The Buffering analysis to identify common geographical factors within the vicinity of severe injury related to motor vehicle crash in Malaysia
2016-11-23NikHisamuddinRahmanRuslanRainisSyedHatimNoorSharifahMasturaSyedMohamad
Nik Hisamuddin Rahman, Ruslan Rainis, Syed Hatim Noor, Sharifah Mastura Syed Mohamad
1Department of Emergency Medicine, School of Medical Sciences, University Sains Malaysia, Kota Bharu 16150, Malaysia
2School of Humanity, University Sains Malaysia, Penang, Malaysia
3Unit of Biostatistics, School of Medical Sciences, University Sains Malaysia, Kota Bharu 16150, Malaysia
4Unit of Health Informatics, School of Health Sciences, University Sains Malaysia, Kota Bharu 16150, Malaysia
Corresponding Author: Nik Hisamuddin Rahman, Email: nhliza@hotmail.com
The Buffering analysis to identify common geographical factors within the vicinity of severe injury related to motor vehicle crash in Malaysia
Nik Hisamuddin Rahman1, Ruslan Rainis2, Syed Hatim Noor3, Sharifah Mastura Syed Mohamad4
1Department of Emergency Medicine, School of Medical Sciences, University Sains Malaysia, Kota Bharu 16150, Malaysia
2School of Humanity, University Sains Malaysia, Penang, Malaysia
3Unit of Biostatistics, School of Medical Sciences, University Sains Malaysia, Kota Bharu 16150, Malaysia
4Unit of Health Informatics, School of Health Sciences, University Sains Malaysia, Kota Bharu 16150, Malaysia
Corresponding Author: Nik Hisamuddin Rahman, Email: nhliza@hotmail.com
BACKGROUND: The main objective was to identify common geographical buildup within the 100-meter buffer of severely injured based on injury severity score (ISS) among the motor vehicle crash (MVC) victims in Malaysia.
METHODS: This was a prospective cohort study from July 2011 until June 2013 and involved all MVC patients attending emergency departments (ED) of two tertiary centers in a district in Malaysia. A set of digital maps was obtained from the Town Planning Unit of the district Municipal Offi ce (local district map). Vector spaces were spanned over these maps using GIS software (ARCGIS 10.1 licensed to the study center), and data from the identified severe injured cases based on ISS of 16 or more were added. Buffer analysis was performed and included all events occurring within a 100 -meter perimeter around a reference point.
RESULTS: A total of 439 cases were recruited over the ten-month data collection period. Fifty two (11%) of the cases were categorized as severe cased based on ISS scoring of 16 and more. Further buffer analysis looking at the buildup areas within the vicinity of the severely injured locations showed that most of the severe injuries occurred at locations on municipal roads (15, 29%), straight roads (16, 30%) and within villages buildup (suburban) areas (18, 35%).
CONCLUSION: This study has successfully achieved its objective in identifying common geographical factors and buildup areas within the vicinity of severely injured road traffi c cases.
Motor vehicle crash; Emergency department; Injury severity score
World J Emerg Med 2016;7(4):278–284
INTRODUCTION
Identifying risk factors for seriously injured victims is crucial in implementing the primary prevention especially in regards to geographical buildup factors common to the accident sites involving critically injured road users.[1]In the past, too much of prevention is focused on general minimally injured population, which can cost millions and increase economic burden on developing countries. Few studies had indicated that pattern of road traffi c injury (RTI) is significantly influenced by geographical lay out and its surrounding buildup.[2,3]Therefore the investigator planned to conduct a research with a primary objective to identify hotspot areas and geographical buildup within the vicinity of severely injured victims of road traffic accidents. The severely injured population was chosen because it involved more of productive young road userswho are crucial for socioeconomic status of the country. Such identification would promote a more focused primary prevention for those regions that are facing with ever-increasing fi nancial crisis. It will create a much safer environment for vulnerable road users and hence reduces the socioeconomic burden of the country.
METHODS
This was a prospective cohort study from July 2011 until June 2013. It involved all MVC patients attending the emergency departments (ED) of two tertiary centers in a district in Malaysia. The Kota Bharu district on the East Coast of Peninsular of Malaysia was chosen because it was known for high prevalence of road traffi c injuries. The study sample included all patients with road-related injuries within the study district who attended the two EDs. Consent was taken from each patient or relative by using standard consent form approved by Ethical Committee of the main study center. By using a two proportion sampling, alpha value of 0.05, power of study 80% and 20% drop out, the required sample size of road traffic accident victims was 415 based on a study done by Abdul Razak in Karachi Pakistan.[4]
For this study, the investigator extracted age, gender, accident mechanisms and causes, and vehicle types from the police & hospital management and outcome. A set of digital maps (road and borough layers) was obtained from the Town Planning Unit of the district Municipal Office (local district map). Vector spaces were spanned over these maps using GIS software (ARCGIS 10.1 licensed to the study center), and data from the identifi ed trauma cases were added. Spatial analysis and overlay tools were used to identify local clusters of events. Buffer analysis was performed and included all events occurring within a 100-meter perimeter around a reference point (Figure 1). The investigators asked the prehospital care providers and patients or relatives to specifi cally identify and draw the map location of the RTI. The researcher attended each of the location of incidence and obtained x and y GIS coordinate in degree, minute and second in WGS 84 format by using a hand held GPS unit brand Garmin model GPS 72H with Serial number 1T7071348 (Manufactured in Taiwan by Garmin Corporation in 2010) which was accurate to 5 meters of the location. The land use and type of buildings within the 100-meter buffer region for each accident point were identified from both the “land use“ digital map layer provided and also from the free open software Google earth view version 7.1.2.2041 operating system Microsoft Windows (5.1.2600.3) (Figure 2). Digital photos were also taken and kept in file. The investigators performed specific geospatial analysis on severely injured victims based on injury severity score (ISS) of 16 and more.
The exclusion criteria included missing or unable to detect the exact location and coordinate (Latitude and Longitude) of RTI, injury treated in hospitals other than the two study hospitals, injury caused by other events i.e. domestic violence or assault and no clinical outcome data available. This was the very first buffer analysis study carried out in the country in relation to clinical severity as outcome. The author also could not find any article published related to 100-meter buffer analysis for severe cases (based on ISS) related to RTI.

Figure 1. The 100-meter buffer for each accident point.
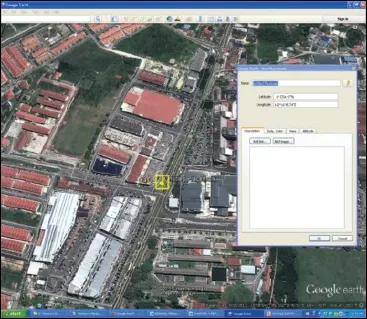
Figure 2. The Google Earth analysis of geographical build up for each MVC point.

Figure 3. The mapping of the coordinate locations for RTI cases.

Table 1. Cases with missing data, which were excluded from the epidemiological analysis

Table 2. The distribution of the initial vital signs on arrival in ED and injury score based on fi nal diagnoses

Table 3. The common geographical buildup within the 100-meter buffer area of the RTI locations based on the coordinates obtained
RESULTS
A total of 439 cases were recruited over the tenmonth data collection period from August 2012 till May 2013. The variables collected were divided into general demography, prehospital, clinical and geographical data. However there were 27 cases with missing data, which were excluded from the epidemiological analysis (Table 1). The mean age (SD) of the RTI victims was 26.04 years (SD 15.26). The range of age was between 2 to 81 years of age. Age (in years) groupings for the RTI victims were less than 13 (4.4%), 13 to 19 (35%), 20 to 40 (41.4%) and older than 40 (18.4%). There were 302 (71.7%) males. Motorcyclists (351, 80.0%) were the most common type of victim involved, which comprised of 87% (305) male riders followed by car occupants (55, 12.5%). A total of 49 (11.2%) of the cases resulted from spontaneous skid and falls without any two vehicle impact. Table 2 shows the distribution of the initial vital signs on arrival in ED and injury scoring based on fi nal diagnoses.
The majority of the RTI occurred on the municipal roads (310, 73.3%) within the district of interest. The mapping of the coordinate locations for all the RTI cases within the study period was plotted as shown in Figure 3 based on the borough and road network layers. Table 3 shows the common geographical buildup within the 100-meter buffer area of the RTI locations based on the coordinates obtained. Fifty-two (11%) of the cases werecategorized as severe based on ISS scoring of 16 or more. Interestingly, the majority of the severely injured victims sustained the RTI on roads with maximum speed limit of 60 km/hour (38, 73%) whereas only ten (19%) cases of the severely injured victims occurred on the roads with maximum speed limit of 90 km/hour. Further buffer analysis looking at the buildup areas within the vicinity of the severely injured locations showed that most of the severe injuries occurred at locations on municipal roads (15, 29%), straight roads (16, 30%) and within villages (suburban) areas (18, 35%). Both adult and pediatric age group victims showed similar geographical distribution. However most of the children (less than 18 years) sustained the RTI within the vicinity of primary schools and on straight roads.
DISCUSSION
RTI is the eighth leading cause of death internationally, and the leading cause of death for young people aged 15–29. Current trend suggests that by 2030 road traffic deaths will become the fifth leading cause of death unless urgent action is taken. According to the Ministry of Health Malaysia's data in 2013, accident due to motor vehicle crash (MVC) was ranked as the fourth most common cause of hospital admissions and fi fth cause of death in the country.[5–7]
The study has shown similar trend in the prehospital and clinical parameters of the RTI victims to the nationwide and international data in particular data originating from the developing countries.[8,9]The victims commonly involved the young age group (40% at between 20 to 40 years of age), the age at which the general population is very productive socioeconomically. Sadly, a significant number of the victims were among the school-aged population ranging from primary schools to the late adolescent (28%). There were significantly more male MVC victims compared to the female. Young age and male are both common denominators in MVC cases worldwide. These two factors are strongly related to psychosocial contributions towards involving in challenging and risky behaviors on the road. Furthermore, the cultural pattern within the study locations showed more men ride motorcycles compared to women. Women tend to be pillion riders to their spouses. A study by Malaysia Institute Research For Road Safety (MIROS) in 2006 indicated that women and elderly population tend to ride less motorcycles compared to men and the young age group respectively.[10]The risky behavior such as speeding, showing off stunt actions, illicit drug influence and driving without safety equipment commonly result in disastrous outcomes on the road.[11,12]A similar trend of young age and male preponderance was found in Singapore data on road fatalities from year 2000 to 2004. As in other middle and low-income countries, the most common type of vehicle involved was two wheelers (motorcycles) and cars (80% and 12% respectively). Numerous other similar findings were published on the risk factors of a two-wheeler involvement in the MVC resulting either in severe injuries or deaths worldwide.[13–15]Malaysian Institute of Research on Road Safety (MIROS) reported that over the 10-year period (2000–2010), an estimated 1.2%–1.5% of the registered motorcycles in Malaysia were involved in accidents. In 2010 alone, out of the 120 156 motorcycle accidents, there were 3 614 driver and 422 pillion rider fatalities. This gives the fatality index (i.e. number of fatalities per road accidents) of 0.03 and 0.003 for riders and pillions respectively.[16]
The investigators also noted that ISS among the victims in suburban area was significantly higher than those in the urban area. Many factors contributed to this signifi cant clinical fi nding such as speeding that is more common in the suburban area due to less traffic density and straighter roads with fewer intersections. In addition there were many motorcyclists who show high-risk behavior on the roads within this area such as young age, no driving license, not wearing safety helmet and illegal racing. Poor enforcement by the police and road safety officer also contributed to the high-risk behaviors as mentioned above.[17,18]Most of the literatures mentioned about well-established factors that determine the clinical outcome such as[19,20]: 1) inadequate in-vehicle crash protection; 2) inadequate roadside protection; 3) the nonuse of protective devices in vehicles; 4) the non-use of protective crash helmets; 5) excessive and inappropriate speed; 6) the presence of alcohol.
In this study, majority of the RTI cases of all categories (ISS>16, polytrauma, disabled, operated cases) occurred on the road with maximum speed limit of 60 km/hour. This road network is mainly located in the suburban area. Much less severe categories of injured victims occurred on the road with maximum speed limit of 35 km/hour. Collectively, more severe categories of MVC cases occurred on roads with higher maximum speed limits (60 & 90 km/hour) compared to those that occurred on the road with speed limit of 35 km/hour. Even though the investigators were unsure of the actual vehicle speed at the time of every impact, it can be concluded that the road users tend to drive faster on anyroads with higher speed limits and hence increase the risk of MVC.[21,22]Unfortunately in this study, the attempt to obtain reliable data on speed of vehicles at the onset of accident was diffi cult and unreliable partly due to the road users unwillingness to disclose the speed.
Nowadays many highway and road safety agencies have been using GIS system for analyzing road related accidents.[23]The process in identifying the environmental factors that contribute to any MVC is crucial and may serve as a corrective measure to prevent similar incidenst in future. When using the system, the user can merge the MVC cases and road infrastructure data and also match the MVC cases with locations buildup. There is a need to obtain accurate information on the circumstances of every collision, especially with regard to location in order to get a general relation of severity of road related injuries with the environment buildup. In this study, the investigators have carried out detail analysis of the environment buildup at each of the MVC location by using proximity analysis buffer technique from ARCGIS software. This study found that the cases with severe ISS (more than 16) matched with cases mostly at the location similar to polytrauma cases. The two common locations were at major intersections of Borough Kenali and Binjai. These two areas are well known to have high vehicle density and vulnerable road users including motorcyclists, pediatric pedestrian and school children. The maximum speed limit within these areas is 60 km/hour. The fact that these roads are normally congested and contain high vehicular density, the risk factors such as vulnerable road users and human attitude have contributed to signifi cant adverse outcome. There were cases in this study that involved underage motorcyclists (both pillion and main riders) who sustained injuries after illegal motorcycle racing on the road in particular long stretch straight road with maximum speed limit of 90 km/hour. Similar geographical pattern was seen in the USA where forty percent of all traffi c fatalities occur in urban areas, the percentage increases to 63 percent in an area that also included the rural area within 2.5 miles of the urban boundary. The percentage increased to 73 percent 5.0 miles out, 81 percent 7.5 miles out, and 86 percent 10 miles out.[24]
The underage motorcyclists and speeding tend to be seen in the suburban and village areas. The enforcement is lacking and the relative low density of vehicles on the road attract drivers to speed. Many of these vulnerable road users did not wear protective helmets based on the report obtained from the ambulance paramedics attending the victims, history from patients and witnesses. Furthermore the distance from the tertiary hospitals resulted in the delay in ambulance arrival and hence delayed ED treatment. A study done by Abdul Manan in 2012 on road fatalities among motorcyclist in Malaysia has shown that 60% of the fatalities occurred on the roads in non-busy areas such as suburban and rural locations. They also found that the majority were young riders (89%), 16 to 20 years old (22.5%), and 90% of the motorcycles were privately owned.[25]Interestingly the east coast region in Malaysia, with a lower motorcycle population and less built-up density, has the highest fatality rate per 10 000 motorcycles. Meanwhile, the Federal Territories, which have the highest population density, record the lowest rate in motorcycle fatality per 10 000 registered motorcycles.[26]Commonly we see that the occurrence of polytrauma cases at the site connecting two major towns. The road which is straight, wide, and traverses through village housing is commonly used by heavy vehicles such as lorries and trucks with the presence of vulnerable road users such as pedestrian, children and motorcyclists among the villagers. The common maximum speed limit within this area is 60 km/ hour, which is high enough to cause significant clinical injuries or death upon impact on other vehicle or human body. Less vehicle density and straight road have always contributed to the urge for drivers to speed at this area and hence increase the risk of MVC. Another signifi cant factor that contributed to severe impact on road users is the quality of road barriers and guardrail. A study carried out at other locations in the country has found that the impact on vehicles and the occupants was partly affected by the type of guardrail installed alongside the roads.[27]
Overall this study has successfully achieved its objectives in identifying geographical factors that are commonly found at locations of severely injured victims related to MVC. The identifi cations of these factors can be utilized further by agencies and government authority interested in focusing implementation of primary prevention against severe injuries related to road traffi c. By focusing on this group of road victims, more fi nancial and manpower resources can be utilized effectively to curtail severe MVC cases and hence prevent unnecessary use of money in providing long term management of critically injured road users. The potential for GIS in RTI research is very promising and great because it has capability in linking display data with health and injury data. Road traffic injuries can be envisaged in relationship to the health care provision, environmental factors and description to sociocultural aspects of the population involved. Therefore, we would like to suggestfew improvements in conducting similar research effort in future:
i. The GIS analysis on road safety should be made much wider, not only in the urban area but also the rural area so that we can see the total spectrum of the injury problem. A comparison can be made with rural area and this will provide a much better preventive strategies to the authority in future.
ii. An integrated data source will be a much better way to conduct such study. It will be ideal if police and health data can be integrated into one system and this can be utilized further for road safety research. Injury outcomes analysis can be improved if pre-hospital, hospital data and injury data are organized into one system. The database system must have geographical component as well to support the Haddon Matrix concept in injury prevention. However this data combination must have common and standardize defi nition, which can be comprehended and made available by many agencies for the purpose of research and audit.
iii. It would be ideal in future, for our setting, if GIS technique can be utilized in specific area of RTI research such as: determination of network of ambulance transportation for trauma cases; pediatric pedestrian injuries specifi cally targeting the school children; cyclist injuries; death related RTI; injury specific analysis which is common in Malaysia i.e traumatic brain injury, orthopedic injury, maxillofacial injury, abdominal injury; Geriatric injury on the road; heavy vehicle and public transportation related MVC and injuries.
Limitations of the study
This study was also subjected to a few limitations. The fundamentals of this study required the exact location of the MVC occurrence for the hotspot analysis. The majority of the latitude and longitude readings were taken by the paramedics who attended the cases with five to ten-meter accuracy; however, there was a small proportion of the self-attended cases which we had to rely on the graphical drawing of the exact location by the victims or relatives and retrieval of the coordinates was done retrospectively by the researcher. The confi rmation of these locations was made by asking the witness at the site and by locating the traces of the MVC such as broken glasses and vehicle parts at the sites. One of the striking fi ndings that was also a limiting factor of this study was the involvement of motorcyclists in the majority of MVC cases. Investigators were hoping the analysis would have covered for all types of the road users but unfortunately it was skewed mainly for two-wheeler users. This is unavoidable as the same pattern of MVC involvements throughout developing countries especially within the urban and suburban areas has been reported in journals and government websites. However this would not alter the ultimate objective of the study to look at the hotspot analysis and clinical outcome rather than the mechanism of injury. In addition, the investigators were unable to determine the exact cause of MVC (i.e. illicit drug taking or mechanical cause) due to unreliable sources of information from the witnesses.
In conclusion, this study has successfully achieved its objective in identifying common geographical factors and buildup areas within the vicinity of severely injured road traffi c cases. Investigators are hoping that this data can be utilized further for the implementation of focused primary prevention to curtail severe injuries on the road and hence reduce the economic burden of RTI in developing country. A bigger scale of geospatial buffer analysis in future will provide a more general conclusive data for nationwide use.
ACKNOWLEDGEMENT
The authors thank the emergency departments staff of USM and HRPZ (2) who have assisted in the data collection and the USM research management office who has awarded the RU (I) research grant for this research project.
Funding: None.
Ethical approval: The study was approved by the Ethical Committee of the main study center.
Conflicts of interest: The authors declare no conflict of interest during the preparation, conduct and submission of the manuscript. Contributors: Rahman NH conceived the study, collected the data and prepared the manuscript. Rainis R conceived the study. Noor SH provided statistical advice on study design and analyzed the data. All authors contributed substantially to its revision. Mohamad SM takes responsibility for the paper as a whole.
REFERENCES
1 Hyder AA, Vecino-Ortiz AI. BRICS: opportunities to improve road safety. Bull World Health Organ 2014; 92: 423–428.
2 Elias W, Shiftan Y. Analyzing and modeling risk exposure of pedestrian children to involvement in car crashes. Accid Anal Prev 2014; 62: 397–405.
3 Hobday M, Knight S. Motor vehicle collisions involving child pedestrians in eThekwini in 2007. J Child Health Care 2010; 14: 67–81.
4 Abdul Razak J. Application of Geographical Information System (GIS) for mapping road traffic injuries using existing source of data in Karachi, Pakistan — A pilot study. J Pak Med Assoc 2011; 61: 640–643.
5 Health Facts 2012 by The Ministry of Health Malaysia. Available at http://www.moh.gov.my/images/gallery/stats/heal_fact/health_ fact_2012_page_by_page.pdf in January 2015. [Accessed online on 4th March 2015]
6 Ahmad R, Rahmat R, Hisamudin N, Rahman NA, Noh AY, Mohammad N, et al. Demographic and clinical characteristics of red tag patients and their one-week mortality rate from the emergency department of the Hospital Universiti Sains Malaysia. Southeast Asian J Trop Med Public Health 2009; 40: 1322–1330.
7 Umar RS. Motorcycle safety programs in Malaysia: how effective are they? Int J Inj Contr Saf Promot 2006; 13: 71–79.
8 Chekijian S, Paul M, Kohl VP, Walker DM, Tomassoni AJ, Cone DC, et al. The global burden of road injury: its relevance to the emergency physician. Emerg Med Int 2014; 139219. Epub 2014 Jan 21.
9 Chalya PL, Mabula JB, Dass RM, Mbelenge N, Ngayomela IH, Chandika AB, et al. Injury characteristics and outcome of road traffi c crash victims at Bugando Medical Centre in Northwestern Tanzania. J Trauma Manag Outcomes 2012; 6: 1.
10 MIROS: Report on Mode of Choice for Vulnerable Motorcyclists in Malaysia. Available at http://www.miros.gov. my/1/publications.php/id_page=23&id_event=358. Accessed on 20th April 2016.
11 Summala H, Rajalin S, Radun I. Risky driving and recorded driving offences: a 24-year follow-up study. Accid Anal Prev 2014; 73: 27–33.
12 Constantinou E, Panayiotou G, Konstantinou N, Loutsiou-Ladd A, Kapardis A. Risky and aggressive driving in young adults: Personality matters. Accid Anal Prev 2011; 43: 1323–1331.
13 Blackman RA, Haworth NL. Comparison of moped, scooter and motorcycle crash risk and crash severity. Accid Anal Prev 2013; 57: 1–9.
14 Albalate D, Fernández-Villadangos L. Motorcycle injury severity in Barcelona: the role of vehicle type and congestion. Traffi c Inj Prev 2010; 11: 623–631.
15 Munivenkatappa A, Devi BI, Gregor TI, Bhat DI, Kumarsamy AD, Shukla DP. Bicycle accident-related head injuries in India. J Neurosci Rural Pract 2013; 4: 262–266.
16 Ramli R, Oxley J, Hillard P, Mohd Sadullah AF, McClure R. The effect of motorcycle helmet type, components and fi xation status on facial injury in Klang Valley, Malaysia: a case control study. BMC Emerg Med 2014; 3: 14–17.
17 Tohira H, Jacobs I, Mountain D, Gibson N, Yeo A. Systematic review of predictive performance of injury severity scoring tools. Scand J Trauma Resusc Emerg Med 2012; 20: 63.
18 Boufous S, Finch C, Hayen A, Williamson A. The impact of environmental, vehicle and driver characteristics on injury severity in older drivers hospitalized as a result of a traffi c crash. J Safety Res 2008; 39: 65–72.
19 Zambon F, Hasselberg M. Factors affecting the severity of injuries among young motorcyclists--a Swedish nationwide cohort study. Traffi c Inj Prev 2006; 7: 143–149.
20 Moini M, Rezaishiraz H, Zafarghandi MR. Characteristics and outcome of injured patients treated in urban trauma centers in Iran. J Trauma 2000; 48: 503–507.
21 Gururaj G, Uthkarsh PS, Rao GN, Jayaram AN, Panduranganath V. Burden, pattern and outcomes of road traffi c injuries in a rural district of India. Int J Inj Contr Saf Promot 2014; 11: 1–8.
22 Aarts L, van Schagen I. Driving speed and the risk of road crashes: a review. Accid Anal Prev 2006; 38: 215–224.
23 Weiner EJ, Tepas JJ. Application of electronic surveillance and global information system mapping to track the epidemiology of pediatric pedestrian injury. J Trauma 2009; 66 (3 Suppl): S10–16.
24 Rakauskas ME, Ward NJ, Gerberich SG. Identification of differences between rural and urban safety cultures. Accid Anal Prev 2009; 41: 931–937.
25 Abdul Manan MM, Várhely A. Motorcycle fatalities in Malaysia. IATSS Research 2012; 36: 30–39.
26 Oxley J, Ravi MD, Yuen J, Hoareau E, Hashim HH. Identifying contributing factors to fatal and serious injury motorcycle collisions involving children in Malaysia. Ann Adv Automot Med 2013; 57: 329–336.
27 Mehrtash S, Taher BM, Mohamed RK, Ramli S. The safety performance of guardrail systems: review and analysis of crash tests data. International Journal of Crashworthiness 2013; 18: 530–543.
Accepted after revision April 25, 2016
10.5847/wjem.j.1920–8642.2016.04.007
Original Article
December 13, 2015
杂志排行
World journal of emergency medicine的其它文章
- The state and future of emergency medicine in Macedonia
- Amiodaron in atrial fi brillation: post coronary artery bypass graft
- Short lessons in basic life support improve self-assurance in performing cardiopulmonary resuscitation
- Is current training in basic and advanced cardiac life support (BLS & ACLS) effective? A study of BLS & ACLS knowledge amongst healthcare professionals of North-Kerala
- Effects of a general practitioner cooperative co-located with an emergency department on patient throughput
- Acute Care/Trauma Surgeon's role in obstetrical/ gynecologic emergencies (The OBCAT Alert)