessment of the patient in the OPD.
1. Fabrega H. Cultural psychiatry: international perspectives.Epilogue. Psychiatr Clin North Am. 2001; 24(3): 595-608
2. Bleuler E. Textbook of Psychiatry 8. Dover reissue ed. New York: Dover Publications, Inc.; 1951
3. Bleuler E. Textbook of Psychiatry 2. New York: The Macmillan Company; 1924
4. Rudalevičienė P, Narbekovas A. [Psichiatro ir kunigo bendradarbiavimas - gydytojo praktikoje iškylanti būtinybė,iniciatyva. (Collaboration between psychiatrist and a priest - a necessity in psychiatric practice. An initiative.)]Sveikatos mokslai. 2005; 15(1): 62-68. Finnish
5. Berrios GE. The History of Mental Symptoms. Cambridge,UK: Cambridge University Press; 1996
6. Hambrecht M, Ha¨fner H. [‘‘Trema, Apopha¨nie,Apokalypse’’— Ist Conrads Phasenmodell empirisch begru¨ndbar? ] Fortschr Neurol Psychiatr. 1993; 61: 418-423. German
7. Ploog DW. Conrad K. In: Hirsch SR, Shepherd M,eds. Themes and Variations in European Psychiatry.Charlottesville, VA: University of Virginia Press; 1974. p:239-240
8. Jaspers K. Basic Philosophical Writings. New York:Humanity Books; 2000
9. Littlewood R, Dein S. Cultural Psychiatry and Medical Anthropology: An Introduction and Reader. London, New Brunswick, New Jersey: The Athlone Press; 2000
10. Tseng W-S. Handbook of Cultural Psychiatry. San Diego,London, Boston, New York, Sydney, Tokyo, Toronto:Academic Press; 2001
11. Azhar MZ, Varma SL, Hakim HR. Phenomenological differences of delusions between schizophrenic patients of two cultures of Malaysia. Singapore Med J. 1995; 36(3):273 - 275
12. Rudaleviciene P, Adomaitiene V, Stompe T, Narbekovas A,Meilius K, Raskauskiene N, et al. Delusions of persecution and poisoning in patients with schizophrenia: sociocultural and religious background. Medicina (Kaunas). 2010; 46(3):185-192
13. Maher BA. The relationship between delusions and hallucinations. Curr Psychiatry Rep. 2006; 8: 179-183
14. Kelleher I, Cannon M. Psychotic-like experiences in the general population: Characterizing a high-risk group for psychosis. Psychol Med. 2011; 41(1): 1-6. doi: http://dx.doi.org/10.1017/S0033291710001005
15. Van Os J, Linscott RJ, Myin-Germeys I, Delespaul P,Krabbendam L. A systematic review and metaanalysis of the psychosis continuum: evidence for a psychosis proneness-persistence-impairment model of psychotic disorder. Psychol Med. 2009; 39(2): 179-195. doi: http://dx.doi.org/10.1017/S0033291708003814
16. Conrad K. Die Beginnende Schizophrenie. Stuttgart,Germany: Thieme Verlag; 1958
17. Jaspers K. General Psychopathology. 7th ed. Hoenig J, Hamilton MW, trans. Manchester, UK: Manchester University Press; 1963
18. Klaus Conrad. Delusional mood, psychosis, and beginning schizophrenia. Schizophr Bull. 2010; 36(1): 9-13. doi:http://dx.doi.org/10.1093/schbul/sbp144
19. Owen G, Harland R, Antonova E, Broome M. Jaspers’concept of primary delusion (letter). BJP. 2004; 185: 77-78

Dr. Saha obtained his Bachelor of Medicine and Bachelor of Surgery degree in 2005 from Maharani LaxmiBai Medical College, Jhansi, Uttar Pradesh and an MD in Psychiatry in 2011 from King George’s Medical University, Lucknow, Uttar Pradesh. He is currently working as a senior research associate in the Department of Psychiatry at the Post Graduate Institute of Medical Educational &Research (PGIMER), Dr. Ram ManoharLohia (RML) Hospital, New Delhi. His research interests are the phenomenology of attention deficit hyperactivity disorder (ADHD) and schizophrenia. He is currently working on a project titled ‘Follow-up study of phenomenology and functional impairment in ADHD children’.
原发性妄想和印度的社会政治环境-一例病例报告和简短综述
Saha R, Sharma A
前驱症状,原发性妄想,文化,社会政治环境、行为
Delusion has always been a central topic for psychiatric research with regard to its etiology,pathogenesis, diagnosis, treatment, and forensic relevance. Among these, primary delusion seems to be the interest of many psychiatrists. Content of delusion has always been the area of interest of cultural psychiatry. We have tried to discuss the various aspects of primary delusion and also tried to explain how cultural and sociopolitical environment in a country like India can shape the formation of primary delusion and influence its psychopathology.
[Shanghai Arch Psychiatry. 2016; 28(4): 230-234.
http://dx.doi.org/10.11919j.issn.1002-0829.216040]
Department of Psychiatry and Deaddiction, PGIMER, Dr Ram Manohar Lohia Hospital, New Delhi 110001, India
*correspondence: Dr. Rahul Saha. Mailing address: Department of Psychiatry and Deaddiction, PGIMER, Dr Ram Manohar Lohia Hospital, New Delhi, India.Poscode: 110001. E-mail: drrahul.saha19@gmail.com.
概述:妄想一直是精神科研究的一个中心主题,研究涉及其病因、发病机制、诊断、治疗和司法精神病学的相关内容。许多精神科医生似乎对其中的原发性妄想尤为感兴趣。妄想的内容一直是文化精神病学感兴趣的领域。我们试图探讨原发性妄想的不同方面,试图解释在印度这样的国家中文化和社会政治环境如何决定原发性妄想的形成并影响其精神病理学。
猜你喜欢
杂志排行

上海精神医学的其它文章
- Some thoughts on the common issue of psychotherapy in different cultures — report on the China conference of psychoanalysis
- Treatment effect of antipsychotics in combination with horticultural therapy on the inpatients with schizophrenia: a randomized, case-controlled study
- A comparison study of Quetiapine and Risperidone’s effectiveness and safety on treating alcohol-induced mental disorder
- Repetitive transcranial magnetic stimulation combined with venlafaxine and lorazepam for treatment of generalized anxiety
- The prospects for the clinical application of exploratory eye movement among patients with psychotic disorders
- A case report of psychoactive drugs aggravating and alleviating Meige syndrome