Emergency department diagnosis of a concealed pleurocutaneous fi stula in a 78-year-old man using point-of-care ultrasound
2016-11-23RichardAminiAlbertAminiPatrickHollingerSuzanneMichelleRhodesCharlesSchmier
Richard Amini, Albert Amini, Patrick Hollinger, Suzanne Michelle Rhodes, Charles Schmier
1Emergency Medicine, University of Arizona,Tucson, Arizona 85724, USA
2Arizona Premier Surgery, 640 W Yellowstone Way, Chandler, Arizona 85248, USA
Corresponding Author: Richard Amini, Email: Richardamini@gmail.com
Emergency department diagnosis of a concealed pleurocutaneous fi stula in a 78-year-old man using point-of-care ultrasound
Richard Amini1, Albert Amini2, Patrick Hollinger1, Suzanne Michelle Rhodes1, Charles Schmier1
1Emergency Medicine, University of Arizona,Tucson, Arizona 85724, USA
2Arizona Premier Surgery, 640 W Yellowstone Way, Chandler, Arizona 85248, USA
Corresponding Author: Richard Amini, Email: Richardamini@gmail.com
World J Emerg Med 2016;7(4):307–309
INTRODUCTION
Although the differential diagnosis for chest wall masses is broad, the vast majority are abscesses, lipomas, or sebaceous cysts. Post-operative chest wall masses can also include infection, hematoma, seroma, cancer recurrence, metastasis, and lung hernia. Bedside ultrasound has been well documented to be beneficial in the differentiation of superficial pathology.[1,2]Pleurocutaneous fistula is a pathologic communication between the pleural space and subcutaneous tissues of the chest wall. Pleurocutaneous fi stula is a rare complication of tube thoracostomy, video-assisted thoracic surgery (VATS) procedures, and various pulmonary infections. There are multiple case reports of pleurocutaneous fi stulas occurring after tube thoracostomy as well as secondary to pulmonary infections including tuberculosis.[3–7]VATS is becoming an increasingly common surgery for treatment of lung carcinoma, spontaneous pneumothorax, and various indications in the trauma setting. Several cases series documenting VATS complications describe pleurocutaneous fi stulas after VATS procedures.[8,9]Point of care ultrasound (POCUS) is increasing in use as a diagnostic tool in the emergency department.[1,2,10–13]Here we present a case that highlights the intersection of a rare complication of a common procedure and the value of ultrasound in the diagnosis of undifferentiated masses and dyspnea in the emergency department.
CASE
A 78-year-old male presented to our Emergency Department complaining of right-sided chest pain, shortness of breath, and a chest wall mass after coughing. His history was significant for stage II lung cancer. Fourteen days prior to presentation the patient had undergone right lower lobectomy with lymph node dissection through VATS. The patient stated that he had coughed in the morning and felt a popping sound in his chest. Subsequently, the patient noticed a mass on his chest wall that changed size when he breathed. The patient's initial vital signs were significant only for an oxygen saturation of 93% while on 2 liters of supplemental oxygen. His physical exam was signifi cant for diminished breath sounds on the right side and scattered expiratory wheezes. Furthermore, the patient was noted to have a fl uid fi lled mass in his lower right chest wall at the incision site for the VATS procedure. This mass appeared to increase in size with inhalation (Figure 1).
The treating emergency physician who was fellowship trained in POCUS performed a POC ultrasound of the chest wall mass and found evidence of a right-sided pleural effusion with pleural fistula extending from the pleural space into the chest wall subcutaneous tissue (Figure 1). The rest of the patient's emergency department workup demonstrated a white blood cell count (WBC) of 22 000 and his chest radiograph (CXR) was positive for a right sided pleural effusion. The CXR demonstrated a pleural effusion; however, it did not demonstrate any evidence of a pleurocutaneous fistula (Figure 2). The patient was started on intravenous (IV) antibiotics, and as a result of the POC ultrasound, the cardiothoracic (CT) surgery service was consulted for admission. During his hospital course, the patient underwent repeat thoracic ultrasoundand interventional radiology performed ultrasoundguided thoracentesis removing 250 cc of fluid for symptomatic relief.

Figure 1. Top left: patient chest wall without obvious defect (expiratory image). Top right: Patient chest wall with obvious defect (inspiratory image). Bottom left: ultrasound image in expiratory phase demonstrating pleural effusion but only trace pleurocutaneous fi stula. Bottom right: ultrasound image in inspiratory phase demonstrating pleural effusion and large pleurocutaneous fi stula.
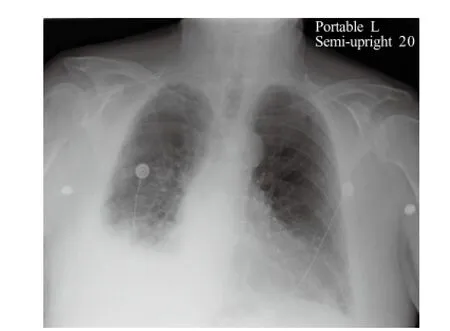
Figure 2. Chest radiograph demonstrating hazing of the costo-phrenic angle consistent with pleural effusion versus pneumonia.
DISCUSSION
Pleurocutaneous fi stula is a pathologic entity consisting of a persistent communication between the pleural space and subcutaneous tissue that can be a consequence of a broad spectrum of diseases including pleural tuberculosis, migrating foreign bodies, metastatic cancer, radiation therapy post mastectomy, tube thoracostomy, and a VATS procedure complication.[3–9]While rare, this case of a pleurocutaneous fi stula highlights the usefulness for point of care ultrasound as an aid to prompt diagnosis and clinical decision making. Case reports have described the diagnosis of this entity by both ultrasound and CT imaging.[4–7]In this case, the pleurocutaneous fi stula and the fistula tract were identified on ultrasound imaging, aiding in the correct diagnosis.
For over half a century emergency physicians have been using point of care ultrasound at the bedside to aid in diagnostic scenarios and therapeutic procedures.[12]Ultrasound is an integral component of undergraduate and graduate medical training and it being used for simple and complex procedures worldwide.[14–17]In the setting of a patient presenting with a subcutaneous thoracic mass, ultrasound has been shown previously to be of use in the aid in diagnosis and differentiation of multiple other diseases such as lipomas, abscesses, and lung herniation.[10]Furthermore, ultrasound can beused as an adjunct to procedures and treatment such as thoracentesis or drainage of abscesses.[1,2,18,19]In patients presenting with dyspnea of unknown etiology ultrasound has been shown to aid in the differentiation of congestive heart failure from other causes of acute dyspnea. Ultrasound can be used to assess for pleural effusions, pulmonary edema, pneumonia and pericardial effusions all of which may be useful in the undifferentiated patient with acute dyspnea.[13]Unlike pleural effusions, which are more easily identified by the novice sonographer, pleurocutaneous fi stula's are rare and smaller proving more difficult to diagnose. In this case ultrasound was used to diagnose both the pleural effusion and the pleurocutaneous fi stula; subsequently, it was also used to guide drainage.
In conclusion, this case highlights an interesting and unique fi nding on POC ultrasound imaging. Additionally, it suggests that POC ultrasound can be used as a diagnostic adjunct for the diagnosis and characterization of a pleural-cutaneous fi stula.
Funding: None.
Ethical approval: Not needed.
Conflicts of interest: The authors declare there is no competing interest related to the study, authors, other individuals or organizations..
Contributors: Amini R proposed the study and wrote the first draft. All authors read and approved the fi nal version of the paper.
REFERENCES
1 Tayal VS, Hasan N, Norton HJ, Tomaszewski CA. The effect of soft-tissue ultrasound on the management of cellulitis in the emergency department. Acad Emerg Med 2006; 13: 384–388.
2 Squire BT, Fox JC, Anderson C. ABSCESS: applied bedside sonography for convenient evaluation of superficial soft tissue infections. Acad Emerg Med 2005; 12: 601–606.
3 Lin MT, Shih JY, Lee YC, Yang PC. Pleurocutaneous fistula after tube thoracostomy: sonographic fi ndings. J Clin Ultrasound 2008; 36: 523–525.
4 Kirshenbaum KJ, Burke RC, Kirshenbaum MD, Cavallino RP. Pleurocutaneous fistula as a complication of oleothorax. CT fi ndings in three patients. Clin Imaging 1995; 19: 125–128.
5 Chan L, Reilly KM, Henderson C, Kahn F, Salluzzo RF. Complication rates of tube thoracostomy. Am J Emerg Med 1997; 15: 368–370.
6 Ferrante D, Arguedas MR, Cerfolio RJ, Collins BG, van Leeuwen DJ. Video-assisted thoracoscopic surgery with talc pleurodesis in the management of symptomatic hepatic hydrothorax. Am J Gastroenterol 2002; 97: 3172–3175.
7 Samuel LM, Kunkler IH, Dixon JM, Walker WS. Pleurocutaneous fi stula as a complication of radiation treatment in locally advanced breast cancer. J R Coll Surg Edinb 1997; 42: 138–139.
8 McKenna RJ, Houck W, Fuller CB. Video-assisted thoracic surgery lobectomy: experience with 1 100 cases. Ann Thorac Surg 2006; 81: 421–425; discussion 5–6.
9 Onaitis MW, Petersen RP, Balderson SS, Toloza E, Burfeind WR, Harpole DH Jr, et al. Thoracoscopic lobectomy is a safe and versatile procedure: experience with 500 consecutive patients. Ann Surg 2006; 244: 420–425.
10 Wagner JM, Lee KS, Rosas H, Kliewer MA. Accuracy of sonographic diagnosis of superfi cial masses. J Ultrasound Med 2013; 32: 1443–1450.
11 Mantuani D, Nagdev A. Three-view bedside ultrasound to differentiate acute decompensated heart failure from chronic obstructive pulmonary disease. Am J Emerg Med 2013; 31: 759.e3–5.
12 Moore CL, Copel JA. Point-of-care ultrasonography. N Engl J Med 2011; 364: 749–757.
13 Frankel HL, Kirkpatrick AW, Elbarbary M, Blaivas M, Desai H, Evans D, et al. Guidelines for the Appropriate Use of Bedside General and Cardiac Ultrasonography in the Evaluation of Critically Ill Patients-Part I: General Ultrasonography. Crit Care Med 2015; 43: 2479–2502.
14 Amini R, Adhikari S, Fiorello A. Ultrasound competency assessment in emergency medicine residency programs. Acad Emerg Med 2014; 21: 799–801.
15 Amini R, Kartchner JZ, Nagdev A, Adhikari S. Ultrasoundguided nerve blocks in emergency medicine practice. J Ultrasound Med 2016; 35: 731–736.
16 Hoyer R, Means R, Robertson J, Rappaport D, Schmier C, Jones T, et al. Ultrasound-guided procedures in medical education: a fresh look at cadavers. Intern Emerg Med 2016; 11: 431–436.
17 Zieleskiewicz L, Muller L, Lakhal K, Meresse Z, Arbelot C, Bertrand PM, et al. Point-of-care ultrasound in intensive care units: assessment of 1 073 procedures in a multicentric, prospective, observational study. Intensive Care Med 2015; 41: 1638–1647.
18 Kjær S, Rud B, Bay-Nielsen M. Ultrasound-guided drainage of subcutaneous abscesses on the trunk is feasible. Dan Med J 2013; 60: A4601.
19 Mercaldi CJ, Lanes SF. Ultrasound guidance decreases complications and improves the cost of care among patients undergoing thoracentesis and paracentesis. Chest 2013; 143: 532–538.
Accepted after revision April 13, 2016
10.5847/wjem.j.1920–8642.2016.04.013
Clinical Image
October 9, 2015
杂志排行
World journal of emergency medicine的其它文章
- The state and future of emergency medicine in Macedonia
- Amiodaron in atrial fi brillation: post coronary artery bypass graft
- Short lessons in basic life support improve self-assurance in performing cardiopulmonary resuscitation
- Is current training in basic and advanced cardiac life support (BLS & ACLS) effective? A study of BLS & ACLS knowledge amongst healthcare professionals of North-Kerala
- Effects of a general practitioner cooperative co-located with an emergency department on patient throughput
- Acute Care/Trauma Surgeon's role in obstetrical/ gynecologic emergencies (The OBCAT Alert)