Effects of ultra-low frequency transcranial magnetic stimulation on motor function and intelligence of children with spastic cerebral palsy: study protocol for a randomized parallel-cohort controlled trial
2016-04-09JunyanFengLingShanBingWangFeiyongJia
Jun-yan Feng, Ling Shan, Bing Wang, Fei-yong Jia*
Department of Pediatric Rehabilitation, First Hospital, Jilin University, Changchun, Jilin Province, China
Background
With advances in perinatal medicine, neonatal mortality has gradually decreased over the years. However, the incidence of cerebral palsy shows an increased tendency (Horsman et al., 2010). Comprehensive rehabilitation training is currently the primary method for treating cerebral palsy.Prompt, long-term, and normative comprehensive rehabilitative training has been shown to improve motor function to varying degrees in children with cerebral palsy (Jia et al., 2011). However, this rehabilitative training is difficult,requires long-term treatment, and provides curative effects that are still far from ideal. Therefore, novel treatment methods are urgently needed to promote rehabilitation in children with cerebral palsy.
The nervous system relays information mainly via neurotransmitters; nervous system lesions inevitably lead to disruption of neurotransmitter systems (Yildiz-Yesiloglu and Ankerst, 2006; Kulak et al., 2009). Amino acids are widely distributed throughout the nervous system, and the concentrations are far greater than the concentration of other neurotransmitters. Some of these amino acids include glutamic acid and aspartate, which are excitatory neurotransmitters, and γ-aminobutyric acid and glycine,which are inhibitory neurotransmitters.
Most child patients with spastic cerebral palsy have a history of asphyxia, and hypoxia is one of the mechanisms underlying fetal and neonatal cerebral damage (Dixon et al.,2015). The nervous system and the various factors that are released by cerebral vessels play a critical role during the initial stages of hypoxic damage; excitatory neurotoxins,mainly the excessive excitatory effects of glutamate, greatly contributes to damage to neurons and other cells, such as periventricular oligodendrocytes, which have been shown to be closely related to various nervous system dysfunctions(Pavlakis et al., 1999; Johnston et al., 2001). Xu et al. (2004)analyzed levels of excitatory and inhibitory amino acids in the cerebrospinal fluid of 45 patients with spastic cerebral palsy, determining that γ-aminobutyric acid levels were significantly reduced in the cerebrospinal fluid of patients,although glutamic acid and aspartate levels were significantly greater than in normal controls. Additionally, glutamic acid levels in the cerebrospinal fluid positively correlated with muscular tension in the patients (P < 0.05). Guo (2012)detected expression of glutamic acid and γ-aminobutyric acid, as well as their receptors GluR1 and GABAA, respectively, in the brains of rats with intrauterine growth retardation. Gou’s results showed that intrauterine growth retardation increased excitatory neurotransmitter glutamic acid release and GluR1 receptor expression, but decreased γ-aminobutyric acid levels and GABAA receptor expression,which is likely to be a mechanism by which cerebral palsy and epilepsy occur in patients who suffer from intrauterine growth retardation. Together these findings suggest that neurotransmitter levels vary in the brains of patients with cerebral palsy. The above-mentioned studies have shown that changes in neurotransmitter levels in cerebral palsy patients also influence neurosynapse function, resulting in increased excitatory synaptic strength and decreased presynaptic strength and postsynaptic strength. These observations are possibly related to muscular spasms and various nervous system dysfunctions in spastic cerebral palsy.
Transcranial magnetic stimulation uses a magnetic field pulse to stimulate the central nervous system (mainly the brain), creating a current impulse of membrane potential to cortical neurons, ultimately leading to a series of physiobiochemical changes. Transcranial magnetic stimulation is a painless, noninvasive method, and has been increasingly accepted in the fields of nervous system diseases and rehabilitation (Andoh and Martinot, 2008; Andoh and Zatorre, 2011). According to the intensity of stimulation frequency, repetitive transcranial magnetic stimulation can be divided into high frequency and low frequency (≤1 Hz) stimulations, while transcranial magnetic stimulation at a frequency of < 0.2 Hz is considered to be ultra-low frequency stimulation.
Ultra-low frequency transcranial magnetic stimulation uses a special magnetic field on the head. Thus, a special induced current is generated in the brain, which has been used to treat brain disorders by strengthening the ultra-slow wave power of neurotransmitters, as well as regulating electrical activity and affecting the physiological function of each neurotransmitter. An encephalofluctuograph examination can help to determine the changes in neurotransmitter levels in some brain disorders, as well as some of the physiological functions of neurotransmitters. Thus, ultra-low frequency transcranial magnetic stimulation overcomes the shortcomings of conventional transcranial magnetic stimulation by taking into consideration stimulation intensity, frequency,protocol, and curative effects (Feng et al., 2013). Ultra-low frequency transcranial magnetic stimulation in combination with encephalofluctuograph examination can provide indices to objectively and quantitatively assess the diagnosis of and curative effects on brain disorders (Xu et al., 2009).
Ultra-low frequency transcranial magnetic stimulation has been widely used to treat insomnia and depression.However, its use for the treatment of cerebral palsy has been little reported. In this randomized, parallel cohort-controlled trial, child patients with spastic cerebral palsy are assigned to an ultra-low frequency transcranial magnetic stimulation(experimental) group or a comprehensive rehabilitation(control) group.
The Gross Motor Function Measure (GMFM) score, Fine Motor Function Measure (FMFM) score, and Wechsler Intelligence Scale for Children (WISC) score will be used to assess motor function and intelligence in child patients with spastic cerebral palsy to investigate the curative effects, application value, and significance of using ultra-low frequency transcranial magnetic stimulation on spastic cerebral palsy in children.
Methods/design
Study design
A randomized parallel-cohort controlled trial.
Study setting
Department of Pediatric Rehabilitation, First Hospital, Jilin
University, China.
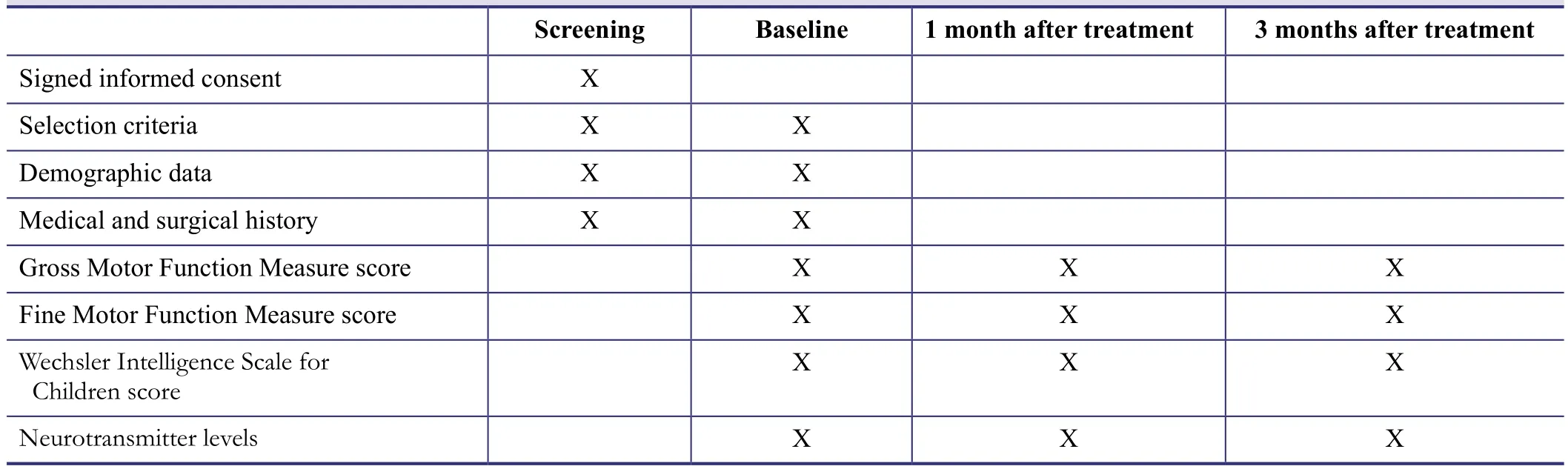
Table 1: Trial outcome evaluation schedule
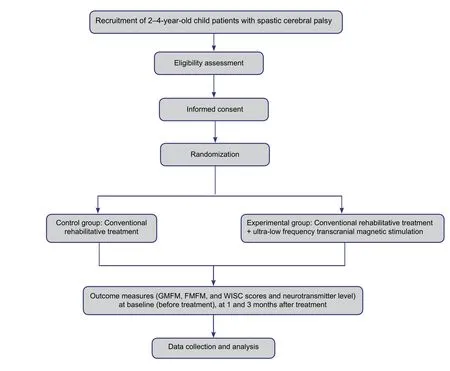
Figure 1: Study flow chart.
Study participants
Inclusion criteria
● Fulfill the diagnosis criteria of spastic cerebral palsy
● Age of 2–4 year
● Ability to follow orders
● Signed, written, informed consent to undergo the therapeutic regimen from each child’s guardian
Exclusion criteria
● Had (or have) a disabling disease in the past or during the study period
● Current or past surgery during the study period or within 1 year before admission
● Current or past therapy with administration of Bacillus botulinus during the study period or within 6 months before admission
● Complicated by epilepsy
● Implantation of metal or an electronic device
● Intracranial infection
● Severe heart, lung, liver, or kidney dysfunction
● Acute hemorrhagic disease
● Poor compliance or unsuitable for participation in this trial
Rejection criteria
● Do not undergo treatment within designated time
● Incomplete medical records
Withdrawal criteria
● Poor compliance, unable to accomplish rehabilitation training or therapy
● Child’s guardian proposed withdrawal from the trial
● Took drugs that can influence the child’s tolerance
Randomization procedure
The included child patients are allocated into groups using a computer-based simple randomization method and are then randomly coded. The codes are provided in a corresponding light-tight emergency envelope, and kept in a secure,locked storage area.
Intervention measures
Control group: Conventional rehabilitative treatments,including exercise therapy, Chinese traditional manipulation (with three considerations including promoting muscle strength recovery, inhibiting abnormal posture, and regulating range of motion), and muscle fiber excitation, once per day for 30 minutes for each item, for a total of 6 days per week.
Experimental group: In addition to routine rehabilitative treatments, ultra-low frequency transcranial magnetic stimulation is used (ultra-low frequency transcranial magnetic stimulation instrument, KF-10, Shenzhen Cornley Hi-Tech Co., Ltd., China). The levels of neurotransmitters, including γ-aminobutyric acid and glutamic acid, in the brain are detected with a SP03 encephalofluctuograph. Over-expressed neurotransmitters are input into the ultra-low frequency transcranial magnetic stimulation instrument. The magnetic field strength (≤ 45 mT (450 Gs)), stimulation time for each above-mentioned consideration (5–15 minutes), and total stimulation time (30 minutes once) are designated.Ultra-low frequency transcranial magnetic stimulation was performed once per day for 10 consecutive days, then twice per week for 2 consecutive weeks, and lastly once per week for 3 consecutive weeks. Ultra-low frequency transcranial magnetic stimulation is terminated or continued (once a week) according to re-examination results for neurotransmitter levels in the brain.
A trial protocol flow chart is shown in Figure 1.
Outcome measures
Primary outcomes
Gross motor function is evaluated using the GMFM score(Feng et al., 2013), fine motor function is evaluated using the FMFM score (Feng et al., 2013), and intelligence is measured using the WISC score. Neurotransmitter levels in the brain, as well as adverse events, are also evaluated.
Blindness evaluation
All evaluations are performed using a single-blinded method. The evaluators are blinded to patient grouping. All data are computer-processed by a statistician who will not participate in the trial.
The outcome evaluation schedule is shown in Table 1.
Data collection, management and statistical analysis
Data collection
The collected data are recorded in a table for subsequent identification, classification, processing, and analysis. During the process of data recording, original data should be checked often to ensure accuracy. Caution should be taken not to omit data, and data can be corrected or re-checked at any time.
Follow up
All patients are followed up at 1 and 3 months after treatment and index evaluation is performed by a physician who is blinded to the grouping. The patients who are unable to visit the hospital are followed up via telephone and the causes for hospital follow-up absence are recorded.
Data management
The medical records acquired from the trial are collected by a designated person and kept in a secure, locked storage area. Simultaneously, the medical records are duplicated and electronically saved in the computer for later use and convenience. To ensure data quality, the data are doubly input.
Statistical analysis
All data from the trial are statistically processed using SPSS 16.0 software by a statistician who will not participate in the trial. Homogeneity test for variance was used to compare measurement data between two groups. The t-test is used for comparison of normally distributed data and the ranksum test for non-normally distributed data. Count data are expressed as rate. Chi-square test is used for intergroup comparison. A level of P < 0.05 is considered statistically significant.
Safety assessment
During the trial, any adverse events and other unexpected reactions will be recorded, evaluated, reported, and investigated. Corresponding solutions will be proposed, and disposal outcomes will be recorded.
Ethical issues and informed consent
This trial was approved by the Medical Ethics Committee, First Hospital of Jilin University, China (approval No. 100818-062). Signed written informed consent will be obtained from each subject. The trial protocol will be conducted in accordance with the Declaration of Helsinki.
DISCUSSION
Changes in neurotransmitter levels in the brains of patients with cerebral palsy have been shown to influence synapse function (Kulak et al., 2006). Ultra-low frequency transcranial magnetic stimulation utilizes an ultra-low frequency non-pulsed magnetic field to create ultra-low frequencyinduced current, which regulates synaptic function and can be used to treat brain disorders. The possible mechanisms by which ultra-low frequency transcranial magnetic stimulation ameliorates cerebral palsy include: (1) regulating neurotransmitter levels in the brain: ultra-low frequency transcranial magnetic stimulation has been shown to alter levels of γ-aminobutyric acid and glutamic acid, thereby improving the excitation/inhibition balance in the brains of child patients with cerebral palsy (Xu et al., 2010); (2)ultra-low frequency transcranial magnetic stimulation has been shown to increase expression of brain-derived nerve growth factor, promote neurite growth (Wang et al., 2010;Wang et al., 2011), enhance neural stem cell differentiation,and induce neuronal differentiation of neural stem cells,thereby providing neuroprotection and improving brain functions (Liu et al., 2011).
The ultra-low frequency transcranial magnetic stimulation instrument does not directly stimulate neurons to create an action potential. Therefore, it cannot disturb neuronal circadian rhythm. However, it generates an induced current with the same frequency to simulate the synaptic after-current potential of a particular neurotransmitter. Therefore, the efficiency of action potentials generated by neurons can be regulated, suggesting that some cerebral function can be specifically regulated. Previous studies have determined that ultra-low frequency transcranial magnetic stimulation is safer and more reliable than conventional transcranial pulsed magnetic stimulation (Anand and Hotson, 2002).
Results from this randomized parallel-cohort controlled trial will hopefully provide clinical data regarding the use of ultra-low frequency transcranial magnetic stimulation to improve motor function and intelligence in children with cerebral palsy. These data can be used to guide treatment and prognosis of cerebral palsy in the clinic. This trial is limited to a short follow-up period. Therefore, the long-term curative effects of ultra-low frequency transcranial magnetic stimulation require further investigation.
Trial status
Recruitment of participants has been finished and trial is ongoing.
Conflicts of interest
None declared.
Author contributions
JYF designed this trial protocol. LS, BW and FYJ were responsible for patient recruitment. All authors approved the final version of this article.
Plagiarism check
This paper was screened twice using CrossCheck to verify originality before publication.
Peer review
This paper was double-blinded and stringently reviewed by international expert reviewers.
Anand S, Hotson J (2002) Transcranial magnetic stimulation: neurophysiological applications and safety. Brain Cogn 50:366-386.
Andoh J, Martinot JL (2008) Interhemispheric compensation: a hypothesis of TMS-induced effects on language-related areas. Eur Psychiatry 23:281-288.
Andoh J, Zatorre RJ (2011) Interhemispheric connectivity influences the degree of modulation of TMS-Induced effects during auditory processing. Front Psychol 2:161.
Dixon BJ, Reis C, Ho WM, Tang J, Zhang JH (2015) Neuroprotective strategies after neonatal hypoxic ischemic encephalopathy.Int J Mol Sci 16:22368-22401.
Feng JY, Jia FY, Jiang HY, Li N, Li HH, Du L (2013) Effect of infra-low-frequency transcranial magnetic stimulation on motor function in children with spastic cerebral palsy. Zhongguo Dang Dai Er Ke Za Zhi 15:187-191.
Guo TY (2012) Expression of amino acid neurotransmitters in the brain of rats with intrauterine growth retardation. Shenyang: China Medical University.
Horsman M, Suto M, Dudgeon B, Harris SR (2010) Ageing with cerebral palsy: psychosocial issues. Age Ageing 39:294-299.
Jia FY, Wang JT, Li HH, Hao YP, Li H, Liu B (2011) Effect of comprehensive rehabilitation on developmental quetient and intelligent structure of children with cerebral palsy. Zhongguo Fu You Bao Jian 26:2759-2760.
Johnston MV, Trescher WH, Ishida A, Nakajima W (2001) Neurobiology of hypoxic-ischemic injury in the developing brain. Pediatr Res 49:735-741.
Kulak W, Sobaniec W, Smigielska-Kuzia J, Kubas B, Zawada B,Otapowicz D (2009) An age and gender dependency of metabolite concentrations in basal ganglia in children with spastic diplegia: proton magnetic resonance spectroscopy study. J Child Neurol 24:73-79.
Kulak W, Sobaniec W, Smigielska-Kuzia J, Kubas B, Walecki J(2006) Metabolite profile in the basal ganglia of children with cerebral palsy: a proton magnetic resonance spectroscopy study.Dev Med Child Neuro 48:285-289.
Liu CY, Zhou SR, Sun XW, Liu ZL, Wu HL, Mei YW (2011) Effects of transcranial magnetic stimulation on the learning and memory abilities of those with cerebral infarction. Zhonghua Wuli Yixue yu Kangfu Zazhi 33:6-9.
Pavlakis SG, Kingsley PB, Harper R, Buckwald S, Spinazzola R,Frank Y, Prohovnik I (1999) Correlation of basal ganglia magnetic resonance spectroscopy with Apgar score in perinatal asphyxia.Arch Neurol 56:1476-1481.
Shi W, Yang H, Shi BP, Wang Y, Wang SJ (2009) Approaches for definition, clinical types and function classification of cerebral palsy domestic and abroad. Zhongguo Kangfu Lilun yu Shijian 15:801-803.
Wang F, Geng X, Tao HY, Cheng Y (2010) The restoration after repetitive transcranial magnetic stimulation treatment on cognitive ability of vascular dementia rats and its impacts on synaptic plasticity in hippocampal CA1 area. J Mol Neurosci 41:145-155.
Wang YY, Ma L, Ma XW, Ma QY, Gu P, Wang WM (2011) The influences of transcranial magnetic stimulation on the growth of hippocampus primary neuronal processes. Zhongguo Quanke Yixue 14:2051-2054.
Xu JL, Cai Q, Xu XX, Sun XH, Xu QY, Zhang JL (2009) Correlation between content of brain dopamine and the power of brain 11 mHz infra-slow wave spectrum in rats. Zhongguo Zuzhi Gongcheng Yanjiu yu Linchuang Kangfu 13:2510-2514.
Xu JL, Xu XX, Cai Q, Lu Q, Zhang JL (2010) Effects of gamma aminobutyric acid and dopamine characteristic repetitive ultralow frequency transcranial magnetic stimulations on rats' neurotransmitter neurotransmitter power. Zhongguo Kangfu Yixue Zazhi 25:127-130.
Xu P, Zhao Y, Zhang X (2004) Change of amino acid neurotransmitter in cerebrospinal fluid in children with cerebral palsy. Jilin Daxue Xuebao 30:117-119.
Yildiz-Yesiloglu A, Ankerst DP (2006) Neurochemical alterations of the brain in bipolar disorder and their implications for pathophysiology: a systematic review of the in vivo proton magnetic resonance spectroscopy findings. Prog Neuropsychopharmacol Biol Psychiatry 30:969-995.
杂志排行
Asia Pacific Journal of Clinical Trials:Nervous System Diseases的其它文章
- Correlating single nucleotide polymorphisms in vitamin D metabolism-related genes to autism susceptibility and vitamin D treatment: study protocol of a non-randomized parallelcohort controlled trial
- Use of low-dose dexmedetomidine in general anesthesia improves postoperative recovery of patients with supratentorial tumors: study protocol for a randomized controlled trial
- Intensive versus nonintensive insulin therapy for hyperglycemia after traumatic brain injury: study protocol for a randomized controlled trial
- Postoperative sedation by intranasal dexmedetomidine in patients with hypertensive cerebral hemorrhage: study protocol for a randomized parallel-cohort controlled trial
- The optimal time window for the use and dosage of nimodipine for acute massive cerebral infarction: study protocol for a randomized controlled trial