Neural correlates of the Heidelberg Music Therapy: indicators for the regeneration of auditory cortex in tinnitus patients?
2015-12-15ChristophM.Krick,HeikeArgstatter
Neural correlates of the Heidelberg Music Therapy: indicators for the regeneration of auditory cortex in tinnitus patients?
Tinnitus, the phenomenon of ringing or buzzing in the ears without an external sound source is one of the most commonly reported symptoms in otorhinolaryngology and aff ects 10 –15% of the general population. Models have been developed to account for neural basis of tinnitus, its pathogenesis and its consequences on mental health (deRidder et al., 2013). In most cases tinnitus onset follows a partial hearing impairment. Peripheral sensory deprivation due to cochlear damages may prompt increased neuronal activity in the central auditory system in order to adapt the neural sensitivity to the reduced sensory inputs. This central gain could over amplify the “neural noise” and thus trigger a homeostatic down-regulation of inhibitory synapses in the auditory cortical map leading to specifi c reorganization of the cortical representation of the tinnitus percept. Dysfunctional feedback connections from limbic regions to auditory brain areas, interacting at the thalamic level, may account for the psychological impairment.
Tinnitus research has led to a variety of prospective treatment options. Most promising of these are treatments which incorporate psychotherapeutic elements and auditory stimulation procedures (Grewal et al., 2014). However, the meaning of “therapy success” does not imply complete disappearance of the tinnitus sound. The aim of tinnitus-related interventions is the attenuation of the tinnitus percept and/or habituation processes to decrease the psychological suff ering. There is as yet no permanent treatment for a neural down-regulation of processes maintaining this auditory self-excitation. On the website of the American Tinnitus Association (ATA) it states: “We know you are looking for a cure to end that suffering. But we want to tell you that no matter what anyone tells you, there is currently no cure for the condition.”
Schecklmann et al. (2013) showed that the extent of tinnitus distress is correlated with gray matter (GM) loss in the auditory cortex during ongoing tinnitus percept. This fi nding was derived from a large cross-sectional sample of 257 patients suffering from chronic tinnitus and it was replicated in a second sample of additional 78 patients. As tinnitus impact causes GM loss in auditory cortex, inverse changes in the same areas seem plausible for tinnitus treatment. Although such reorganization may alleviate the phantom sound sensation, its realization seems futuristic. Since the brain is an informationally isolated system, managing brain functions externally has only small or transient eff ects. Thus commonly used masker devices come with the disadvantage of lengthy application and they only offer the passive “sounding” of the tinnitus as long as they were applied. One way to aff ect the brain may be the therapeutic use of repetitive transcranial magnetic stimulation (rTMS). The eff ects of rTMS on the left temporoparietal cortex in tinnitus patients has been shown to be temporary eff ective (Lefaucheur et al. 2014). Another approach consists of therapeutic regimes aiming at neuronal reorganization by means of neuro-psychotherapeutic interventions that use principles of neural self-organization. The tinnitus’ self-excitation seems best accessible by inner neural pathways of acoustic learning, attention control, and emotional processing.
Sound therapies may also alleviate the perception of tinnitus (Hoare et al. 2013). Their underlying notion is the desynchronization of the pathologically increased neuronal synchrony leading to tonotopic changes in the auditory cortex using music. The German Center for Music Therapy Research (DZM e.V.) promotes a music therapeutic approach: the Heidelberg Model of Neuro-Music Therapy. It stems from a ten-year eff ort of therapy development and its evaluation using questionnaires, electrophysiological examination and Magnet Resonance Imaging (MRI). The Neuro-Music Therapy integrates a number of strategies to manage the psychological state of the patient and to restore the underlying neuronal circuits. To do so, complementary music- and psychotherapeutic interventions and techniques are structured into modules. The therapy protocol consists of nine 5-minute sessions of individualized therapy over a period of fi ve consecutive days, comprising acoustic training for frequency discrimination, auditory attention control tasks, and guided exercises for mindfulness and distress regulation. A detailed description of the therapy can be found in Argstatter et al. (2015). Compared to sound-based approaches using passive listening, during the Heidelberg Neuro-Music Therapy the patients are confronted actively with their individual tinnitus sounds. There are fi ve important strategies: (i) The patients are told to focus on their tinnitus explicitly instead of trying to ignore it; (ii) the music therapy makes use of specifi c tonal material, matched to the individual’s tinnitus frequency; (iii) the main parts of the therapy consist of active music therapy modules, meaning that there is no need and no purpose for spectrally changing the music used, which facilitates the application of the treatment considerably; (iv) it is important to ensure the training regime is intrinsically motivating and active music therapy guarantees the lasting co-operation of the patients forcing self-organization processes in the brain; and (v) the duration of the music therapy does not exceed 5 consecutive training days and is thus extremely short. However, this therapy is limited to patients without severe hearing impairment allowing the participation in the musically guided sessions.
Over 1,200 patients suffering from chronic tinnitus have undergone the Neuro-Music Therapy in the last 10 years. Overall, about 80% of them experienced a reliable improvement of symptoms (‘responder’), both in participants in controlled clinical trials and in participants in daily clinical sessions in the outpatient department at the DZM e.V. The therapy has shown long-term eff ects despite the short intervention interval (Argstatter et al., 2012). Similar clinical therapeutic eff ects in patients with recent onset tinnitus have been reported by Grapp et al. (2013).
The previously observed long-term eff ects of the Heidelberg Neuro-Music Therapy have led to the hypothesis that structural reorganization can be expected as a neural correlate of clinical improvement. High resolution MRI scans were performed on two subsequent weekends to investigate longitudinal structural changes (Krick et al., 2015). Tinnitus-related mental load, i.e., distress, was measured using the Tinnitus Questionnaire (TQ) (Goebel and Hiller, 1998) before and after therapy. At the time of including the patients, they reported mean strain of 37.3 ± 16.1 points on TQ scale. Time since tinnitus onset was 4.9 ± 2.1 weeks. The patients fi rst underwent standard clinical treatment for acute tinnitus. Cases with tinnitus remission during this phase were excluded from further therapy. Finally 41 patients still suff ering from the recent onset tinnitus accepted to undergo
the Neuro-Music therapy. In order to observe therapy-related eff ects, the patients were randomly divided into two groups, a treatment group (TG) and a waiting group of passive tinnitus controls (PTC). Tinnitus distress and tinnitus duration was controlled in both groups. At the time of MRI, mean tinnitus duration was 8.14 ± 1.85 weeks in TG and 8.10 ± 1.45 weeks in the PTC group. Twenty-two healthy participants also underwent the music therapy as active controls (AC) in order to analyze the tinnitus-related therapy eff ects by comparing the scans with the treatment group. All participants had age-appropriate hearing levels and reported no otological or psychological comorbidity. The three groups did not diff er in sex (females 43%) or age (mean 41.6 ± 11.8 years).

Figure 1 Both TG and AC experienced hearing exercises and relaxation techniques over 1 week.
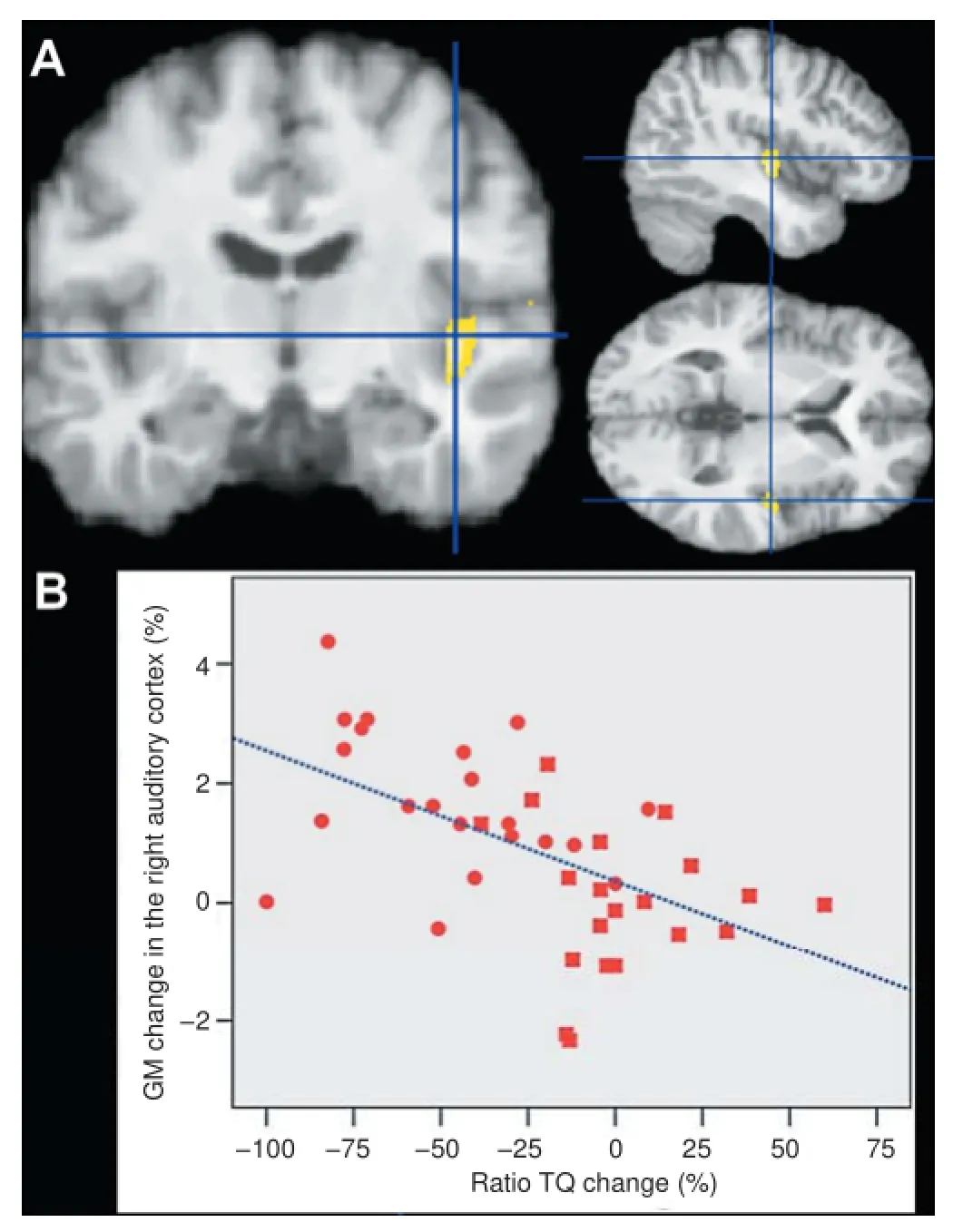
Figure 2 Specifi c therapy eff ect.
Between the MRI sessions with delay of 1 week, the treatment group and the active controls were treated with the Neuro-Music therapy according to the Heidelberg Model. Participants in the PTC group did not receive any intervention during the study week (but after). On the psychological level, the therapy signifi cantly reduced the TQ score in the treatment group compared to the PTC group (df = 1; F = 22.9; MSE = 1,374; P< 0.00005). Brain reorganization was calculated by longitudinal Voxel-Based Morphometry (VBM). The infl uence of the treatment on GM density was contrasted between the groups using a repeated measures analysis of variance. Therapy-induced GM changes were derived from the contrast between the treatment group and the PTC. Specifi c tinnitus-related GM changes were calculated from contrast between the treatment group and active controls, each experiencing the same treatment, respectively. In both groups the 1-week therapy yielded GM increase in the precuneus (see Figure 1) which is involved in the neural network for self-perception and distress regulation (de Ridder et al. 2013). Only the treatment group showed a GM increase in the right primary auditory cortex, comprising the right Heschl’s gyrus (see Figure 1). The intersection between specific tinnitus-related structural eff ects and therapy-induced brain alterations revealed a signifi cant right-lateralized GM increase in the right auditory cortex, especially in the location of the right Heschl’s gyrus (MNI coordinates 44/–12/–5) as shown in Figure 2A. This specifi c tinnitus-related structural GM increase and the TQ reduction led to the hypothesis that the therapy inversely involved the distress-sensitive auditory structures as described by Schecklmann et al. (2013). The localization of this specifi c improvement-related structural enhancement is partially in line with the fi ndings of Schecklmann et al. (2013) which were located in similar coordinates (left: 44/–12/-11, right: 46/–15/–6). However, this structural overlap concerns the right hemisphere only. It is worth noting that the sign of slope was inverted between both observations.
In the current study, we also aimed to describe the corresponding neural correlates of the distress dependency of the primary auditory cortex in tinnitus patients more thoroughly. Beyond the structural group diff erences as detailed in Krick et
al. (2015) we therefore focused on individual changes of distress and GM, too. The rate of TQ decrease was inversely correlated (Spearman-Rho= –0.59; P < 0.0001) with the GM increase at the right Heschl’s gyrus (see Figure 2B). A regression analysis with the dependent value of individual GM change in the Heschl’s gyrus revealed signifi cant infl uences from relative TQ change only, but there was no interaction with age, gender, or initial TQ. The resulting regression model (F = 4.35; df = 4; P< 0.01) can explain about 33% of the variance regarding the magnitude of reorganization in the right Heschl’s gyrus. This result underlines the general relationship between tinnitus distress and GM density in the auditory cortex by means of longitudinal measurements. These results are compatible with the cross-sectional fi ndings reported by Schecklmann et al. (2013), but they also provide insight into the speed of the reorganization process.
The observations regarding distress-related GM loss in the auditory cortex and the therapy-induced GM increase could be viewed as two sides of the same coin. The two inversely related eff ects concern the same brain structure that is involved in both tinnitus distress and its clinical improvement. In each case, the self-perceived tinnitus distress seemed to be dependent on the extent of gray matter changes in the auditory cortex. Although the processes on cellular level cannot be identifi ed by the current methods, the macroscopic structural eff ects may have reversed the pathophysiological generation of tinnitus distress located within the auditory areas. Further evidence for the involvement of the auditory areas comes from the common observation that the phantom noise changes its pitch before it begins to mute in the course of the Neuro-Music Therapy (Hutter et al., 2014).
The fi nding of lateralized structural brain changes are diffi -cult to account for, though they may be explained by the therapy strategies applied in the Neuro-Music Therapy that is tailored to the individual’s tinnitus pitch. Since spectral processing of the acoustic percept predominantly involves right auditory areas (Doeller et al., 2003), there is an interplay with the main components of the training that depend on the patients’ ability to discriminate auditory stimuli. This current limitation to right dominant eff ects yields potential for future development.
The results of structurally managing the auditory cortex may open a door to new strategies towards remission of tinnitus-based brain irritations, though only a small percentage of patients reported a complete remission of their tinnitus sensation. However, the observed reorganization of the crucial auditory brain region, which was once impaired by tinnitus, may now yield an explanatory model for the sustained therapy success. Regarding our patients’ suff ering from recent-onset tinnitus, it seems that the prolonged therapy eff ects caused by neural reorganization may be able to prevent tinnitus from chronifi cation (Grapp et al., 2013).
In conclusion, this musically guided therapy option may lead to the rapid neural regeneration of the tinnitus core by distinct focal reorganization of the underlying neural circuits. Thus, these indicators of auditory cortical map regeneration give hope that the statement with respect to a cure for tinnitus on the American Tinnitus Association website may need to be revised some day.
The study was supported by KTS Klaus Tschira Stiftung gGmbH. And many thanks to Dr. Carrie Ankerstein for stylistic and linguistic improvement of this paper.
Christoph M. Krick*, Heike Argstatter
Department of Neuroradiology, Saarland University Hospital, D-66241 Homburg, Germany (Krick CM)
German Center for Music Therapy Research (Viktor Dulger Institute) DZM, D-69123 Heidelberg, Germany (Argstatter H)
*Correspondence to: Christoph M. Krick, Ph.D.,
christoph.krick@uniklinikum-saarland.de.
Accepted: 2015-06-16
Argstatter H, Grapp M, Hutter E, Plinkert P, Bolay HV (2015) The effectiveness of Neuro-Music Therapy according to the Heidelberg model compared to a single session of educational counselling as treatment for tinnitus: a controlled trial. J Psychosom Res 78:285-292.
Argstatter H, Grapp M, Hutter E, Plinkert P, Bolay HV (2012) Long-term effects of the “Heidelberg Model of Music Therapy” in patients with chronic tinnitus. Int J Clin Exp Med 5:273-288.
De Ridder D, Vanneste S, Weisz N, Londero A, Schlee W, Elgoyhen AB, Langguth B (2013) An integrative model of auditory phantom perception: Tinnitus as a unifi ed percept of interacting separable subnetworks. Neurosci Biobehav Rev 44C:16-32.
Doeller CF, Opitz B, Mecklinger A, Krick C, Reith W, Schröger E (2003) Prefrontal cortex involvement in preattentive auditory deviance detection: neuroimaging and electrophysiological evidence. NeuroImage 20:1270-1282.
Goebel G, Hiller W (1998) Tinnitus-Fragebogen: (TF); ein Instrument zur Erfassung von Belastung und Schweregrad bei Tinnitus; Handanweisung. Göttingen, Hogrefe Verl. für Psychologie.
Grapp M, Hutter E, Argstatter H, Plinkert PK, Bolay HV (2013) Music therapy as an early intervention to prevent chronifi cation of tinnitus. Int J Clin Exp Med 6:589-593.
Grewal R, Spielmann PM, Jones SE, Hussain SS (2014) Clinical efficacy of tinnitus retraining therapy and cognitive behavioural therapy in the treatment of subjective tinnitus: a systematic review. J Laryngol Otol 128:1028-1033.
Hoare DJ, Adjamian P, Sereda M, Hall DA (2013) Recent technological advances in sound-based approaches to tinnitus treatment: a review of effi -cacy considered against putative physiological mechanisms. Noise Health 15:107-116.
Hutter E, Grapp M, Argstatter H, Bolay HV (2014) Music therapy for chronic tinnitus: variability of tinnitus pitch in the course of therapy. J Am Acad Audiol 25:335-342.
Krick CM, Grapp M, Daneshvar-Talebi J, Reith W, Plinkert PK, Bolay HV (2015) Cortical reorganization in recent-onset tinnitus patients by the Heidelberg Model of Music Therapy. Front Neurosci 9:49.
Lefaucheur JP, André-Obadia N, Antal A, Ayache SS, Baeken C, Benninger DH, Garcia-Larrea L (2014) Evidence-based guidelines on the therapeutic use of repetitive transcranial magnetic stimulation (rTMS). Clin Neurophysiol 125:2150-2206.
Schecklmann M, Lehner A, Poeppl TB, Kreuzer PM, Rupprecht R, Rackl J, Burger J, Frank E, Hajak G, Langguth B, Landgrebe M (2013) Auditory cortex is implicated in tinnitus distress: a voxel-based morphometry study. Brain Struct Funct 218:1061-1070.
10.4103/1673-5374.165220 http://www.nrronline.org/
Krick CM, Argstatter H (2015) Neural correlates of the Heidelberg Music Therapy: indicators for the regeneration of auditory cortex in tinnitus patients? Neural Regen Res 10(9):1373-1375.
杂志排行

中国神经再生研究(英文版)的其它文章
- PTEN inhibition and axon regeneration and neural repair
- Neurochemical plasticity of Müller cells after retinal injury: overexpression of GAT-3 may potentiate excitotoxicity
- The choline pathway as a strategy to promote central nervous system (CNS) remyelination
- Enhancing endogenous stem cells in the newborn via delayed umbilical cord clamping
- Elastic modulus aff ects the growth and diff erentiation of neural stem cells
- Non-steroidal anti-infl ammatory drugs (NSAIDs) and neuroprotection in the elderly: a view from the mitochondria