肩峰指数与运用Multiloc髓内钉治疗肱骨近端骨折的临床相关性研究
2016-06-27邹义源向明李一平杨国勇陈杭胡晓川
邹义源 向明 李一平 杨国勇 陈杭 胡晓川
·论著·
肩峰指数与运用Multiloc髓内钉治疗肱骨近端骨折的临床相关性研究
邹义源1向明2李一平2杨国勇2陈杭2胡晓川2
目的 评估肩峰指数(acromionindex,AI)与Multiloc髓内钉治疗肱骨近端骨折的相关性。方法 将2014年2月至2015年6月,四川省骨科医院采用Multiloc髓内钉治疗17例肱骨近端骨折患者的病例资料纳入研究。其中男6例,女11例;年龄48~67岁,平均61.4岁;AI为0.69~0.94,平均0.78,其中男0.66,女0.75。根据Neer分型,二部分骨折8例(47%),三部分骨折7例(41%),四部分骨折2例(12%),其中合并有鹰嘴骨折、桡骨远端骨折、肩袖损伤及腋神经损伤。所有患者均为闭合性骨折。记录手术时间,出血量,术后1、2、4、6、8、12个月门诊定期复查,X线检查复位效果及愈合情况,并采用美国肩肘外科协会评分(ratingscaleoftheAmericanshoulderandelbowsurgeons,ASES),Constant评分等指标评价患者肩关节功能。结果 17例患者均顺利完成手术,1例术后出现肘关节僵硬,术后并发症发生率为5.8%。ASES评分中:总分P=0.670,疼痛P=0.078,生活功能P=0.010;Constant评分中:总分P=0.019,疼痛P=0.083,功能活动P=0.453,肩关节活动度P=0.007,力量P=0.869;出血量P<0.001;骨折愈合时间P=0.001;手术时间P=0.866。日常活动中:前屈上举P=0.012,外展P=0.010,外旋P=0.038。6例男性平均AI为0.66±0.54,11例女性平均AI为0.75±0.40,两者AI相比P=0.218。提示AI与患者术中出血量、骨折愈合时间及术后功能活动(特别是前屈上举、外展、外旋)有相关性。结论 肱骨近端骨折运用髓内钉治疗时,AI大小与性别、年龄、手术时间无明显相关性。AI越小,术中出血量越少,骨折愈合时间越短;AI越大,术中出血量相对较多,骨折愈合时间稍长。AI较大的患者,术后ASES评分及Constant评分较高,术后功能活动(前屈上举、外展及外旋)较好;相反,AI较小的患者,术后ASES评分及Constant评分相对较低,术后功能活动(前屈上举、外展及外旋)相对较差。在运用Multiloc髓内钉治疗肱骨近端骨折时,暂未发现与手术相关并发症,且AI的大小与术后并发症的发生无明显相关性。
肩峰指数;肱骨近端骨折;髓内钉
肱骨近端骨折属于骨科临床常见病种,其发生率占所有骨折的4%~5%[1],超过70%的肱骨近端骨折发生于60岁以上老年人,其发生趋势随着我国老龄化的到来,将会逐年递增。其中多数肱骨近端骨折可以通过保守治疗,能够获得较好的临床功能预后[2-3],但仍存在一定的并发症。肱骨近端骨折手术治疗方式包括:闭合或切开复位内固定和肩关节置换。内固定的选择多样,如Multiloc髓内钉[4-6]。
在Multiloc髓内钉治疗的手术过程中,Rispoli等[7]发现肩峰指数(acromionindex,AI)的大小对手术有影响,但目前国内尚无相关的文献报道。故本文假设AI的大小与肱骨近端骨折运用Multiloc髓内钉治疗时,在手术时间、术中出血量、骨折愈合时间、术后功能评分及功能恢复上有差异。本研究回顾性分析2014年2月至2015年6月四川省骨科医院应用Multiloc髓内钉治疗肱骨近端骨折17例患者的病例资料,并记录手术时间、出血量、骨折愈合时间、术后功能恢复及功能评分等。
资 料 与 方 法
一、一般资料
2014年2月至2015年6月本院应用Multiloc髓内钉治疗且随访1年的肱骨近端骨折患者17例,男6例,女11例;年龄48~67岁,平均61.4岁;AI为0.69~0.94,平均0.78,其中男0.66,女0.75。根据Neer分型,二部分骨折8例(47%),三部分骨折7例(41%),四部分骨折2例(12%),其中合并有鹰嘴骨折、桡骨远端骨折、肩袖损伤及腋神经损伤。17例患者中优势手受伤8例(47%),非优势手受伤9 例(53%)。患者受伤原因:走路滑倒摔伤9例(53%),自行车摔伤5 例(29.4%),交通事故3 例(17.6%)。所有骨折均为闭合性骨折。本研究获得医院伦理委员会批准,所有受试者均签署知情同意书。
二、随访及评价指标
手术均由同一组医师完成,由另外2名高年资骨科医师进行门诊随访和评价。患者出院后门诊密切随访,术后1、2、4、6、8、12个月定期复查,拍摄DR片。记录手术时间、出血量、骨折愈合情况及功能活动情况等。采用肩关节活动度、美国肩肘外科协会评分(ratingscaleoftheamericanshoulderandelbowsurgeons,ASES)[8]、Constant肩关节评分评估肩关节功能[9]。ASES评分为美国肩肘外科协会制定的肩关节功能评价标准,包括疼痛(50%)和生活功能(50%),满分为100分,分数越高表示肩关节功能越好。Constant肩关节评分系统满分为100分,由疼痛(15分)、肌力(25分)、功能活动(20分)及肩关节活动度(40分)4个子量表组成,分数越高,表示肩关节功能越好。
三、AI的测量
所有患者均拍摄标准肩关节正位、侧位及腋位片,采用盲法由1名有丰富经验的高年资放射科医师完成。由2名上肢科医师分别测量肩峰外侧缘至肩关节盂平面的距离和肱骨头外端外侧缘至肩关节盂平面距离,结果取两人平均值,且使用图像均由院内图片存档及通信系统(picturearchivingandcommunicationsystems,PACS)提供,避免不同设备和技术人员导致的测量误差。
四、统计学分析
采用SPSS22.0统计软件,患者性别使用独立样本t检验,Neer二部分、三部分、四部分骨折患者肩关节功能、出血量、手术时间、骨折愈合时间、ASES评分及Constant评分采用直线相关分析。检验水准α值取双侧0.05。P<0.05为差异有统计学意义。
结 果
一、一般结果
ASES评分:总分P=0.670,疼痛P=0.078,生活功能P=0.010;Constant评分:总分P=0.019,疼痛P=0.083,功能活动P=0.453,肩关节活动度P=0.007,肌力P=0.869;出血量P<0.001;骨折愈合时间P=0.001;手术时间P=0.866。日常活动:前屈上举P=0.012,外展P=0.010,外旋P=0.038。6例男性平均AI为0.66,11例女性平均AI为0.75,两者比较P=0.218,见表1。
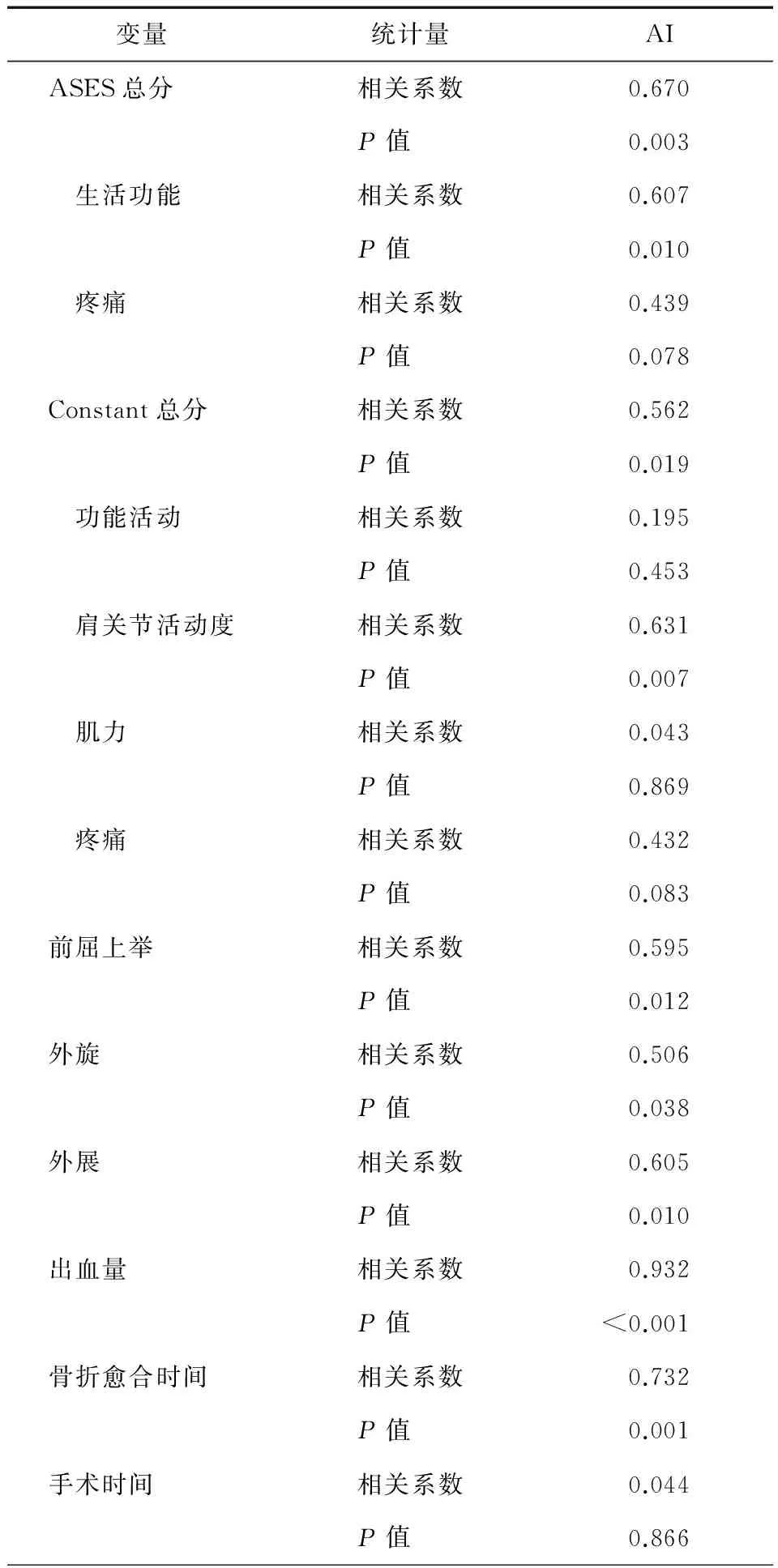
表1 AI指数与Multiloc髓内钉治疗肱骨近端骨折的统计学结果
注:AI为肩峰指数;ASES为美国肩肘外科协会评分
AI较小(<0.68)的患者5例,其中Neer二部分骨折1例,三部分骨折3例,四部分骨折1例。平均年龄55.8岁(43~69岁),平均AI0.55(0.47~0.66);术中出血量平均110ml(100~150ml);前屈上举角度平均146°(120°~170°),外旋角度平均36°(30°~40°),外展角度平均88°(80°~110°);术后ASES评分平均83.8分(80~90分),Constant评分平均81分(76~91分);骨折愈合时间平均1.6个月(1.5~2个月)。
AI较大(>0.68)的患者12例,其中Neer二部分骨折7例,三部分骨折4例,四部分骨折1例。平均年龄61.4岁(48~69岁),平均AI0.78(0.69~0.94);术中出血量平均为257.5ml(150~300ml);前屈上举角度平均161.6°(120°~180°),外旋角度平均40°(20°~50°),外展角度平均106.5°(85°~160°);术后ASES评分平均89.7分(80~96分),Constant评分平均87.3分(79~98分);骨折愈合时间平均2.25个月(1.5~3个月)。
二、术后并发症
至末次随访,17例患者中无医源性神经、血管损伤,无一例出现切口感染,无内固定物松动断裂失效,无肱骨头坏死发生。1 例患者出现同侧肘关节僵硬活动障碍(屈110°,伸50°),但无肌力减弱、肌肉萎缩或其他神经损害表现,考虑与3 个月未能按时门诊随访及康复治疗有关,Multiloc髓内钉固定术后1年行肘关节松解术,术后肘关节功能得到明显恢复(屈130°,伸10°)。AI的大小与患者术后是否出血并发症并无明显相关性。
讨 论
肱骨近端骨折大部分是闭合性骨折,且绝大多数稳定的轻度或无移位骨折可以采取非手术治疗[10],然而有15%~64%的肱骨近端骨折是移位型骨折,需要手术治疗。如采取非手术治疗,其并发症如骨折畸形愈合、骨折不愈合、肩关节僵硬以及创伤后肩关节炎等[10-11]。
本组在治疗肱骨近端骨折时选用Multiloc髓内钉[4-5]。术中沙滩椅位,通过三角肌前束与中束之间,劈开三角肌,必要时分离保护腋神经。通过强生5#线牵拉或带螺纹克氏针做Joy-stick技术复位骨折块。理想的髓内钉进针点为:肱骨头顶端,肱二头肌腱后外侧,大结节和肱骨头之间的沟内侧,冈上肌肌腱止点内侧1~1.5cm处。恰当的进针点将决定了复位的结果,而不恰当的进针点将直接导致复位不良[12]。此时需术中探查肩袖,若肩袖撕裂,可适当沿长破口选择进针;若肩袖完整,可沿冈上肌肌纤维方向作约1cm小切口。导针位置确认后,插入组装Multiloc髓内钉,C臂透视再次确认髓内钉位置。依据骨折类型,在近端选用3枚以上4.5mm螺钉及数枚3.5mm钉中钉增加肱骨头及后内侧区把持力[13-14],根据需要选择4mm上升螺钉对肱骨距进行支撑[15-16],远端用1或2枚4mm锁定螺钉固定,以减少髓内钉在髓腔内摆动。最后选用Orthocord线或强生5#线修复肩袖。此入路会不可避免损伤肩袖,Park等[17]指出虽然髓内钉治疗肱骨近端骨折患者术后可能出现肩关节疼痛和活动受限,是否与切开肩袖有关存在争议,但实际上是医师术中对肩袖处理不当所致。
AI这一概念首先由Nyffeler等[18]提出,它直接反映了肩峰横向延展度。肩峰向外侧延伸越长,AI越高。测量AI需要一张肩关节前后位X线片。具体方法是三条特殊的平行线之间的距离测定。第一条线连接肩胛盂的上皮质缘和下皮质缘的最边缘,第二条线平行于第一条线,与肩峰的最边缘相切;第三条线与此二线平行,与肱骨头的最边缘相切(图1)。
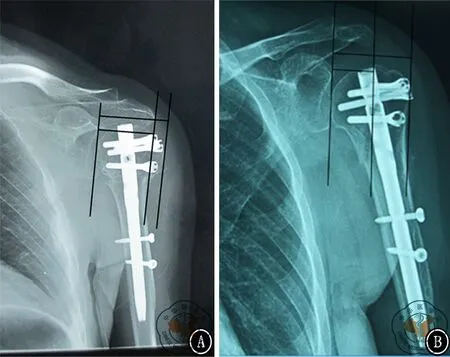
图1 AI指肩峰外侧缘至肩关节盂平面的距离与肱骨头外端外侧缘至肩关节盂平面距离的比值。图A肩峰覆盖较大,AI较高;图B肩峰覆盖较小,AI较低
有研究表明男女肩峰形态存在明显差异[11-20],在其研究中虽然右肩和左肩差异无统计学意义,但发现女性比男性更容易发病,原因是女性有更高的肩峰覆盖率,即AI高,并且AI的大小并不与年龄成正相关。
据Rispoli等[7]指出肩袖撕裂的程度与AI成正相关:肩袖全层撕裂患者的AI为0.73±0.06,而健康对照组AI为0.64±0.06。Hamid等[19]研究证实:肩袖损伤时AI为0.69±0.06。Torrens等[11]指出在肩袖损伤病例中AI的平均值为0.69(0.49~0.89)。Zumstein等[21]研究结果示:肩袖的损伤有些是两条肌腱的复合伤(平均AI为0.68,范围0.54~0.86),有的是三条肌腱的复合伤(平均AI为0.75,范围0.66~0.88),并且术后随访发现部分患者出现了肩袖再撕裂。而对比完全康复 (平均AI为0.65)和再撕裂 (平均AI为0.75)的患者,AI差异有统计学意义,即平均AI>0.68的患者其手术时间要比<0.68的患者较长,且出血量也较多。
Ames等[22]的研究结果显示:对比有较大AI与较小AI的患者,前者比后者更易患有2条及以上肩袖撕裂,术中需要更多的锚钉来修复肩袖,并且术后患者满意度较低。AI较大的患者对术者来说,是一种技术性挑战。患者术后恢复不太理想,虽可能与术者术中粗糙的缝合技术有关,但与AI的大小密切相关。对于AI较大的患者,术中为了达到理想锚钉置入点,需要助手协助从患者腋下横向外侧牵拉,人为降低AI,并使手术视野暴露更充分(图2)。

注:AI为肩峰指数;ASES为美国肩肘外科协会评分图3 AI大小与统计数据相关性。图A AI与 ASES生活功能评分相关性;图B AI与Constant肩关节活动度相关性;图C AI与术中出血量相关性;图D AI与肩关节外展角度相关性;图E AI与肩关节外旋角度相关性;图F AI与肩关节前屈上举角度相关性

图2 AI较大的患者为取得理想进针点,需人为牵拉肱骨近端。图A较大AI的患者,对于Multiloc进针点选择上非常困难;图B需要从腋窝处横向牵拉肱骨近端,人为减少AI,取得理想进针点
本研究中,在AI与肱骨近端骨折运用Multiloc髓内钉治疗时,笔者发现所有参与本研究的患者中,性别与肩峰大小差异无统计学意义(P>0.05)。AI较大的患者其术中出血量较AI较小的患者多,差异具有统计学意义(P<0.05)。虽然本研究中手术时间与AI在治疗肱骨近端骨折时,差异无统计学意义(P>0.05),但对于较大的AI患者,需要横向牵拉肱骨近端,以充分暴露髓内钉进针点。且术前怀疑患者合并肩袖损伤,也需充分显露术区才能发现并及时修补肩袖,这点对于患者预后相当重要(图2)。根据患者术后VAS、ASES、Constant功能评分显示,术后疼痛与AI大小差异无统计学意义(P>0.05),但在患者术后功能活动,如前屈上举、外展及外旋,AI越大,术后功能活动相对较好;相反,AI较小,术后功能活动,如前屈上举、外展及外旋反而较差(P<0.05),见图3。
结 论
肱骨近端骨折运用髓内钉治疗时,AI大小与性别、年龄、手术时间无明显相关性。AI越小,术中出血量越少,骨折愈合时间越短;AI越大,术中出血量相对较多,骨折愈合时间稍长。AI较大的患者,术后ASES评分及Constant评分较高,术后功能活动(前屈上举、外展及外旋)较好;相反,AI较小的患者,术后ASES评分及Constant评分相对较低,术后功能活动(前屈上举、外展及外旋)相对较差。在运用Multiloc髓内钉治疗肱骨近端骨折时,暂未发现与手术相关并发症,且AI的大小与术后并发症的发生无明显相关性。
[1]SüdkampN,BayerJ,HeppP,etal.Openreductionandinternalfixationofproximalhumeralfractureswithuseofthelockingproximalhumerusplate.Resultsofaprospective,multicenter,observationalstudy[J].JBoneJointSurgAm,2009,91(6):1320-1328.
[2]BurkhartKJ,DietzSO,BastianL,etal.Thetreatmentofproximalhumeralfractureinadults[J].DtschArzteblInt,2013,110(35-36):591-597.
[3]WidnallJC,DheerendraSK,MalalJJ,etal.Proximalhumeralfractures:areviewofcurrentconcepts[J].OpenOrthopJ,2013,7:361-365.
[4] 向明,胡晓川.Multiloc髓内钉内固定治疗肱骨近端骨折进展与展望[J/CD]. 中华肩肘外科电子杂志,2016,4(1):1-4.
[5] 杨国勇,向明,陈杭,等.Multiloc髓内钉治疗肱骨近端骨折的近期疗效[J].中华骨科杂志,2016, 36(2):103-112.
[6] 周君琳.肱骨近端骨折的交锁髓内钉治疗[J/CD].中华肩肘外科电子杂志,2015,1(2):51-56.
[7]RispoliDM,AthwalGS,SperlingJW,etal.Theanatomyofthedeltoidinsertion[J].JShoulderElbowSurg,2009,18(3):386-390.
[8]RichardsRR,AnKN,BiglianiLU,etal.Astandardizedmethodfortheassessmentofshoulderfunction[J].JShoulderElbowSurg,1994,3(6):347-352.
[9]ConstantCR,MurleyAH.Aclinicalmethodoffunctionalassessmentoftheshoulder[J].ClinOrthopRelatRes, 1987(214): 160-164.
[10]BiglianiLU,FlatowEL,PollockRG.Fracturesoftheproximalhumerus//RockwoodCAJr,GreenDP,BucholzRW.RockwoodandGreen′sfracturesinadults[M]. 4thed.Philadelphia:Lippincott-Raven, 1996: 1055-1107.
[11]TorrensC,LópezJM,PuenteI,etal.Theinfluenceoftheacromialcoverageindexinrotatorcufftears[J].JShoulderElbowSurg,2007,16(3):347-351.
[12]NodaM,SaegusaY,MaedaT.Doesthelocationoftheentrypointaffectthereductionofproximalhumeralfractures?Acadavericstudy[J].Injury,2011,42(4):35-38.
[13]StedtfeldHW,MittlmeierT.Fixationofproximalhumeralfractureswithanintramedullarynail:tippsandtricks[J].EurJTraumaEmergSurg,2007,33(4):367-374.
[14]LillH,HeppP,GowinW,etal.Age-andgender-relateddistributionofbonemineraldensityandmechanicalpropertiesoftheproximalhumerus[J].Rofo,2002,174(12):1544-1550.
[15]SchiumaD,PleckoM,KloubM,etal.Influenceofperi-implantbonequalityonimplantstability[J].MedEngPhys,2013,35(1):82-87.
[16]RuegerJM,RückerA,BriemD,etal.Proximalhumeralfractures:nailing[J].EurJTraumaEmergSurg,2007,33(4):357-366.
[17]ParkJY,PandherDS,ChunXY,etal.Antegradehumeralnailingthroughtherotatorcuffinterval:anewentryportal[J].JOrthopTrauma, 2008, 22(6): 419-425.
[18]NyffelerRW,WernerCM,SukthankarA,etal.Assoeiationofalargelateralextensionoftheacromionwithrotatorcufftears[J].JBoneJointSurg, 2006, 88(8): 800-805.
[19]HamidN,OmidR,YamaguchiK,etal.Relationshipofradiographicacromialcharacteristicsandrotatorcuffdisease:aprospectiveinvestigationofclinical,radiographic,andsonographicfindings[J].JShoulderElbowSurg,2012,21(10):1289-1298.
[20]SangiampongA,ChompoopongS,SangvichienS,etal.TheacromialmorphologyofThaisinrelationtogenderandage:studyinscapulardriedbone[J].JMedAssocThai,2007,90(3):502-507.
[21]ZumsteinMA,JostB,HempelJ,etal.Theclinicalandstructurallong-termresultsofopenrepairofmassivetearsoftherotatorcuff[J].JBoneJointSurgAm,2008,90(11):2423-2431.
[22]AmesJB,HoranMP,vanderMeijdenOA,etal.Associationbetweenacromialindexandoutcomesfollowingarthroscopicrepairoffull-thicknessrotatorcufftears[J].JBoneJointSurgAm,2012,94(20):1862-1869.
(本文编辑:胡桂英)
邹义源,向明,李一平,等.肩峰指数与运用Multiloc髓内钉治疗肱骨近端骨折的临床相关性研究[J/CD]. 中华肩肘外科电子杂志,2016,4(4):214-220.
CorrelationstudiesbetweenacromionindexandMultilocintramedullarynailinthetreatmentofproximalhumeralfracture
ZouYiyuan1,XiangMing2,LiYiping2,YangGuoyong2,ChenHang2,HuXiaochuan2.
1SouthwestMedicalUniversity,Luzhou646000,China;2DepartmentofUpperExtremityTraumatology,SichuanProvincialOrthopaedicHospital,Chengdu610041,China
XiangMing,Email:josceph_xm@sina.com
Background The proximal humeral fracture is a common clinical disease in the department of orthopedics, accounting for 4%-5% of all the fractures. More than 70% of the proximal humeral fractures occur in the elderly patients of over 60 years, and the number will increase year by year with the trend of population aging in China. The majority of proximal humeral fractures obtain good clinical prognosis through conservative treatment, but there are still some complications. The surgical treatment methods include close or open reduction and internal fixation and shoulder joint arthroplasty. The internal fixators are numerous, such as Multiloc intramedullary nail. During the intramedullary nailing treatment, Rispoli,etc. discovered the value of acromion index (AI) had an effect on the surgery, but no domestic literatures are reported at present. So this study assumes that the operation time, intraoperative blood loss, fracture healing time, postoperative functional scores and functional rehabilitation are different as the AI varies during the treatment of proximal humeral fractures with Multiloc intramedullary nail. In this study, seventeen patients of proximal humeral fractures were treated with Multiloc intramedullary nails from February 2014 to June 2015 in Sichuan provincial orthopedic hospital and the operation time, blood loss, fracture healing time, postoperative functional rehabilitation (anteflexion and uplift, internal and external rotation) and functional scores, etc. were recorded. All the clinical data were retrospectively analyzed to assess the correlation between AI and Multiloc intramedullary nailing in the treatment of proximal humeral fractures.Methods (1)General information.From February 2014 to June 2015, seventeen patients of proximal humeral fractures, including 6 males and 11 females were treated with Multiloc intramedullary nails and followed up for 1 year. The ages ranged from 48 to 67 years with 61.4 years on average. The AI ranged from 0.69 to 0.94 with 0.78 on average. The mean AI were 0.66 in male patients and 0.75 in females. According to Neer classification, there were 8 cases (47%) of 2-part fracture, 7 cases (41%) of 3-part fracture and 2 cases (12%) of 4-part fracture, including olecranon fracture, distal radius fracture, rotator cuff tear and axillary nerve injury. 8 cases (47%) were injured in the dominant sides and 9 cases (53%) were non-dominant sides. The causes were slips during walking in 9 cases (53%), falls from bicycles in 5 cases (29.4%) and traffic accidents in 3 cases (17.6%) and all the injuries were closed fractures. This research was approved by the hospital ethics committee and all the subjects signed the informed consents.(2)Follow-ups and evaluation index.All the operations were performed by physicians of the same group, and the follow-ups and assessments were conducted by another 2 senior orthopedic clinicians in the outpatient department. The postoperative routine visits were in the 1st, 2nd, 4th, 6th, 8th and 12th months and the X-ray radiographs were taken at the same time. The shoulder activity scale, rating scale of the American shoulder and elbow surgeons (AESE) and Constant scoring system were applied in the evaluation of shoulder function. ASES is made by the association of American shoulder and elbow surgeons, including pain (50%) and life function (50%). The total score is 100 points and the higher score indicates the better function. The Constant scoring system is composed of pain (15 points), muscle strength (25 points), functional activity (20 points) and range of motion of shoulder joint (40 points),and the total score is 100 points. The higher score reveals the better shoulder function as well. (3)AI measurement Standard.The X-ray radiographs of anteroposterior view, lateral view and axillary view were taken in all the patients by 1 senior and experienced radiologist with blind method. The respective distances from the lateral margin of acromion and the outer end of humeral head to the glenoid plane were measured by two physicians and the results were the mean values. All the radiographic images were provided by picture archiving and communication systems (PACS) in the hospital to avoid the measurement bias caused by different equipments and technical personnel. (4)Statistical analysis.The SPSS 22.0 statistical software was adopted and the independent samplesttestwasusedintheanalysisofpatientgenders.Thelinearcorrelationanalysiswasappliedinshoulderjointfunction,bloodloss,operationtime,fracturehealingtime,ASESscoresandConstantscores.Theαvalueofinspectionlevelwas0.05ondoublesidesandthedifferencewasconsideredstatisticallysignificantwithP<0.05.Results(1)Generalresults.ASESscore:totalscoreP=0.670,painP=0.078,lifefunctionP=0.010;Constantscore:totalscoreP=0.019,painP=0.083,functionalactivityP=0.453,shoulderactivityscaleP=0.007,musclestrengthP=0.869,bloodlossP<0.001,fracturehealingtimeP=0.001,operativetimeP=0.866.Dailylife:anteflexionandupliftP=0.012,abductionP=0.010,externalrotationP=0.038.ThemeanAIwas0.66in6malesand0.75in11femaleswiththecomparisonP=0.218.FivepatientshadsmallerAI(<0.68),including1caseof2-partfracture, 3casesof3-partfractureand1caseof4-partfracture.Themeanagewas55.8years(43-69years)andthemeanAIwas0.55 (0.47-0.66);Themeanintraoperativebloodlosswas110ml(100-150ml);Themeandegreeofanteflexionandupliftwas146° (120°-170°)with36°ofabductiononaverage(30°-40°)and88°ofexternalrotationonaverage(80°-110°);ThemeanASESscorewas83.8points(80-90points)andthemeanConstantscorewas81points(76-91points);Themeanfracturehealingtimewas1.6months(1.5-2months).TwelvepatientshadlargerAI(>0.68),including7casesof2-partfracture, 4casesof3-partfractureand1caseof4-partfracture.Themeanagewas61.4years(48-69years)andthemeanAIwas0.78 (0.69-0.94);Themeanintraoperativebloodlosswas257.5ml(150-300ml);Themeandegreeofanteflexionandupliftwas161.6° (120°-180°)with40°ofabductiononaverage(20°-50°)and106.5°ofexternalrotationonaverage(85°-160°);ThemeanASESscorewas89.7points(80-96points)andthemeanConstantscorewas87.3points(79-98points);themeanfracturehealingtimewas2.25months(1.5-3months).(2)Postoperativecomplications.Inthelastfollow-ups,noiatrogenicneurovascularinjury,woundinfection,internalfixationfailureorhumeralheadnecrosiswerefoundin17patients.Onepatienthadipsilateralelbowjointstiffness(110°offlexionand50°ofextension)butnomusclestrengthloss,muscleatrophyorothernervedamages,whichwasconsideredtoberelevantwiththe3monthsabsenceofoutpatientfollow-ups.Thereleasesurgeryofelbowjointwasperformed1yearafterMultilocintramedullarynailfixationandthefunctionalrehabilitationwasacquiredafteroperation(130°offlexionand10°ofextension).TherewasnoobviouscorrelationbetweenAIandpostoperativebleedingcomplications.ConclusionsNoobviouscorrelationwasfoundbetweentheAIandthegenders,agesandoperationtimeinthetreatmentofproximalhumeralfractureswithintramedullarynails.ThesmallerAIindicatedlessintraoperativebloodlossandfracturehealingtime.Onthecontrary,thelargerAIindicatedmoreintraoperativebloodlossandfracturehealingtime.ThepatientswithlargerAIobtainedhigherASESandConstantscoresandbetterpostoperativefunction(anteflexion,abductionandexternalrotation).OtherwisethepatientwithsmallerAIacquiredlessASESandConstantscoresandrelativelypoorpostoperativefunction.NooperativecomplicationsoccurredinthetreatmentofproximalfractureswithMultilocintramedullarynailandtheAIhadnosignificantcorrelationwiththepostoperativecomplications.
Acromionindex;Proximalhumeralfractures;Intramedullarynail
10.3877/cma.j.issn.2095-5790.2016.04.005
四川省中医院管理局课题(2016C040)
646000泸州,西南医科大学1;610041成都,四川省骨科医院上肢科2
向明,Email:josceph_xm@sina.com
2016-09-29)