TNF-α和HSP70-2基因多态性与急性胰腺炎的相关性研究
2015-12-21胡家平庄建新李勇余永欢胡庆红赖银英吴安涛
胡家平,庄建新,李勇,余永欢,胡庆红,赖银英,吴安涛
TNF-α和HSP70-2基因多态性与急性胰腺炎的相关性研究
胡家平,庄建新△,李勇,余永欢,胡庆红,赖银英,吴安涛
目的探讨肿瘤坏死因子(TNF)-α和热休克蛋白(HSP)70-2基因多态性与急性胰腺炎(AP)的相关性。方法运用聚合酶链式反应-限制性片段长度多态性(PCR-RLFP)检测72例AP患者(AP组)和71例正常人(对照组)的TNF-α及HSP70-2基因多态性。结果AP组与对照组的TNF-α基因型和等位基因比例间差异无统计学意义;AP组中,重型胰腺炎(SAP)和轻型胰腺炎(MAP)的TNF-α基因型和等位基因间差异无统计学意义。TNF-α和HSP70-2基因AA型与GA+GG型患者的白细胞、C反应蛋白(CRP)、淀粉酶、三酰甘油、血糖差异均无统计学意义;AP组的HSP70-2基因GA+GG型患者比例高于对照组(69.4%vs 49.3%),AP组携带的G等位基因比例高于对照组(46.5%vs 31.7%),差异均有统计学意义。AP组中,SAP的GA+GG型比例高于MAP(81.0%vs 53.3%),差异有统计学意义;而G等位基因在SAP和MAP间无明显差异(P>0.05)。结论TNF-α基因多态性与AP不相关,HSP70-2基因多态性与AP相关,携带G等位基因发生重症AP的可能性增大,可能是重症AP的易感因素之一。
肿瘤坏死因子α;HSP70热休克蛋白质类;胰腺炎;基因多态性;HSP70-2;多态性,限制性片断长度;聚合酶链反应
急性胰腺炎(acute pancreatitis,AP)是指多种病因引起的胰酶激活,继以胰腺局部炎症反应为主要特征,伴或不伴有其他器官功能改变的疾病。临床上,大多数AP患者的病程呈自限性,20%~30%的患者临床过程凶险,病死率可达5%~10%[1]。目前其发病机制尚未完全阐明,研究发现在AP早期,胰腺星状细胞中的促炎因子表达上调[2]。遗传因子特别是AP相关的炎症因子,可能是胰腺损伤甚至是AP严重程度和炎症进展中一个重要的易感因素。单核苷酸多态性(single nucleotide polymorphisms,SNPs)数量巨大,分布广,目前被认为是最有价值的遗传标记[3]。有研究报道肿瘤坏死因子(TNF)-α和热休克蛋白(HSP)70-2基因多态性与多种炎症性疾病有关[4-5],但关于TNF-α和HSP70-2基因多态性与AP易感性的相关研究较少,本研究检测TNF-α及HSP70-2的基因多态性,并探讨其与AP的关系。
1 对象与方法
1.1 研究对象选取2012年6月—2013年2月在我院就诊的发病72 h内的AP患者72例作为AP组,年龄(54.9± 14.1)岁。诊断标准符合中华医学会消化病学分会胰腺疾病学组制定标准[1]及中华医学会外科学会胰腺外科学组制定标准[6]。其中轻型胰腺炎(MAP)30例,重型胰腺炎(SAP)42例。选择同期我院查体健康人71例为对照组,年龄(50.6± 13.9)岁。
1.2 TNF-α及HSP70-2基因多态性检测
1.2.1 引物扩增采研究对象外周血3 mL于EDTA抗凝管。采用经典苯酚-氯仿提取法从全血中提取基因组DNA,溶解于50 μLTE液中,-20℃冰箱保存。参考文献[7]及GenBank设计引物,由Invitrogen公司合成。TNF-α引物:上游5′-AGGCAATAGGTTTTGAGGGCCAT-3′,下游5′-TCCTCCCTGCTCCGATTCCG-3′,扩展片段长度107 bp;HSP70-2引物:上游5′-CAGCAAAGTCCTTGAGTCCC-3′,下游5′-TCCGAAGGACTGGAGCTCTTG-3′,扩展片段长度2 075 bp。TNF-α和HSP70-2 PCR反应体系均为50 μL:取DNA模板1 μL,分别加入TNF-α和HSP70-2引物,然后加入TaqDNA合成酶。扩增条件:(1)TNF-α。95℃预变性5 min;95℃30 s,60℃30 s,72℃45 s,共35个循环,最后72℃延伸10 min;(2)HSP70-2。94℃预变性5 min;95℃1 min,60℃1 min,72℃3 min,共35个循环,最后72℃延伸10 min。
1.2.2 酶切反应取10 μLTNF-αPCR产物加入NcoⅠ限制性内切酶,10 μL HSP70-2 PCR产物加入PstⅠ限制性内切酶,均在37℃恒温水浴锅过夜。于2%琼脂糖凝胶电泳下分析TNF-α酶切产物,1%琼脂糖凝胶电泳下分析HSP70-2酶切产物,与标准DNA Marker比对。
1.3 统计学方法应用SPSS17.0软件包进行统计分析,基因型及等位基因频率采用例(%)表示,组间比较采用χ2检验;计量资料用或M(P25,P75)表示,组间比较采用t检验或非参Z检验,P<0.05为差异有统计学意义。
2 结果
2.1 TNF-α、HSP70-2基因PCR产物酶切结果TNF-α基因PCR产物经NcoⅠ酶切后凝胶电泳结果显示GG型(87 bp+20 bp,由于20 bp太小无法显示,但不影响结果判定)、GA型(107 bp+87 bp+20 bp,图中未见此型)和AA型(107 bp);HSP70-2基因PCR产物经PstⅠ酶切后凝胶电泳结果显示GG型(1 139 bp+936 bp)、GA型(2 075 bp+1 139 bp+ 936 bp)和AA型(2 075 bp),见图1、2。
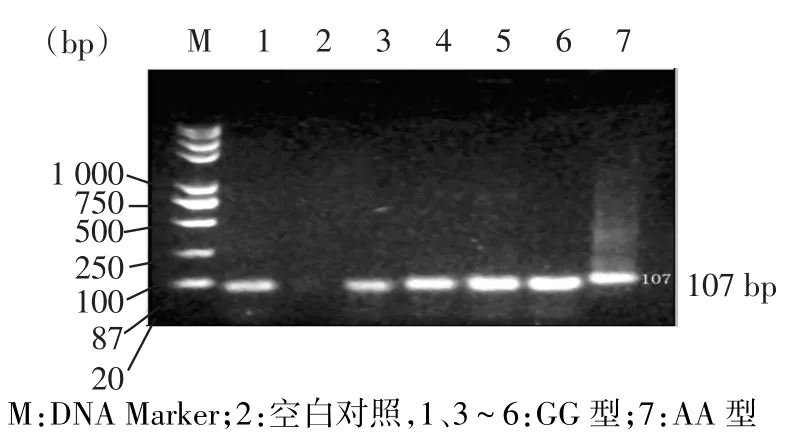
Fig.1TNF-α polymorphism in the result of 2%sepharose electrophoresis图1 TNF-α基因多态性2%琼脂糖凝胶电泳结果
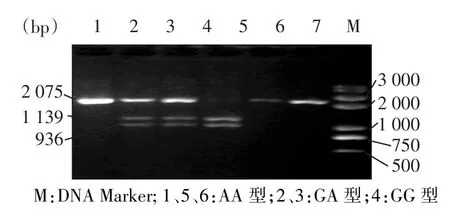
Fig.2HSP70-2 polymorphism in the result of the 1%sepharose electrophoresis图2 HSP70-2基因多态性1%琼脂糖凝胶电泳结果
2.2 TNF-α基因多态性与AP易感性的关系AP组与对照组的TNF-α基因型和等位基因比例间差异无统计学意义,见表1;AP组中,SAP组和MAP组的TNF-α基因型和等位基因间差异无统计学意义,见表2。
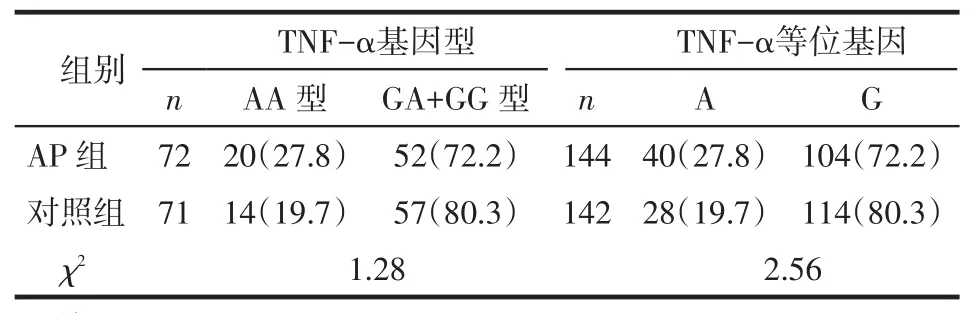
Tab.1Comparison of TNF-α genotype and allele between AP group and control group表1 AP组和对照组TNF-α基因型和等位基因比较例(%)
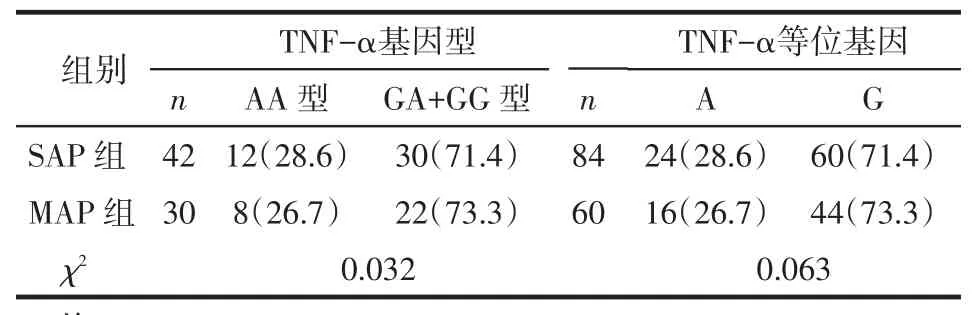
Tab.2Comparison of TNF-α genotype and allele between SAP and MAP groups表2 SAP组和MAP组的TNF-α基因型和等位基因比较例(%)
2.3 不同TNF-α基因型患者的有关临床检验参数比较TNF-α基因AA型与GA+GG型患者的白细胞、CRP、淀粉酶、三酰甘油、血糖差异均无统计学意义,见表3。
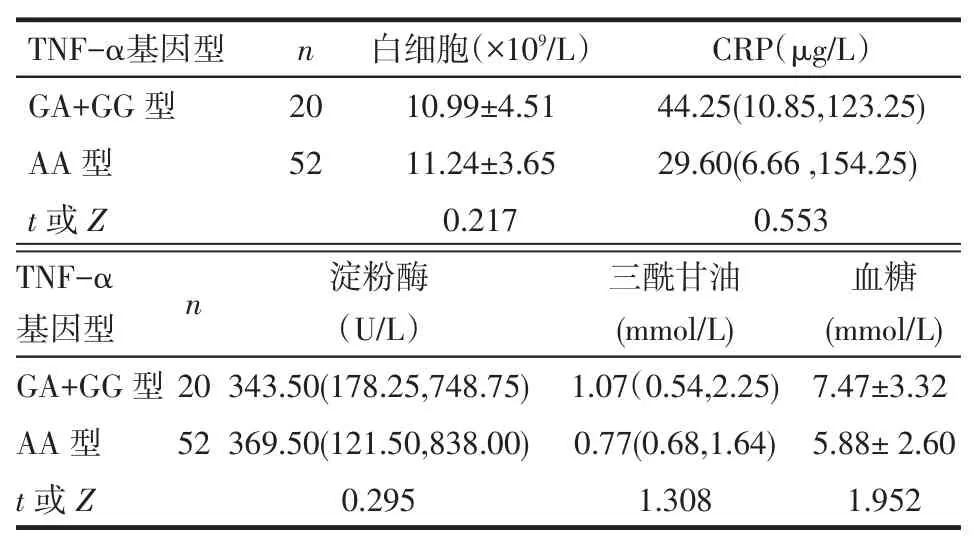
Tab.3Comparison of clinical laboratory parameters between AP patients with different TNF-α genotypes表3 不同TNF-α基因型AP患者的临床检验参数比较
2.4 HSP70-2基因多态性与AP易感性的关系AP组的HSP70-2基因GA+GG型患者比例高于对照组,AP组携带的G等位基因比例高于对照组(均P<0.05),见表4。AP组中,SAP组的GA+ GG型比例高于MAP组;而G等位基因在SAP组和MAP组间无明显差异(P>0.05),见表5。

Tab.4Comparison of HSP70-2 genotype and allele between AP group and control group表4 AP组和对照组HSP70-2基因型和等位基因比较例(%)
2.5 不同HSP70-2基因型患者的有关临床检验参数比较HSP70-2基因AA型与GA+GG型患者的白细胞、血糖、CRP、淀粉酶、三酰甘油差异均无统计学意义,见表6。

Tab.5Comparison of HSP70-2 genotype and allele between SAP and MAP groups表5 SAP组和MAP组HSP70-2基因型和等位基因比较例(%)
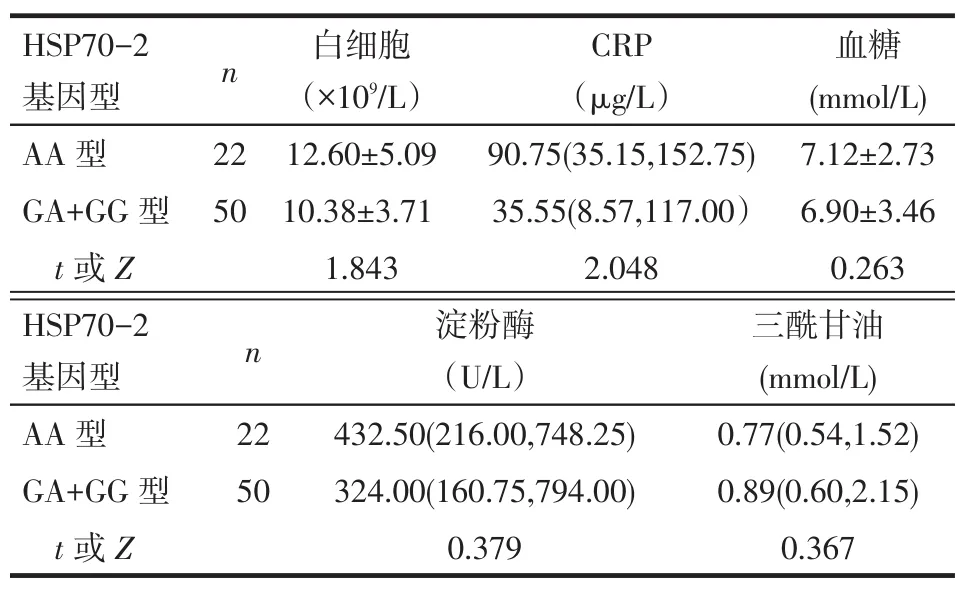
Tab.6Comparison of clinical laboratory parameters between AP patients with different HSP70-2 genotypes表6 不同HSP70-2基因型AP患者的临床检验参数比较
3 讨论
AP是常见的消化系统疾病之一,是因早期炎症使胰腺腺泡中的胰酶过早激活导致自身组织消化的过程[8],其病理过程包括水肿、出血和坏死。TNF-α在AP的血清中是可以被检测出来的。在炎症反应早期,TNF-α可以激活中性粒细胞,促进多种炎症介质释放,在AP的发生发展过程中起重要作用[9]。本研究结果显示:AP组与对照组的TNF-α基因型和等位基因无明显差异;轻症和重症AP间也无明显差异,虽然GG型比例在AP中所占比例较高(72.2%,52/72);且不同基因型的血液检测指标亦无明显差异,提示TNF-α基因的多态性可能与AP发病、严重程度及血液指标无关。与Özhan等[10]、Yang等[11]的研究结论基本一致。但也有不一致的研究,Balog等[7]研究发现TNF-α的308A位点基因多态性是SAP的影响因素,其认为基因型检测可以预测轻重症AP的过程和预后。Dianliang等[12]研究表明TNF-α-308位点多态性与AP不相关,但与AP的脓毒血症相关。以上研究结果的不同可能与不同种族、地域及样本量差异有关,尚需开展多中心、大样本的试验进行研究。
HSP70-2蛋白作为转换蛋白的分子伴侣,参与受损蛋白质的修复,使其恢复活性,从而在蛋白水平起到预防、保护的作用[13],在受到炎症、受热、缺血、缺氧或代谢性毒物等因素刺激时,细胞内迅速表达HSP70-2[14]。本研究结果显示:AP组GA+GG型比例高于对照组;AP组携带G等位基因的比例高于对照组。AP组中SAP的GA+GG型比例高于MAP;而G等位基因在SAP和MAP间无明显差异。Balog等[7]研究发现,重症AP患者携带HSP-70-2等位基因G的比例高于轻症AP患者和健康人群,而具有AA型基因的AP,很少发展为重症胰腺炎,HSP70-2等位基因G是急性重症胰腺炎的危险因素,与本研究结果一致。
[1]Wang XP,Li ZS,Yuan YZ.China guidelines for the diagnosis and treatment of acute pancreatitis(2013,Shanghai)[J].Chinese Journal of Pancreatology,2013(2):73-78.[王兴鹏,李兆申,袁耀宗.中国急性胰腺炎诊治指南(2013,上海)[J].中华胰腺病杂志,2013(2):73-78].
[2]Weiss FU,Simon P,Mayerle J,et al.Germline mutations and gene polymorphism associated with human pancreatitis[J].Endocrinol Metab Clin North Am,2006,35(2):289-302,viii-ix.
[3]Xi SY,Han YL.The characteristics of single nucleotide polymorphism and its application progress inmedicine[J].Medical Journal of Liaoning,2007,21(1):36-39.[席素雅,韩雅玲.单核苷酸多态性的特点及其在医学中的应用进展[J].辽宁医学杂志,2007,21 (1):36-39].
[4]Zeng Z,Duan Z,Zhang T,et al.Association between tumor necrosis factor-α(TNF-α)promoter-308 G/A and response to TNF-α blockers in rheumatoid arthritis:a meta-analysis[J].Modern Rheumatology,2013,23(3):489-495.
[5]Giacconi R,Costarelli L,Malavolta M,et al.Association among 1267 A/G HSP70-2,-308 G/A TNF-α polymorphisms and pro-inflammatory plasma mediators in old ZincAge pop μLation[J].Biogerontology,2014.15(1):65-79.
[6]Zhang SD,Lei RQ.Guidelines for the diagnosis and treatment of severe acutepancreatitis[J].ChineseJournalofsurgery,2007,45(11):727-729.[张圣道,雷若庆.重症急性胰腺炎诊治指南[J].中华外科杂志,2007,45(11):727-729].
[7]Balog A,Gy μLai Z,Boros LG,et al.Polymorphism of the TNF-α,HSP70-2,and CD14 genes increases susceptibility to severe acute pancreatitis[J].Pancreas,2005,30(2):e46-e50.
[8]Gorelick FS,Thrower E.The acinar cell and early pancreatitis responses[J].Clin Gastroenterol Hepatol,2009,7(11 Suppl):S10-14. doi:10.1016/j.cgh.2009.07.036.
[9]Nie JH,Chen WC.Research progress of gene polymorphism and acutepancreatitis[J].ChineseJournalofPancreatology,2007,7(4):271-273[聂锦山,陈卫昌.基因多态性与急性胰腺炎相关研究进展[J].胰腺病学,2007,7(4):271-273.]
[10]Özhan G,Yanar HT,Ertekin C,et al.Polymorphisms in Tumour NecrosisFactorAlpha(TNF)[J].Mediatorsofinflammation,2010.2010.
[11]Yang Z,Qi X,Wu Q,et al.Lack of association between TNF-α gene promoter polymorphisms and pancreatitis:a meta-analysis[J]. Gene,2012,503(2):229-234.
[12]Dianliang Z,Jieshou L,Zhiwei J,et al.Association of plasma levels of tumor necrosis factor(TNF)-alpha and its soluble receptors, two polymorphisms of the TNF gene,with acute severe pancreatitis and early septic shock due to it[J].Pancreas,2003,26(4):339-343.
[13]Duan CC,Chen Q,Zheng MM,et al,The association between heatshockprotein70-2gene polymorphismandcoronaryheartdisease[J]. JournalofChinesePhysician,2010,12(9):1194-1197.[段成城,陈倩,郑美梅等,热休克蛋白70-2(HSP70-2)基因多态性与冠心病的相关性研究[J].中国医师杂志,2010,l2(9):1194-1197].
[14]Lin XW,Yang Y.Heat shock protein 70-2 gene polymorphism and susceptibility to diabetic nephropathy[J].Med J Chin PLA,2014,39 (11):898-901.[林新伟,杨阳.HSP70-2基因多态性与糖尿病肾病易感性的关系[J].解放军医学杂志,2014,39(11):898-901].
(2014-07-15收稿2014-09-02修回)
(本文编辑闫娟)
Polymorphisms of TNF-α gene and HSP70-2 gene in patients with acute pancreatitis
HU Jiaping,ZHUANG Jianxin△,LI Yong,YU Yonghuan,HU Qinghong,LAI Yinying,WU Antao
The First Affiliated Hospital of Nanchang University,Nanchang 330006,China△
ObjectiveTo investigate the association of tumor necrosis factor(TNF)-α,heat shock protein(HSP)70-2 gene polymorphisms and susceptibility of acute pancreatitis(AP).MethodsUsing case-control method,The gene polymorphism of TNF-α and HSP70-2 was detected by PCR-RLFP in 72 patients with AP and 71 healthy controls.Results There were no significant differences in proportion of TNF-α genotype and alleles between AP and control groups(P>0.05). There were no significant differences in TNF-α genotype and alleles between severe acute pancreatitis(SAP)and light acute pancreatitis(MAP)of AP group(P>0.05).There were no significant differences in white blood cell count,C-reactive protein(CRP),amylase,three acyl glycerin and glucose between TNF-a and HSP70-2 gene of AA type and GA+GG type patients(P>0.05).The HSP70-2 genotype GA+GG proportion was significantly higher in AP group than that of control group(69.4%vs 49.3%).The ratio of patients with G allele was significantly higher in AP group than that of control group(46.5% vs 31.7%).The ratio of patients with GA+GG type AP was significantly higher in SAP patients than that of MAP patients of AP group(81.0%vs 53.3%).There was no significant difference in G allele between SAP and MAP patients(P>0.05). ConclusionTNF-α polymorphisms is not associated with acute pancreatitis.There is an association between HSP70-2 polymorphisms and acute pancreatitis.Carrying the G allele increases the possibility of a severe acute pancreatitis,which is one of the genetic susceptibility factors of severe acute pancreatitis.
tumor necrosis factor-alpha;HSP70 heat-shock proteins;pancreatitis;genetic polymorphism;HSP70-2;polymorphism,restriction fragment length;polymerase chain reaction
R576
A
10.3969/j.issn.0253-9896.2015.01.015
江西省科技厅支撑计划
南昌大学第一附属医院普外科五病区(邮编330006)
胡家平(1967),男,副主任医师,副教授,硕士生导师,硕士,主要从事胃肠肿瘤研究
△通讯作者E-mail:zjx136@qq.com