动态压应力重建外固定技术免植骨治疗超大段胫骨缺损
2016-11-28乔永平原巧玲王劲淞孙滨丛培军
乔永平+原巧玲+王劲淞+孙滨+丛培军
【摘要】 目的:观察分析采用重建外固定技术动态加压免植骨治疗超大段骨缺损的临床效果。方法:22例骨缺损长度超过15 cm的胫骨骨缺损,断端彻底清创,清除硬化骨质,采用Ilizarov重建外固定技术,干骺端截骨,通过骨运输修复骨缺损,断端会师对接后对接点动态加压,以期通过压应力成骨方式获得骨愈合。采用Ilizarov技术研究应用学会(ASAMI)骨及功能评分进行评价。结果:所有病例获得了14~23个月的随访,平均17.6个月,骨缺损断端均骨性愈合,恢复下肢负重行走功能,ASAMI优良等级,20例未植骨获得了骨性愈合,2例重吸烟史合并糖尿病患者通过植骨获得骨愈合,未植骨愈合率为90.9%。22例病例均出现针孔钉孔渗出红肿等炎症反应,局部处理后愈合,未影响骨段滑移及骨愈合。结论:Ilizarov骨运输技术可有效修复超大段骨缺损,通过对接点加压可免植骨获得骨愈合效果可靠。
【关键词】 Ilizarov技术; 骨运输; 骨缺损; 植骨
【Abstract】 Objective:To observe and analyze the clinical effect of the reconstruction of external fixation technique for the treatment of large segmental bone defect.Method:22 cases with bone defect length more than 15 cm of the tibia bone defect,broken end thoroughly debridement, removal of bone sclerosis,the Ilizarov,fixation,metaphyseal osteotomy, bone transport through the repair of bone defect, the pressure on the dynamic contact ends of rendezvous docking, the compressive stress of osteoblasts obtained bone healing.The outcome were evaluated by using Association for the Study and Application of Methods of Ilizarov(ASAMI) scoring systeme.Result:All cases were followed up for 14-23 months,average 17.6 months.The bone defects were healed,the recovery of walking function of lower limb, the good grade of ASAMI.Bone healing was achieved in 20 cases without bone grafting,2 cases with severe smoking history and diabetes were treated with bone graft,and the rate of bone healing was 90.9%.In 22 cases,the inflammatory reaction, such as inflammation reaction, local treatment, and bone fracture healing were not affected by local treatment.Conclusion:Ilizarov bone transport technology can effectively repair large segmental bone defect, the contact pressure can obtain bone graft bone healing effect is reliable.
【Key words】 Ilizarov technology; Bone transportation; Bone defect; Bone graft
First authors adress:The Wendeng Osteopath Hospital of Shandong Province,Weihai 264400,China
doi:10.3969/j.issn.1674-4985.2016.30.011
缺损长度超过15 cm的超大段胫骨缺损,无法通过传统植骨的手段修复,即使通过Ilizarov骨重建技术修复骨缺损,后期需植骨获得骨愈合[1-2],笔者自2006年10月-2014年9月对22例骨缺损15.0~23.5 cm病例采用骨运输修复骨缺损,利用压应力成骨技术原理,采用对接点动态加压的方法免植骨获得骨愈合,疗效满意,现报告如下。
1 资料与方法
1.1 一般资料 本组共22例,男15例,女7例;年龄21~53岁,平均37.5岁。原发创伤:均为高能量胫腓骨粉碎骨折,其中开放骨折12例,病史追溯Grade ⅢA型7例,Grade Ⅱ型5例。创伤原因:高处坠落伤6例,车祸伤14例,重物砸伤2例。骨缺损原因:开放骨折大段骨丢失3例,感染性骨不连清创后骨缺损19例。进行骨修复前所经历手术次数3~7次,平均4.2次。原始创伤至骨重建时间4~25个月,平均9个月。对骨愈合有重要影响的长期重吸烟史2例,糖尿病5例。骨缺损长度为15.0~23.5 cm,平均17.2 cm。该研究已经伦理学委员会批准,患者知情同意。
1.2 手术方法 缺损断端清创截骨放置外固定支架手术,采用硬膜外麻醉或股神经+坐骨神经阻滞麻醉,充分切除骨缺损断端硬化骨质至缺损断端形成新鲜渗血骨面,断端尽可能平行,以利骨缺损断端对接后,获得尽可能大的对位面积,利于骨愈合,避免断端不平对接后持续加压造成成角畸形[3]。安装预先装配的环形外固定支架套入小腿,通常采用3模块的环形外固定支架构型,两端为固定胫骨远近端的固定模块,中间为滑移模块,如骨缺损位于胫骨远端,则外加跨踝关节的支架构型,调整外固定支架圆环距皮肤的距离。根据骨缺损离膝关节、踝关节的距离,选择血运丰富的干骺端附近截骨,利于骨块快速形成及获得良好矿化[4-5]。截骨方式采用1~2 cm小切口,用止血钳分开达骨面,插入微创连孔截骨器,用电钻钻孔,插入固定导针,用电钻继续钻孔直达对侧皮质,连续翻转移动微型连孔截骨器继续进行相同操作,在不超过2 cm小切口内完成干骺端的完全截骨,最大限度保护截骨平面软组织及血运,利于牵拉骨痂成骨。远端及近端固定骨段的固定设计2~3枚钢针形成交叉角度,交叉钢针的穿针点间距4~5 cm,中间滑移运输骨段以1~2枚交叉钢针固定,滑动骨段因在滑移过程中受力较大,可增加1枚半螺纹螺钉,以保证有效滑移。连接固定所有钢针及半螺纹螺钉,所有连接钢针需拉张,增强其强度,增加固定牢固性[6-7]。骨折端间骨缺损区,在闭合创口后形成空腔,需放置引流,减少瘢痕组织形成,利于骨折端加压反应成骨。
1.3 术后处理 截骨后经过7~10 d静息期后,开始按每天0.8 mm的速度,每天8次的频率,预定的滑动方向进行移动滑动模块,此牵拉速度及频率有别于目前通行的每天1 mm及每天6次的速度和频率。后期根据骨痂牵拉矿化形态及密度,调整牵拉速度,如出现漏沙样形态,减慢牵拉速度,或回缩进行手风琴技术操作,直至上述异常形态消失。在骨痂牵拉阶段,指导患者进行患肢未固定关节进行屈伸运动,术后疼痛明显减轻后,扶拐进行负重行走,经骨运输后,骨折断端对接会师,通过滑动模块继续进行加压,每周1次按0.2~0.4 mm/d的速度加压,每2周复查1次,直至骨折对接点折线模糊。注意护理针孔及钉道,避免出现针孔炎症加重、感染等并发症,影响患肢主动负重训练。
1.4 观察指标与评价标准 采用ASAMI评价系统进行骨愈合及功能评分,再生骨每厘米骨缺损矿化时间(RCI)及每厘米骨缺损携带外固定架时间(EFI)。
2 结果
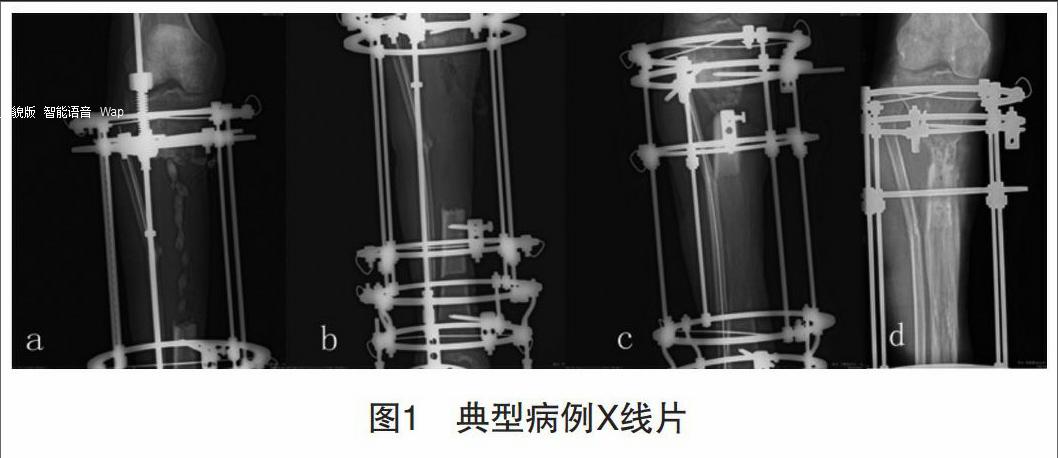
22例患者在除去外固定支架至最后一次复诊,获14~23个月随访,平均17.6个月。20例未植骨获得骨愈合,2例重度吸烟史合并糖尿病患者通过植骨获得骨愈合,免植骨骨愈合率为90.9%,ASAMI骨愈合情况及功能为优良,患侧肢体膝关节、踝关节功能均满足日常生活工作要求。RCI 1.29个月/cm,EFI 1.51个月/cm,平均外固定时间13.4个月。22病例均有外固定针道红肿、脓性分泌物感染表现,经局部处理均顺利控制。有3例骨运输患者在完成断端对接及加压治疗后,因支架钉、针松动固定失效,更换外固定支架螺钉继续固定。典型病例X线片见图1。
3 讨论
造成超过15 cm的超大段骨缺损,因缺乏足够的骨源,且大量无血运游离骨成活率低,成骨质量差,无法恢复下肢承重行走功能[8-9]。导致大段骨缺损的因素中,大部分为感染性骨不连清创导致大段骨缺损,存在不同程度游离植骨禁忌[10-12]。文献[13]报道,采用吻合血管的游离腓骨移植或者难度更大的组合组织移植的方法治疗,但此类手术创伤大,供区损伤大,腓骨胫骨化时间往往持续数年,且远远达不到胫骨的直径及强度,日常生活工作中极易出现再骨折。Ilizarov技术目前已经广泛应用在肢体矫形、肢体延长、骨缺损等领域,是治疗骨不连、骨缺损的金标准,通过骨痂牵拉成骨的骨运输的重建外固定技术,作为保肢的最后手段,已成为修复超过10 cm的大段骨缺损的唯一可靠有效方法[14]。本组研究病例,在骨缺损断端清创过程中,按彻底切除的原则,清除生物活力差的硬化骨质,至清创骨面出现活跃渗血,尽可能使两断端骨面平行,利于断端对接后获得最大接触面,利于骨断端愈合,避免加压成角[15]。在骨段滑移运输的过程中,滑移的频率和速度对骨痂牵拉区新骨形成有明显影响,根据笔者临床经验及相关文献报道,有别于目前通常采用的每天1 mm,分6次的频率,采用降低速度,增加频率的方式进行,每天0.8 mm,分8次的频率操作,可使牵拉区成骨更均匀,矿化质量更好,能避免出现牵拉骨痂呈漏沙样弊端[16]。
超过15 cm大段的骨缺损,在骨缺损区最少经过5个多月骨折端才能会师对接,期间骨折端形成纤维瘢痕组织,这对骨愈合是一种未知因素[17]。骨组织的再生生物学过程遵循Wolff定律,在应力应变的刺激下,局部组织能重现再生潜能,修复和重建肢体的形态和功能[18]。在下肢骨折的治疗过程中,临床中发现骨折延迟愈合,通常指导患者逐渐增加负重,利用应力传导刺激,促进骨折愈合。笔者根据上述Wolff定律及临床实践经验,断端会师对接后,采取断端加压的措施,通过压应力刺激,完成骨不连界面的转化成骨,恢复正常的骨性连接[19]。在对接点动态加压操作中,加压速度和频率不同于骨运输,需减慢频率,降低速度,以免造成持续加压导致的对接点成角及再生骨的骨折,需定期进行X线片检查,观察对接点解除及力线情况,如出现成角,进行回缩操作,纠正成角,2周后根据断端X线片表现再进行加压操作。本研究的结果显示骨折端对接后骨端加压,通过压应力转化成骨,未植骨骨愈合率为90.9%,提示对于超大段骨缺损,通过骨运输及压应力成骨技术,避免供骨区损害,可有效取得骨缺损修复及骨愈合,对明显骨缺损需植骨的治疗方法是一种突破。本组有2例重吸烟史患者骨缺损断端通过植骨获得骨愈合,尽管病例数量较少,但据本研究结果及文献[20]报道,长期吸烟可能对于骨运输后骨折端骨愈合具有影响。
参考文献
[1] Fürmetz J,Soo C,Behrendt W,et al.Bone transport for limb reconstruction following severe tibial fractures[J].Orthopedic Reviews,2016,8(1):6384.
[2] Sadek A F,Laklok M A,Fouly E H,et al.Two stage reconstruction versus bone transport in management of resistant infected tibial diaphyseal nonunion with a gap[J].Arch Orthop Trauma Surg,2016,136(9):1233-1241.
[3] Kawoosa A A,Wani I H,Dar F A,et al.Deformity correction about knee with ilizarov technique:accuracy of correction and effectiveness of gradual distraction after conventional straight cut osteotomy[J].Ortop Traumatol Rehabil,2015,17(6):587-592.
[4] Azzam W,El-Sayed M.Ilizarov distraction osteogenesis over the preexisting nail for treatment of nonunited femurs with significant shortening[J].Eur J Orthop Surg Traumatol,2016,26(3):319-328.
[5] Kim H T,Lim K P,Jang J H,et al.Resection of a physeal bar with complete transverse osteotomy at the metaphysis and Ilizarovexternal fixation[J].Bone Joint J,2015,97-B(12):1726-1731.
[6] Gubin A,Borzunov D,Malkova T.Ilizarov method for bone lengthening and defect management review of contemporary literature[J].Bull Hosp Jt Dis(2013),2016,74(2):145-154.
[7] Borzunov D Y,Balaev P I,Subramanyam K N.Reconstruction by bone transport after resection of benign tumors of tibia:A retrospective study of 38 patients[J].Indian J Orthop,2015,49(5):516-522.
[8] Davis J A,Choo A,OConnor D P,et al.Treatment of infected forearm nonunions with large complete segmental defects using bulk allograft and intramedullary fixation[J].J Hand Surg Am,2016,41(9):881-887.
[9] Li J J,Roohani-Esfahani S I,Dunstan C R,et al.Efficacy of novel synthetic bone substitutes in the reconstruction of large segmental bone defects in sheep tibiae[J].Biomed Mater,2016,11(1):1748.
[10] Kovoor C C,Jayakumar R,George V V,et al.Vascularized fibular graft in infected tibial bone loss[J].Indian Journal of Orthopaedics,2011,45(4):330-335.
[11] Allsopp B J,Hunter-Smith D J,Rozen W M.Vascularized versus nonvascularized bone grafts:what is the evidence[J].Clin Orthop Relat Res,2016,474(5):1319-1327.
[12] Schmidmaier G,Moghaddam A.Long Bone Nonunion[J].Z Orthop Unfall,2015,153(6):659-674.
[13] Krappinger D,Lindtner R A,Zegg M,et al.Masquelet technique for the treatment of large dia-and metaphyseal bone defects[J].Oper Orthop Traumatol,2015 ,27(4):357-368.
[14] Onyekwelu I,Hasan S,Chapman C B.Ilizarov external fixator for length salvage in infected amputated nonunions[J].Bull Hosp Jt Dis(2013),2014,72(2):176-180.
[15] Ahmad Khan R D,Maqbool M A.Effectiveness of ilizarov frame fixation on functional outcome in aseptic tibial gap non-union[J].
J Pak Med Assoc,2015,65(3):S179-S185.
[16] Luk H K,Lai Y M,Qin L,et al.Computed radiographic and ultrasonic evaluation of bone regeneration during tibial distractionosteogenesis in rabbits[J].Ultrasound Med Biol,2012,38(10):1744-1758.
[17] Polyzois V D,Stathopoulos I P,Lampropoulou-Adamidou K,et al.Strategies for managing bone defects of the lower extremity[J].Clin Podiatr Med Surg,2014 ,31(4):577-584.
[18] Schell H,Thompson M S,Bail H J,et al.Mechanical induction of critically delayed bone healing in sheep:radiological and biomechanical results[J].J Biomech,2008,41(14):3066-3072.
[19] Lovisetti G,Sala F.Clinical strategies at the docking site of distraction osteogenesis:are open procedures superior to the simple compression of Ilizarov[J].Injury,2013,44(10):S58-S62.
[20] Patel R A,Wilson R F,Patel P A,et al.The effect of smoking on bone healing:A systematic review[J].Bone Joint Res,2013,2(6):102-111.
(收稿日期:2016-06-19) (本文编辑:郎威)