Combined vascular resection and analysis of prognostic factors for hilar cholangiocarcinoma
2015-12-24
Guangzhou, China
Combined vascular resection and analysis of prognostic factors for hilar cholangiocarcinoma
Shu-Tong Wang, Shun-Li Shen, Bao-Gang Peng, Yun-Peng Hua, Bin Chen, Ming Kuang, Shao-Qiang Li, Qiang He and Li-Jian Liang
Guangzhou, China
BACKGROUND: Hilar cholangiocarcinoma (HCCA) is a devastating malignancy arising from the bifurcation of the hepatic duct, whether combined vascular resection benefits HCCA patients is controversial. This study was undertaken to assess the effect of combined vascular resection in HCCA patients and to analyze the prognostic factors.
METHODS: Clinical data of 154 HCCA patients who had been treated from January 2005 to December 2012 were retrospectively analyzed. The patients were divided into three groups based on vascular resection: those without vascular resection; those with portal vein resection alone and those with hepatic artery resection. The survival and complication rates were compared among the three groups. Multivariate analysis was made to determine prognostic factors.
RESULTS: No significant differences were found in survival and complication rates among the three groups (P>0.05). Multivariate analysis showed that 3 factors were related to survival: lymph node metastasis, tumor size (>2.5 cm), and positive resection margin.
CONCLUSIONS: Vascular resection improved the survival rate of patients with HCCA involving the hepatic artery or portal vein. Lymph node metastasis, tumor size (>2.5 cm) and positive resection margin were poor prognostic factors in patients with HCCA.
(Hepatobiliary Pancreat Dis Int 2015;14:626-632)
hilar cholangiocarcinoma;
Introduction
Hilar cholangiocarcinoma (HCCA), also known as Klatskin tumor,[1]accounts for 50%-60% of all biliary tract cholangiocarcinomas.[2]HCCA is one of the most challenging diseases because of its location.[3]Resection is the only therapeutic option that offers a possibility of cure.[4]And the negative resection margin improves long-term survival.[5-7]One critical reason to preclude the negative resection margin is local invasion of major hilum vascular structures, such as the hepatic artery and portal vein. In such cases, only combined vascular resection can achieve negative resection margin. Numerous HCCA patients have undergone combined vascular resection in recent years.[8-12]However, there is no general consensus on whether combined vascular resection benefits HCCA patients. The main prognostic factors for HCCA are also controversial. Therefore, we retrospectively analyzed the data of HCCA patients treated in our center and evaluated the effect of vascular resection on patient survival; we also investigated the prognosis factors in patients with HCCA.
hepatic artery resection;
portal vein resection;
prognostic factors
Methods
Ethical guidelines and patients' data
This study was approved by the Medical Ethics Committee of the First Affiliated Hospital, Sun Yat-Sen University, Guangzhou, China. The study was conducted in accordance with theDeclaration of Helsinki. The data of the patients were extracted from their medical records and a prospective database established by the Department of Hepatic Surgery, First Affiliated Hospital, Sun Yat-sen University. Only HCCA patients who had been confirmed pathologically after resection were included in the study. Exclusion criteria: patients with distal bile duct carcinoma, gallbladder tumors or intrahepatic cholangiocarcinoma; and those with radiotherapy, che-motherapy or transplantation. Altogether, 277 HCCA patients were enrolled from January 2005 to December 2012. Among them, 93 patients had unresectable tumors because of extensive local invasion, distant metastases or concomitant systemic diseases. They were subjected to stent implantation, liver transplantation, chemotherapy, biotherapy, etc. The remaining 184 patients underwent surgical exploration with curative intent. In these patients, 30 had unresectable tumors because of local invasion or peritoneal seeding and 154 who had undergone tumor resection were analyzed (Fig. 1).
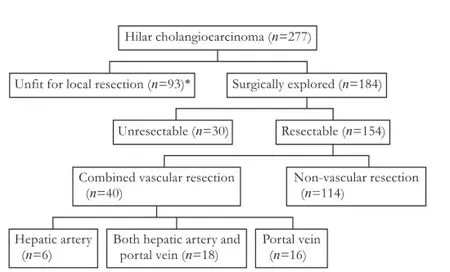
Fig. 1. Flow diagram showing the treatment of all patients in this study. *: These patients were not suitable for resection because of extensive local invasion, distant metastases or concomitant systemic diseases.
Preoperative assessment and biliary drainage
Tumor size, the stage of the disease and vascular involvement were evaluated preoperatively by imaging. All patients underwent contrast-enhanced ultrasound and multi-slice spiral computed tomography (CT). In the 154 patients, 103 were assessed by magnetic resonance imaging (MRI) (Fig. 2) and magnetic resonance cholangiopancreaticography. Residual liver volume was assessed in patients with extensive tumor invasion, hepatic lobe atrophy or vascular invasion. We transferred patient imaging data into hepatectomy simulation software (Myrian XP-Liver), calculated liver volume and made a surgical plan. Residual liver volume should be larger than 30% of total liver volume.
Cholangiography through percutaneous transhepatic cholangio drainage (PTCD) or endoscopic retrograde approaches were performed to describe the bile tract in 94 patients. The patients were staged according to the Bismuth-Corlette staging system, as type I (n=6), II (n=11), IIIa (n=36), IIIb (n=63), and IV (n=38). Preoperative biliary drainage was done in 74 (48.1%) patients, endoscopic nasobiliary drainage (ENBD) in 4, and PTCD in 65. Five patients underwent both ENBD and PTCD. The median drainage time was 14 days.
Surgery
All the operations for HCCA were performed by experienced surgeons. Regular resection consisted ofen blocresection of the common bile duct, the tumor and the gallbladder, and clearance of hepatoduodenal ligament lymph nodes. Caudate resection was routinely performed in patients receiving hepatectomy. Biliary drainage was completed by modified Warren hepaticojejunostomy or Roux-en-Y hepaticojejunostomy. Vascular resection and reconstruction were planned preoperatively in patients suspected of vascular invasion according to contrast-enhanced CT or MRI, and these procedures were performed only when the vasculature could not be detached from the tumor during surgery. Fifty-two patients were planned preoperatively to perform combined vascular resection because of the suspected vascular invasion. Only 36 (69.2%) of the 52 patients underwent vascular resection and reconstruction, 4 patients had peritoneal metastasis, 4 had no vascular invasion, and 8 had unresectable tumors. Four patients were found to have vascular invasion during exploration and underwent vascular resection and reconstruction. In total, combined vascular resection was performed in 40 patients. Eighteen patients underwent resection of the portal vein and hepatic artery, 16 underwent resection of the portal vein alone, and 6 underwent resection of the hepatic artery alone.
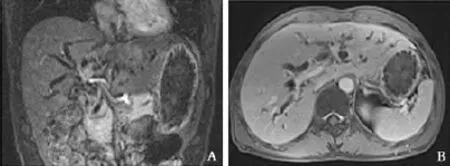
Fig. 2. Bismuth IV hilar cholangiocarcinoma. A: Enhanced MRI showing that tumor encroached the right hepatic artery; B: Enhanced MRI showing that the right portal vein was inviolate. We performed left hemihepatectomy, combined with right hepatic artery resection, right hepatic artery and gastroduodenal artery anastomosis.
We have a few technical tips to minimize the incidence of vascular complications: (1) use of microsurgical instruments; (2) protection of vascular intima; (3) vascular dissociation that makes vascular reconstruction tension appropriate; (4) perioperative anticoagulation while rinsing the vascular end with heparin saline during operation and subcutaneous injection of low molecular weight heparins after operation; (5) mild eversion suture; and (6) avoidance of suturing the adventitia into the vascular lumen. To minimize hepatic ischemia time and protect the residual liver function, we suggest to (1) conduct parenchymal transection before vascular resec-tion; and (2) reconstruct the portal vein first when both hepatic artery and portal vein are resected. Comparing with the hepatic artery, the portal vein provides more blood flow to the residual liver, and continuous suture in portal vein reconstruction is relatively easy and quick.
Groups
The 154 patients were divided into three groups based on the involvement of the hilum vessels (Miyazaki's method).[12]The non-vascular resection group consisted of 114 patients without vascular resection or reconstruction. The portal vein only group comprised 16 patients who underwent combined portal vein resection and reconstruction only. The hepatic artery group comprised 24 patients, 18 underwent both portal vein and hepatic artery resection and 6 underwent hepatic artery resection alone (Table 1).
Statistical analysis
Pearson's Chi-square test and Fisher's exact test were used to compare morbidity and mortality among the three groups. Continuous variables were expressed as mean±standard deviation. Categorical variables were expressed as numbers. Survival time was calculated from the day of surgery. Survival curves were calculated by the Kaplan-Meier method. Factors influencing the survival curves were compared using the log-rank test. Factors showing statistical significance shown by univariate analysis were analyzed by multivariate analysis. Statistical analysis was performed with SPSS software, version 22.0 (IBM, Armonk, NY, USA). Statistical significance was defined as a P value of <0.05.
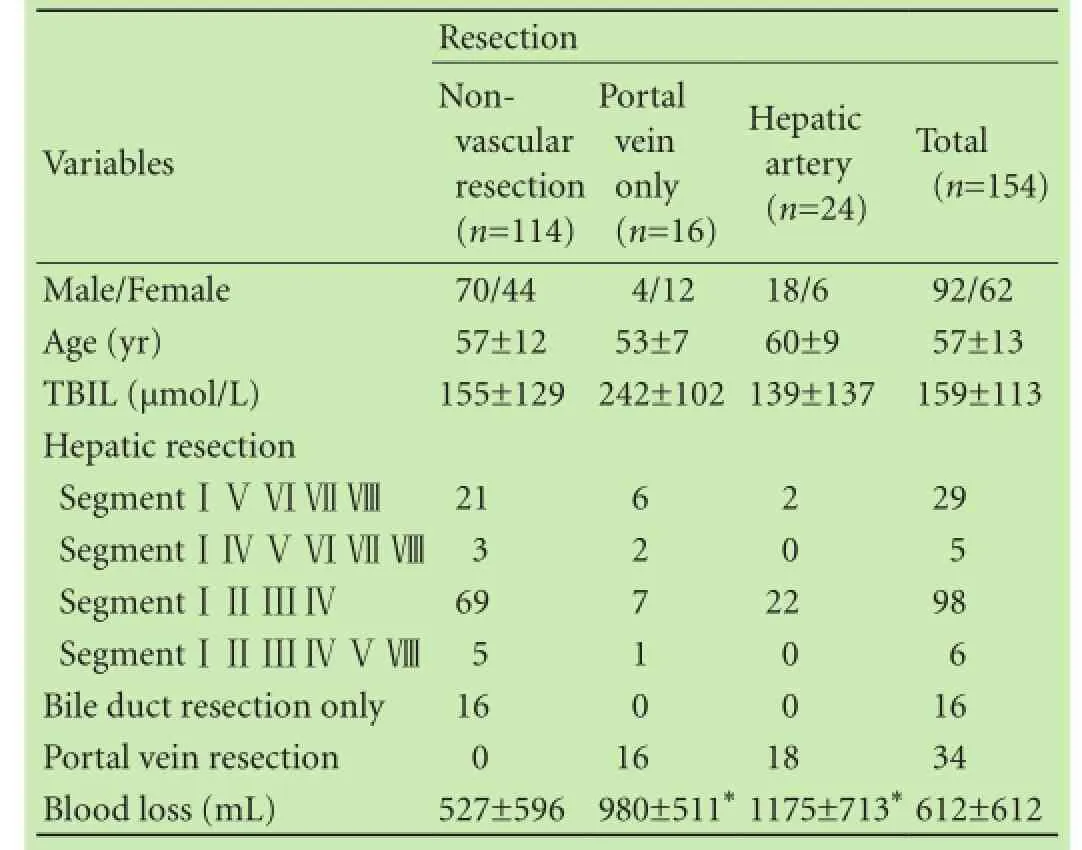
Table 1. Descriptive analysis of patients
Results
In the 154 patients, 40 underwent vascular resection and reconstruction, and 24 were subjected to resection and reconstruction of the hepatic artery (n=6) or resection and reconstruction of the portal vein and hepatic artery (n=18). Portal vein resection and reconstruction alone were performed in 16 patients (Fig. 1). Of the 16 patients, 3 had wedge resections and 13 segmental resections. Portal vein reconstruction in patients with wedge resection was completed using primary closure. The portal vein was reconstructed by end-to-end anastomosis between the residual trunk and the hepatic branch in 12 patients with segmental resection. In contrast to portal vein resection and reconstruction, hepatic artery resection and reconstruction were based on hepatic autografting, saphenous vein transplantation, and right gastroepiploic artery anastomosis (Table 2). The median reconstruction of the portal vein took 8.2 minutes, and that of the hepatic artery, 13.6 minutes. A typical combined vascular resection is shown in Fig. 3. The margin of the remnant bile duct was routinely resected for histological examination. The resection margins were negative for tumor tissue in 138 patients and positive in 16 patients.
Morbidity and mortality
Complications occurred in 56 patients (36.4%) after surgery. Bile leakage was the most common complication (n=22, 14.3%), followed by wound infection (n=12, 7.8%). Five patients died in the hospital after surgery within one month. There were no significant differences in morbidity or mortality among the three groups (P>0.05). Also there were no significant differences between any two groups (Fisher's exact test; P>0.05). Themorbidity and mortality were comparable between the patients who underwent vascular resection and those who did not undergo vascular resection (P>0.05). Combined resection of the hepatic artery and portal vein wasnot significantly related to the morbidity or mortality of the patients (Table 3).
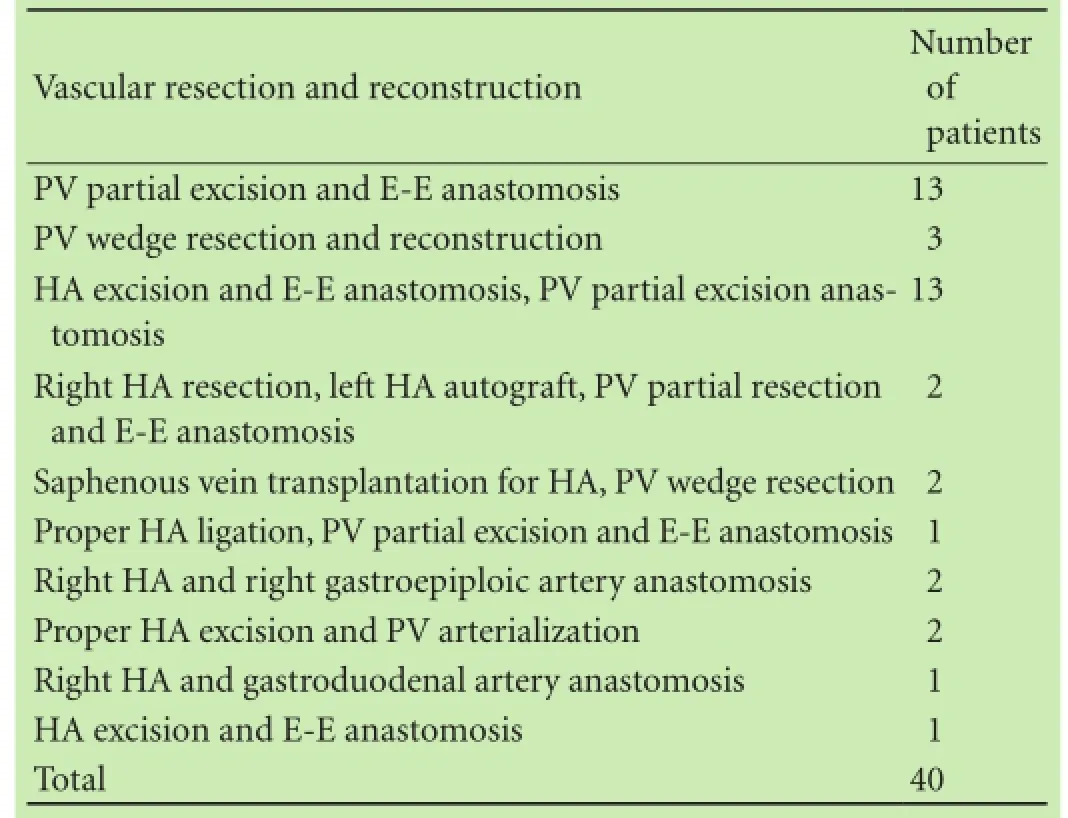
Table 2. Types of vascular resection and reconstruction
Survival
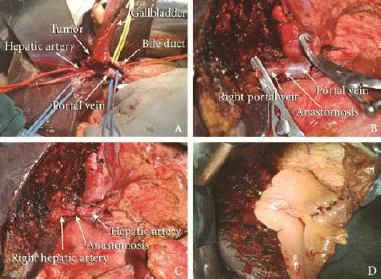
Fig. 3. Partial excision anastomosis of the hepatic artery and partial excision anastomosis of the portal vein. A: Ready for resection; B: Partial excision anastomosis of the portal vein; C: Partial excision anastomosis of the hepatic artery; D: After hepaticojejunostomy.
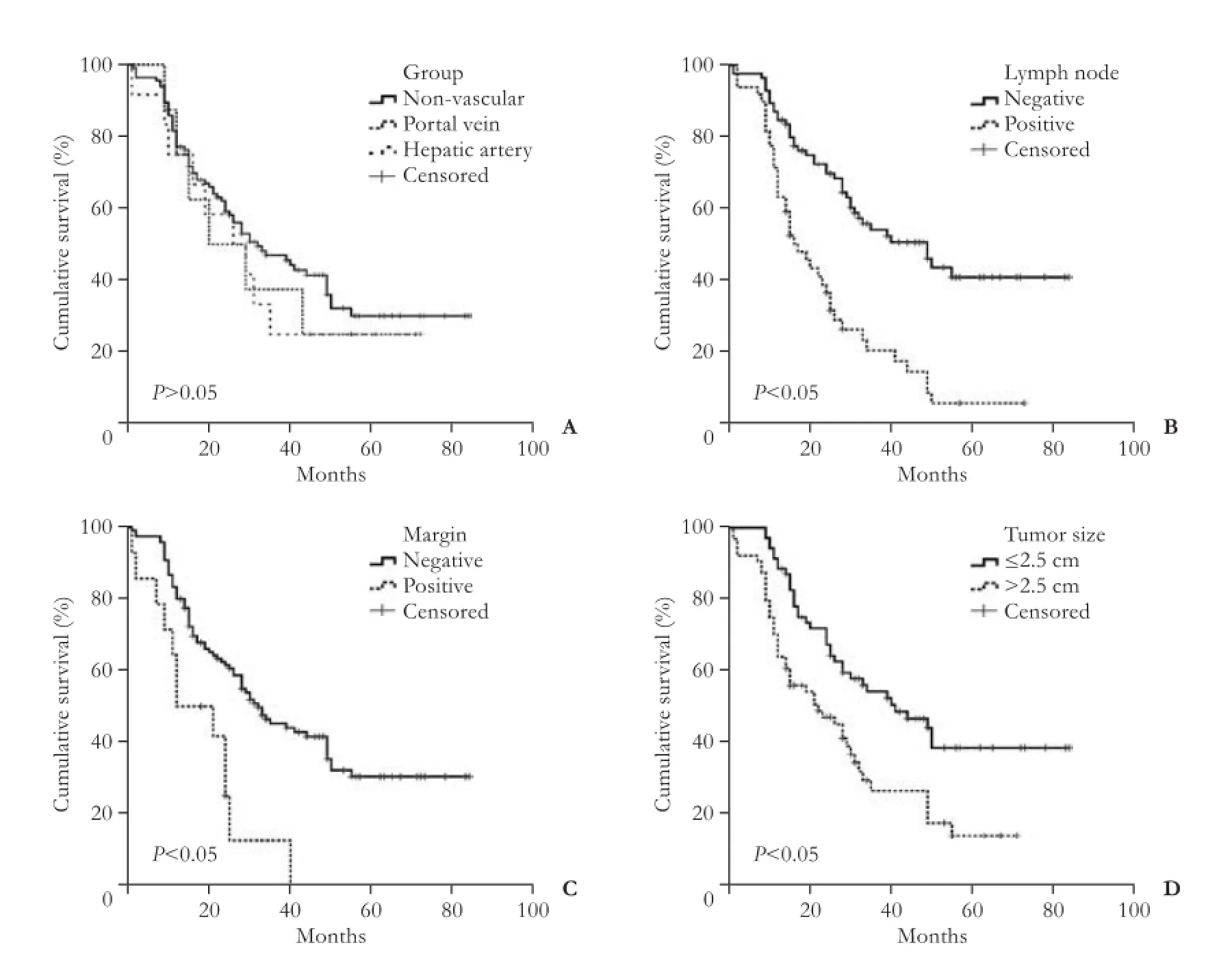
Fig. 4. Cumulative survival after surgery. A: Survival in the portal vein group, hepatic artery group and non-vascular resection group (log-rank test,P>0.05). Univariate analysis identified that lymph node metastasis (B), resection margin (C), and tumor size (>2.5 cm) (D) were the signifiant factors affecting survival.
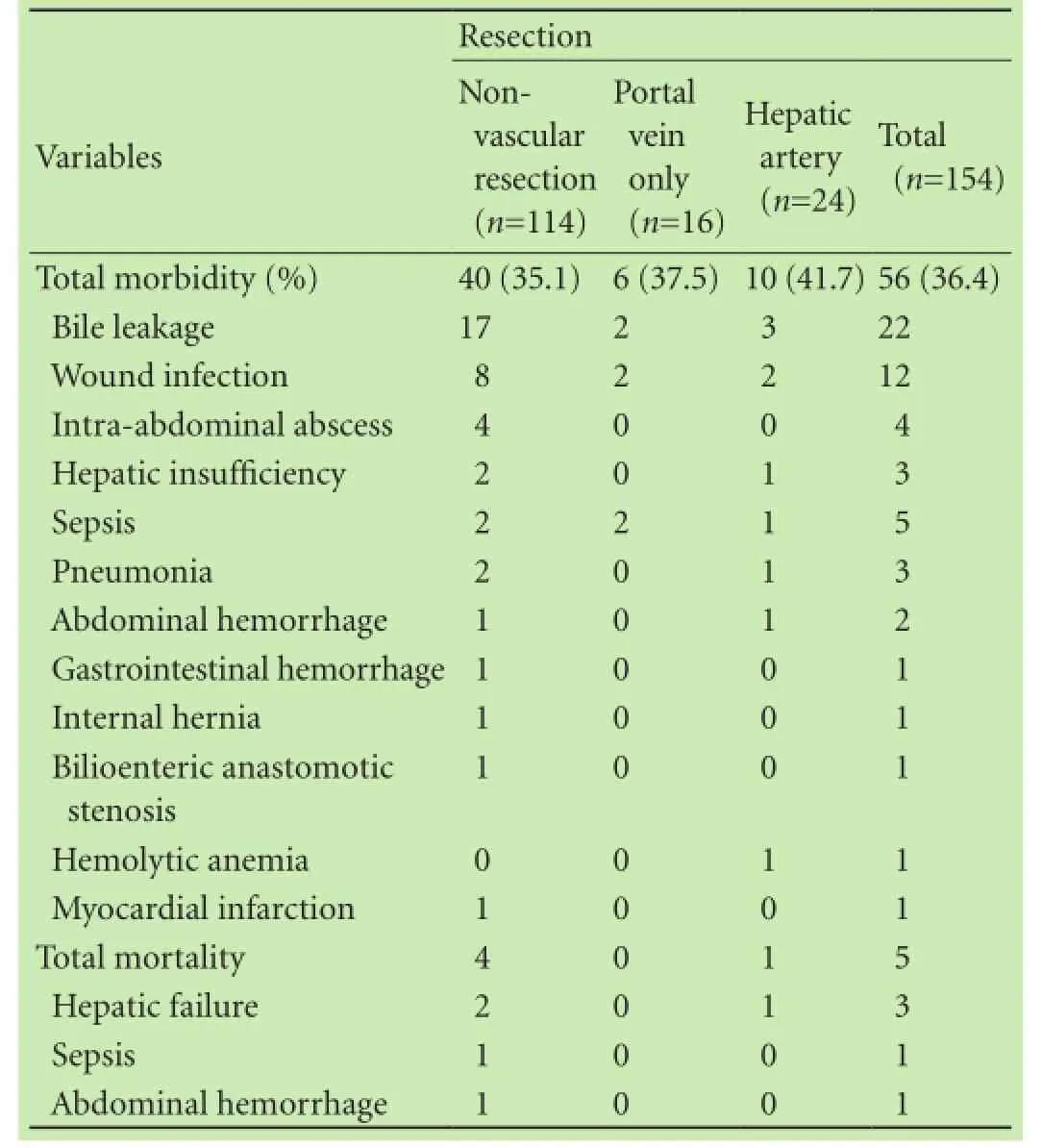
Table 3. Surgical morbidity and mortality
The 5-year survival rate was 35.7% (median survival, 32 months) for patients without vascular resection. It was proximately 25.0% for those who had portal vein resection (median survival, 20 months), and 25.0% for those who had hepatic artery resection (median survival, 26 months). No significant difference was observed among the three groups (log-rank test,P>0.05) (Fig. 4A). The 5-year survival rate of patients without lymph node metastasis was approximately 41.0% (median survival, 49 months) and that of those with lymph node metastasis (median survival, 17 months), 5.9% (Fig. 4B). The 5-year survival rate of patients with negative margins was approximately 30.4% (median survival, 32 months), and that of those with positive margins (median survival, 12 months), 0% (Fig. 4C). The 5-year survival rate of patients with tumors ≤2.5 cm was approximately 38.8% (median survival, 41 months), and that of those with tumors >2.5 cm (median survival, 22 months) was 14.3% (Fig. 4D).
Univariate and multivariate analysis
Univariate analysis identified that lymph node metastasis, resection margin, and tumor size were the significant factors affecting survival (Fig. 4). Age, gender, vascular resection, and histologic differentiation were not significantly related to the prognosis after resection. Multivariate analysis revealed three independent prognostic factors that influenced survival after resection: lymph node metastasis, tumor size, and resection margin (Table 4). Portal vein resection and hepatic artery resection were not independent risk factors.
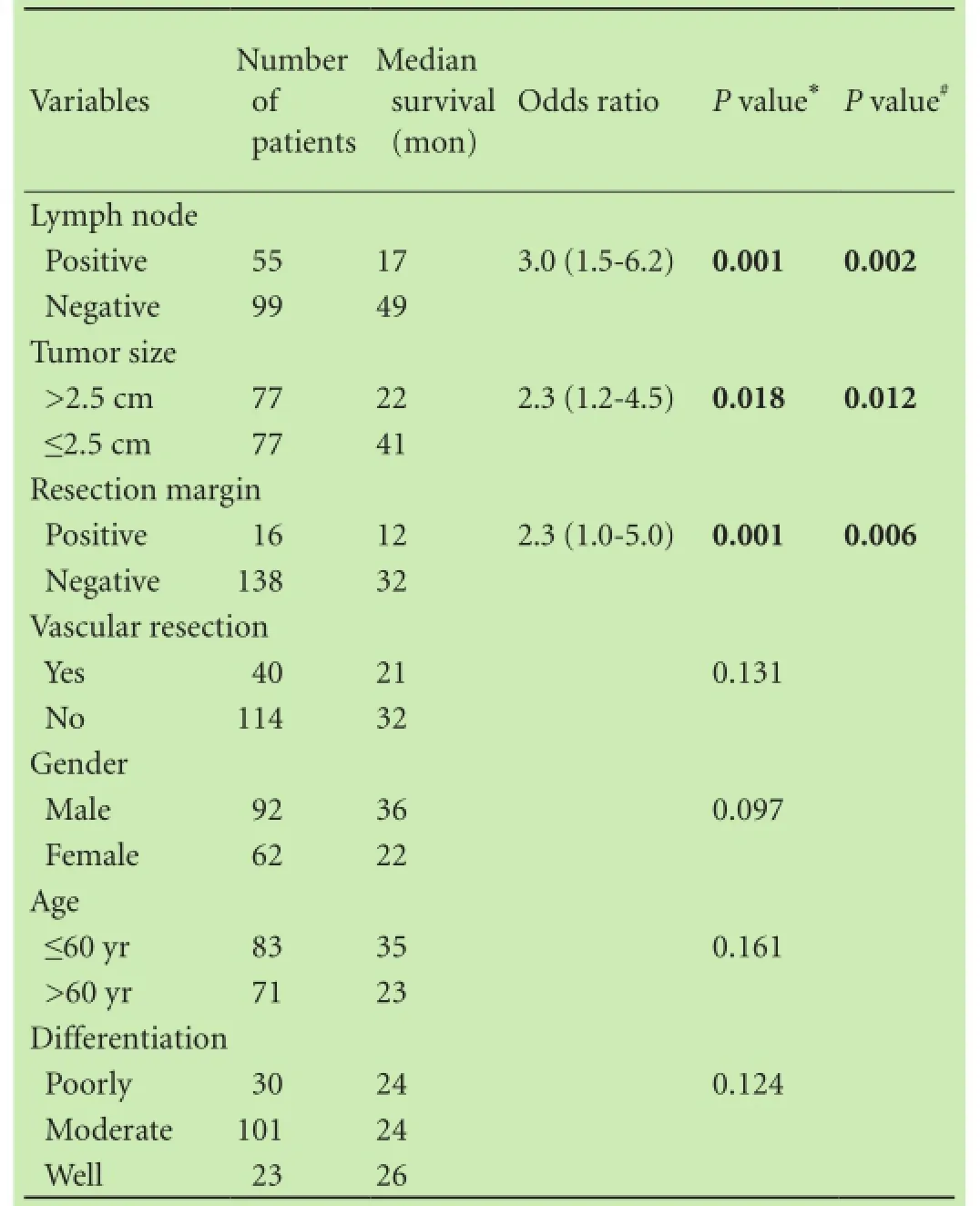
Table 4. Prognostic factors
Discussion
There has been controversial over whether combined vascular resection is benefitial to HCCA patients. The data of a large Japanese series showed that combined vascular resection (portal vein or hepatic artery resection) is an independent poor prognostic factor after curative resection of HCCA. The survival rate of the non-vascular resection group was higher than that of the combined vascular resection group.[12]Conversely, a recent metaanalysis[13]indicated that combined portal vein resection increases the overall survival in advanced HCCA patients. They demonstrated that combined portal vein resection was feasible in the treatment of HCCA. Our results demonstrated that resection of the portal vein and hepatic artery was safe and effective in radical resection of HCCA. The morbidity and mortality of the vascular groups (the hepatic artery group or the portal vein group) were not significantly different from those of the non-vascular resection group.
Previous reports showed that the survival rate of HCCA patients with vascular involvement and without combined vascular resection was poorer than that of those without vascular involvement.[14]The survival time was not significantly different among the three groups in our study, indicating that vascular resection was beneficial. If the involved vasculature could be resected, patients with vascular involvement had the same probability of survival as those without vascular involvement. These results showed that the involvement of the portal vein or hepatic artery was not a contraindication for curative resection in patients with HCCA.
Sometimes, the hepatic artery is difficult to reconstruct after resection. In our study, two patients in the hepatic artery resection group underwent portal vein arterialization. One of them was alive and healthy for more than 76 months after surgery. Hence portal vein arterialization might be a good solution if hepatic artery reconstruction is difficult after resection. Certainly, more studies are needed. Another patient underwent anasto-mosis of the right hepatic artery and gastroduodenal artery because of difficulty in reconstruction. The patient was alive and healthy for 68 months after surgery. How can the hepatic artery be reconstructed after resection, particularly when direct end-to-end anastomosis is difficult to perform? Should portal vein arterialization be performed, or should another artery be used for anastomosis? These questions should be answered in the future studies.
The treatment of HCCA has been improved over decades.En blocbile duct resection with or without hepatectomy, caudate lobectomy, and lymph node dissection are performed routinely. Hilar vascular resection and reconstruction are increasingly performed in selected patients to obtain R0 resection. However, the survival time of some patients remains disappointing. If the survival of these patients is predictable via the prognostic factors, the patients could be given more personalized healthcare. Patients with a high risk of recurrence need frequent follow-ups after surgery. Patients also need to be treated differently depending on prognostic factors. However, no consensus has been reached on prognostic factors in patients with HCCA, such as lymph node status. Studies on this topic are also inconsistent with the association of lymph node status with survival, some authors showed clear effects and others did not.[9,15]
Our results showed that lymph node metastasis was a poor prognostic factor. The median survival time of lymph node-involved patients was 17 months, much shorter than that (49 months) of patients without lymph node involvement. Although we performed lymphadenectomy, the survival of lymph node positive patients was still dismal. Positive lymph node involvement may suggest a more advanced, biologically aggressive tumor.[11]Patients with positive lymph node should be compared separately as a subgroup when we design clinical trials to test new treatments for HCCA patients in the future.
A study[16]emphasized the importance of complete resection with tumor-free margins to improve survival. We found that the median survival time was 12 months in patients with positive margins and 32 months in those with negative margins.
The average tumor size of our patients was 2.5 cm, we therefore divided the patients into two groups. The median survival time of patients whose tumor size was>2.5 cm was 22 months, much shorter than that of those whose tumor size was ≤2.5 cm (41 months). Multivariate analysis showed that tumor size >2.5 cm was the only preoperative factor associated with early death after resection. Hughes et al[17]analyzed 331 patients with HCCA and found that tumor size >3.0 cm was independently associated with death within 12 months. It seems that the larger the HCCA tumor size is, the shorter the time that patients live after tumor resection. Therefore, early detection and resection of HCCA are of vital importance.
The clinical practice guidelines of the National Comprehensive Cancer Network pointed out that new treatments including adjuvant chemo-radiation therapy can be used to prolong the survival of HCCA patients, particularly those with poor prognostic factors. Patients who underwent surgery and adjuvant chemo-radiation had a longer survival rate.[18]Adjuvant concurrent 5-FU-based chemo-radiation should be performed in patients with positive margins or positive lymph nodes after resection of HCCA.[7]A recent meta-analysis[19]evaluated adjuvant therapy in the treatment of biliary tract cancer and supported the use of adjuvant therapy for patients with high-risk feature after resection of tumor, especially those patients with lymph node-positive disease (OR=0.49;P=0.004) and R1 resection (OR=0.36;P=0.002). Our study demonstrated that tumor size was another high-risk factor relating to poor prognosis. Whether adjuvant chemo-radiation therapy should be given to the patients with large size HCCA needs further study.
Our study has some limitations. The number of patients with vascular resection was small since HCCA is rare, and thus the conclusions should be verified in further studies.
In conclusion, combined vascular resection may result in more R0 resections and prolong the survival of HCCA patients with vascular invasion. However, this procedure does not significantly affect postoperative morbidity or mortality. Lymph node metastasis, tumor size >2.5 cm and positive resection margins are vital poor prognostic factors for HCCA patients.
Contributors:PBG proposed the study. WST and SSL analyzed the data, wrote the first draft and contributed equally to this article. All authors contributed to the design and interpretation of the study and to further drafts. PBG is the guarantor.
Funding:This study was supported by a grant from the National Natural Science Foundation of China (81172039).
Ethical approval:This study was approved by the Medical Ethics Committee of the First Affiliated Hospital, Sun Yat-Sen University.
Competing interest:No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
1 Klatskin G. Adenocarcinoma of the hepatic duct at its bifurcation within the porta hepatis. an unusual tumor with distinctive clinical and pathological features. Am J Med 1965;38:241-256.
2 Khan SA, Davidson BR, Goldin RD, Heaton N, Karani J,Pereira SP, et al. Guidelines for the diagnosis and treatment of cholangiocarcinoma: an update. Gut 2012;61:1657-1669.
3 Deoliveira ML, Schulick RD, Nimura Y, Rosen C, Gores G, Neuhaus P, et al. New staging system and a registry for perihilar cholangiocarcinoma. Hepatology 2011;53:1363-1371.
4 Yu W, Gu Z, Shi S, Shen N, Zhang Y. Effect evaluation of vascular resection for patients with hilar cholangiocarcinoma: original data and meta-analysis. Cell Biochem Biophys 2014;69:509-516.
5 Ebata T, Kosuge T, Hirano S, Unno M, Yamamoto M, Miyazaki M, et al. Proposal to modify the International Union Against Cancer staging system for perihilar cholangiocarcinomas. Br J Surg 2014;101:79-88.
6 Matsuo K, Rocha FG, Ito K, D'Angelica MI, Allen PJ, Fong Y, et al. The Blumgart preoperative staging system for hilar cholangiocarcinoma: analysis of resectability and outcomes in 380 patients. J Am Coll Surg 2012;215:343-355.
7 Cannon RM, Brock G, Buell JF. Surgical resection for hilar cholangiocarcinoma: experience improves resectability. HPB (Oxford) 2012;14:142-149.
8 Tamoto E, Hirano S, Tsuchikawa T, Tanaka E, Miyamoto M, Matsumoto J, et al. Portal vein resection using the no-touch technique with a hepatectomy for hilar cholangiocarcinoma. HPB (Oxford) 2014;16:56-61.
9 Nagino M, Ebata T, Yokoyama Y, Igami T, Sugawara G, Takahashi Y, et al. Evolution of surgical treatment for perihilar cholangiocarcinoma: a single-center 34-year review of 574 consecutive resections. Ann Surg 2013;258:129-140.
10 de Jong MC, Marques H, Clary BM, Bauer TW, Marsh JW, Ribero D, et al. The impact of portal vein resection on outcomes for hilar cholangiocarcinoma: a multi-institutional analysis of 305 cases. Cancer 2012;118:4737-4747.
11 Hemming AW, Mekeel K, Khanna A, Baquerizo A, Kim RD. Portal vein resection in management of hilar cholangiocarcinoma. J Am Coll Surg 2011;212:604-616.
12 Miyazaki M, Kato A, Ito H, Kimura F, Shimizu H, Ohtsuka M, et al. Combined vascular resection in operative resection for hilar cholangiocarcinoma: does it work or not? Surgery 2007;141:581-588.
13 Chen W, Ke K, Chen YL. Combined portal vein resection in the treatment of hilar cholangiocarcinoma: a systematic review and meta-analysis. Eur J Surg Oncol 2014;40:489-495.
14 Park J, Kim MH, Kim KP, Park do H, Moon SH, Song TJ, et al. Natural History and Prognostic Factors of Advanced Cholangiocarcinoma without Surgery, Chemotherapy, or Radiotherapy: A Large-Scale Observational Study. Gut Liver 2009;3:298-305.
15 Endo I, House MG, Klimstra DS, Gönen M, D'Angelica M, Dematteo RP, et al. Clinical significance of intraoperative bile duct margin assessment for hilar cholangiocarcinoma. Ann Surg Oncol 2008;15:2104-2112.
16 Regimbeau JM, Fuks D, Pessaux P, Bachellier P, Chatelain D, Diouf M, et al. Tumour size over 3 cm predicts poor shortterm outcomes after major liver resection for hilar cholangiocarcinoma. By the HC-AFC-2009 group. HPB (Oxford) 2015;17:79-86.
17 Hughes MA, Frassica DA, Yeo CJ, Riall TS, Lillemoe KD, Cameron JL, et al. Adjuvant concurrent chemoradiation for adenocarcinoma of the distal common bile duct. Int J Radiat Oncol Biol Phys 2007;68:178-182.
18 Benson AB 3rd, Abrams TA, Ben-Josef E, Bloomston PM, Botha JF, Clary BM, et al. NCCN clinical practice guidelines in oncology: hepatobiliary cancers. J Natl Compr Canc Netw 2009;7:350-391.
19 Horgan AM, Amir E, Walter T, Knox JJ. Adjuvant therapy in the treatment of biliary tract cancer: a systematic review and meta-analysis. J Clin Oncol 2012;30:1934-1940.
Received February 3, 2015
Accepted after revision June 23, 2015
Author Affiliations:Department of Hepatic Surgery, First Affiliated Hospital, Sun Yat-Sen University, Guangzhou 510080, China (Wang ST, Shen SL, Peng BG, Hua YP, Chen B, Kuang M, Li SQ, He Q and Liang LJ)
Bao-Gang Peng, MD, PhD, Department of Hepatic Surgery, First Affiliated Hospital, Sun Yat-Sen University, Guangzhou 510080, China (Tel: +86-20-87755766ext8214; Email: pengbaogang@medmail. com.cn)
© 2015, Hepatobiliary Pancreat Dis Int. All rights reserved.
10.1016/S1499-3872(15)60025-X
Published online October 21, 2015.
杂志排行

Hepatobiliary & Pancreatic Diseases International的其它文章
- Primary hepatic solitary fibrous tumor with histologically benign and malignant areas
- Pigmented well-differentiated hepatocellular neoplasm with β-catenin mutation
- An immortalized rat pancreatic stellate cell line RP-2 as a new cell model for evaluating pancreatic fibrosis, inflammation and immunity
- Trametinib and dactolisib but not regorafenib exert antiproliferative effects on rat pancreatic stellate cells
- Coagulopathy and the prognostic potential of D-dimer in hyperlipidemia-induced acute pancreatitis
- Ankaflavin ameliorates steatotic liver ischemiareperfusion injury in mice