Nonintubated uniportal video-assisted thoracoscopic surgery for primary spontaneous pneumothorax
2015-10-31ShubenLiFeiCuiJunLiuXinXuWenlongShaoWeiqiangYinHanzhangChenJianxingHe
Shuben Li, Fei Cui, Jun Liu, Xin Xu, Wenlong Shao, Weiqiang Yin, Hanzhang Chen, Jianxing He
1The First Clinical College, Southern Medical University, Guangzhou 510515, China;2Department of Cardiothoracic Surgery, The First Affiliated Hospital of Guangzhou Medical University, Guangzhou 510120, China
Correspondence to: Professor Jianxing He, MD, PhD, FACS. Department of Cardiothoracic Surgery, The First Affiliated Hospital of Guangzhou Medical University, 151 Yanjiang Road, Guangzhou 510120, China. Email: drjianxing.he@gmail.com.
Nonintubated uniportal video-assisted thoracoscopic surgery for primary spontaneous pneumothorax
Shuben Li1,2, Fei Cui2, Jun Liu2, Xin Xu2, Wenlong Shao2, Weiqiang Yin2, Hanzhang Chen2, Jianxing He2
1The First Clinical College, Southern Medical University, Guangzhou 510515, China;2Department of Cardiothoracic Surgery, The First Affiliated Hospital of Guangzhou Medical University, Guangzhou 510120, China
Correspondence to: Professor Jianxing He, MD, PhD, FACS. Department of Cardiothoracic Surgery, The First Affiliated Hospital of Guangzhou Medical University, 151 Yanjiang Road, Guangzhou 510120, China. Email: drjianxing.he@gmail.com.
Objective: The objective of the current study was to evaluate the feasibility and safety of nonintubated uniportal video-assisted thoracoscopic surgery (VATS) for the management of primary spontaneous pneumothorax (PSP).
Methods: From November 2011 to June 2013, 32 consecutive patients with PSP were treated by nonintubated uniportal thoracoscopic bullectomy using epidural anaesthesia and sedation without endotracheal intubation. An incision 2 cm in length was made at the 6thintercostal space in the median axillary line. The pleural space was entered by blunt dissection for placement of a soft incision protector. Instruments were then inserted through the incision protector to perform thoracoscopic bullectomy. Data were collected within a minimum follow-up period of 10 months.
Results: The average time of surgery was 49.0 min (range, 33-65 min). No complications were recorded. The postoperative feeding time was 6 h. The mean postoperative chest tube drainage and hospital stay were 19.3 h and 41.6 h, respectively. The postoperative pain was mild for 30 patients (93.75%) and moderate for two patients (6.25%). No recurrences of pneumothorax were observed at follow-up.
Conclusions: The initial results indicated that nonintubated uniportal video-assisted thoracoscopic operations are not only technically feasible, but may also be a safe and less invasive alternative for select patients in the management of PSP. This is the first report to include the use of a nonintubated uniportal technique in VATS for such a large number of PSP cases. Further work and development of instruments are needed to define the applications and advantages of this technique.
Uniportal; video-assisted thoracoscopic surgery (VATS); spontaneous pneumothorax
Introduction
Video-assisted thoracoscopic surgery (VATS) has been reported to offer substantial clinical advantages compared to open surgery for many clinical conditions (1). Regarding primary spontaneous pneumothorax (PSP), several studies have shown that the VATS procedure is as effective as thoracotomy in terms of recurrence and complication rate (2). In the context of minimally invasive thoracic surgery,uniportal VATS represents one of the most recent evolutions. With the aim of further reducing the invasiveness of VATS, Rocco and colleagues demonstrated that treatment of PSP using uniportal VATS was feasible and, compared with the conventional (3-portal)VATS, resulted in less postoperative pain, paraesthesia,postoperative drainage duration, postoperative stay, and hospital costs (3).
Currently, general anaesthesia with one-lung intubated ventilation is the standard anaesthesia in thoracic surgery. Intubated anaesthesia is often associated, however, with postoperative throat discomfort, including irritating cough,as well as throat pain in some patients. Nonintubatedanaesthesia can reduce general anaesthesia-related complications; therefore, many investigators have begun to explore its application in general thoracic surgery (4). Two examples of such groups are Dong et al. who reported that thoracoscopic wedge resection under nonintubated anaesthesia was both feasible and safe (5), and Chen et al.,who reported the safety and feasibility of thoracoscopic resection under nonintubated anaesthesia in 285 patients (6).
The combination of uniportal VATS and nonintubated anaesthesia is potentially a less invasive operation in the management of PSP. This is the first report to include a large number of records on the use of a nonintubated uniportal technique in VATS for PSP.
Patients
This study was reviewed and approved by the First Affiliated Hospital of Guangzhou Medical University Research Ethics Committee. From November 2011 to June 2013, VATS was performed for PSP in our department using a singleincision and non-rib-spreading approach. The same group of thoracic surgeons and anaesthesiology team performed all of the operations. Data from 32 consecutive patients(28 males and 4 females) who received this operation were analysed (Table 1).
Materials and methods
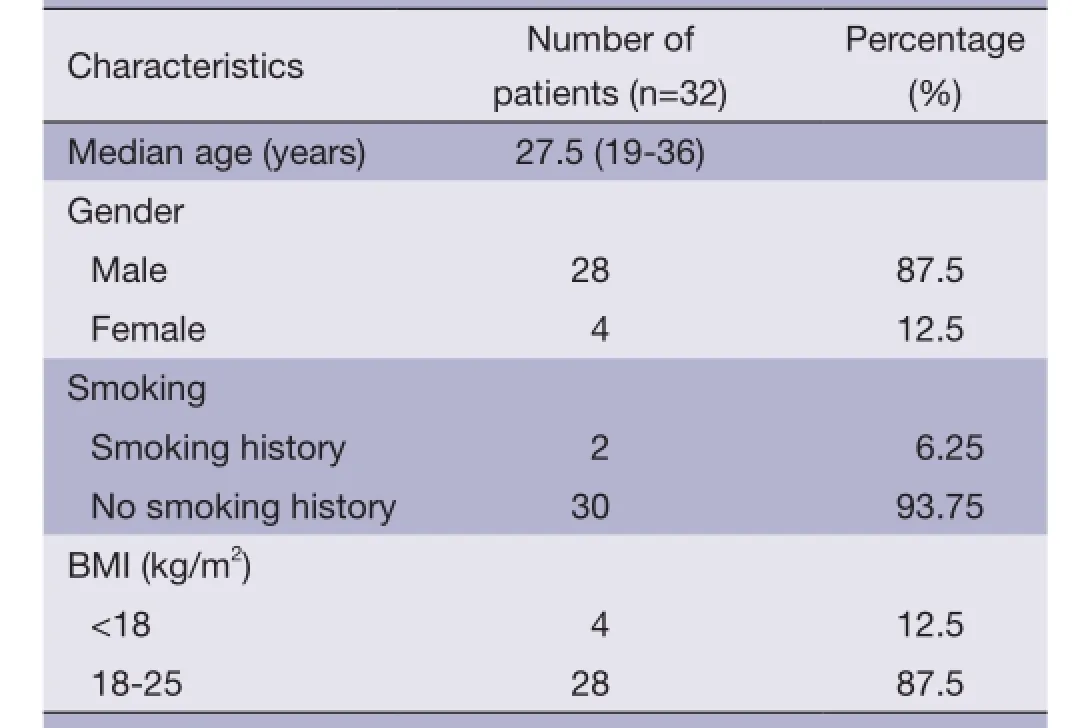
Table 1 Patient characteristics
Patients were eligible for the procedure if their CT scan demonstrated unilateral apical bullae, if they had an American Society of Anesthesiologists (ASA) grade of I-II and a body mass index (BMI) <25, and had no evident airway secretions or contraindications for epidural puncture in the preoperative anaesthesia assessment.
Surgical technique
Administration of anaesthesia
After establishing intravenous rehydration, an epidural catheter was inserted in the thoracic T6-7 space. With the patient in the supine position, 2 mL of 2% lidocaine was injected through the epidural catheter. If signs of spinal anaesthesia were not present within 5 min, fractionated injection of 12 mL 0.375% ropivacaine was performed. Prior to surgery, an anaesthesia level between T2 and T10 had to be achieved. Propofol and remifentanil were infused for sedation and anaesthesia during surgery, and bispectral index values were maintained between 40 and 60. During the surgery, masked and nasopharyngeal airway assisted ventilation were provided with a fraction of inspired oxygen(FiO2) concentration of 0.33. The hilum and waist were padded to widen the intercostal space further. To reduce coughing induced by pulling on the lung tissue, and to ensure a steady surgical environment, 6 mL of 2% lidocaine was sprayed on the surface of the lung under thoracoscopic guidance in the chest cavity. The use of lidocaine on the lung surface eliminated the need for blocking of the vagus nerve.
Surgical management
All video-assisted thoracic operations were performed using a Stryker 1288 HD 3-Chip Camera/1288 (Stryker,USA) with a three-chip HD camera system, in addition to endoscopic instruments specially designed by our department. We created a 2 cm incision at the level of the 6thintercostal space in the median axillary line, after which a soft incision protector was placed into the space as the surgical operation channel. A 5 mm 30° video thoracoscope and two laparoscopic instruments (Roticulator™ and Endo Grasp™, USSC-Tyco Healthcare and Endo GIA Universal,Johnson & Johnson, USA) were introduced through this channel.
By deploying the articulating arm, the target bullae were identified and resected with 2-3 firings of blue cartridges. For all procedures, the video thoracoscope lay between the operative instruments, but shifts may have occurred during the procedure. Thus, the relative position was best determined by a geometric approach to the target area. The specimen was usually extracted through an endobag, after which the incision protector was removed, and an 18 Frchest tube was introduced under direct camera visualization,and placed in the pleural apex. The chest tube was removed after air leak stopped, and an X-ray of the chest demonstrated a well-expanded lung. The patients were observed overnight, and discharged the following morning.
Results
During a telephone interview, all patients provided answers to a questionnaire regarding pain and satisfaction scores. The mean postoperative follow-up time was 14.5 months with a minimum follow-up of 10 months (range, 10-19 months). Neither the signs nor the symptoms of recurrent pneumothorax were observed in any patients.
The median operative time was 49.0 min (range, 33-65 min). The necessity to convert the uniportal VATS procedure to a standard 3-port VATS procedure or a thoracotomy was not encountered. Further, no major complications were observed, and the administration of opiates was not required. The postoperative feeding time was 6 h. The median chest drainage time was 19.3 h (range,15-26 h). All patients were discharged after a median hospital stay of 41.6 h (range, 26-47 h). Variables contained in the prospective dataset included operation length,intraoperative blood loss, postoperative feeding time,drainage volume, drainage time, postoperative hospital stay,and pain scores (Table 2).

Table 2 Intra- and post-operative conditions of uniportal VATS
Discussion
Currently, VATS is reported to be as effective as thoracotomy, and entails less associated morbidity. In an attempt to reduce complications, conventional VATS has developed to include either smaller working ports and instrumentation, or fewer incisions. Rocco and colleagues first described the uniportal VATS technique as an effective approach to the safe performance of wedge resections for pulmonary lesions (7).
Compared with general anaesthesia performed in a traditional thoracic surgery, nonintubated anaesthesia reduces intubation-related complications, and facilitates timely patient mobility (8). With nonintubated anaesthesia,coughing induced by postoperative throat discomfort is significantly reduced (9). Further, coughing may worsen wound pain, which in turn suppresses the cough reflex,making pulmonary secretions difficult to discharge after surgery. Additionally, nonintubated endoscopic resection may reduce the required dose of intraoperative anaesthetic drugs, which may help protect breathing and digestive functions.
In 4-6 h after non-intubated segmental resection, patients could start eating, drinking, and could get out of bed. The absence of general anaesthesia and double-lung ventilation,in combination with the reduction of postoperative hospital days, could decisively shift the balance in the management of PSP toward uniportal VATS.
At present, nonintubated anaesthesia, combined with uniportal VATS bullectomy, is one of the most minimally invasive surgeries, but only a limited number of reports have been published regarding this procedure. According to the literature (10-15), most previous uniportal VATS were performed under general anaesthesia. Only one procedure, conducted by Rocco et al., was performed while the patient was conscious (16). The procedure described by Rocco et al. was performed using a 5 mm 0° thoracoscope,an endostapler, and grip forceps, with which they resected blebs or bullae in the lung apex. In a separate study, Gigirey et al. reported some disadvantages including quality of vision; however, problems related to quality of vision are not an issue if a 30° thoracoscope and an incision protector are used (17). Additionally, the absence of any protected channels for introducing the material into the cavity can lead to intercostal nerve injury, as well as increase the need to clean the optical lenses and consequently delay the operative time.
Tsai et al. (18) performed a vagus nerve block during nonintubated VATS. In the current study, however, it was not necessary for us to perform this procedure, which raises the risks of damage to adjacent vessels. Instead, we sprayedapproximately 6 mL of 2% lidocaine onto the surface of lung. Using the latter method, we found that the cough reflex could be effectively abolished without affecting the heart rate, breathing rate, or blood pressure. Further, we believe that this novel technique is safer than performing a vagus nerve block.
Reports from eight different authors regarding patients who received bullectomy for PSP, including the present report, were divided into four different groups (A-D) for a comparison of duration of chest drainage, postoperative feeding time, and postoperative hospital stay (Table 3). Patients in group A received conventional (3-port) VATS under general anaesthesia, and had the longest duration of chest drainage,postoperative feeding time, and postoperative hospital stay of the four groups. Group B patients also received conventional (3-port) VATS, but under nonintubated anaesthesia. Data from group B was similar to that of group A, except for postoperative feeding time, which was significantly reduced and similar to group D patients,who also underwent nonintubated anaesthesia. Group C received uniportal VATS under general anaesthesia. Postoperative feeding time was similar to that of group A,while duration of chest drainage was the same as group D. The postoperative hospital stay of group C patients was also slightly less when compared to group A.
Finally, group D patients underwent a combination of uniportal VATS under nonintubated anaesthesia, Rocco et al. reported only one case, and did not use an incision protector. In contrast, we have reported 32 cases, each of which involved the use of a soft incision protector. The mean operative time of group D was comparable to all other groups; however, the combination of the other scores was less than values observed in the other three groups. Specifically, both the postoperative feeding time and hospital stay were less in group D patients than in group A and C subjects, while both duration of chest drainage and postoperative hospital stay were less in group D than in groups A and B.
Passlick et al. (21) demonstrated that about a third of all patients who underwent minimally invasive surgeryexperienced chronic pain. Sihoe et al. (22) found that over 50% of patients who underwent VATS for PSP complained of distinct paraesthesia resulting from wound pain. In each of our 32 cases, we chose the use of a soft incision protector instead of a trocar to safeguard the surgical operation channel. We observed moderate chest wall pain in two patients (6.25%), which was a lower rate than previously reported (35%) for the uniportal no-trocar technique (12). It is possible that the use of an incision protector in VATS procedures shields the intercostal nerves from compression due to torqueing of the camera or instruments, and therefore reduces the rate of residual chest wall paraesthesia. It is our opinion that using a smaller soft incision protector could further reduce the intensity of postoperative pain. The incidence of chronic postoperative pain in our uniportal group was less than that of the 3-port group (3). We believe this to be an effect of the potential advantages of using only one intercostal space, as well as a soft incision protector. By reducing the number of ports and using smaller instruments without trocars, the risk of traumatizing the intercostal nerves was decreased. Further,the potential reduction in intercostal nerve trauma was apparent by the fact that the administration of opiates was not necessary during the performance of procedures in the current study, and patients did not require any painkillers after surgery.

Table 3 Comparison of intraoperative and postoperative variables between bullectomy groups
We acknowledge that the study was limited by the lack of a control group. Further studies and follow-up are needed to verify the benefits of nonintubated uniportal VATS for PSP. Nevertheless, our initial results indicate that nonintubated uniportal VATS is technically feasible,and may be a safe and less invasive alternative for the management of PSP.
Acknowledgements
The authors are grateful for Professor Guangqiao Zeng(State Key Laboratory of Respiratory Disease and National Clinical Center for Respiratory Disease, China) for his assistance in preparing this paper.
Disclosure: The authors declare no conflict of interest.
1. Lang-Lazdunski L, Chapuis O, Bonnet PM, et al. Videothoracoscopic bleb excision and pleural abrasion for the treatment of primary spontaneous pneumothorax: long-term results. Ann Thorac Surg 2003;75:960-5.
2. Shaikhrezai K, Thompson AI, Parkin C, et al. Videoassisted thoracoscopic surgery management of spontaneous pneumothorax--long-term results. Eur J Cardiothorac Surg 2011;40:120-3.
3. Jutley RS, Khalil MW, Rocco G. Uniportal vs standard three-port VATS technique for spontaneous pneumothorax: comparison of post-operative pain and residual paraesthesia. Eur J Cardiothorac Surg 2005;28:43-6.
4. Chen JS, Cheng YJ, Hung MH, et al. Nonintubated thoracoscopic lobectomy for lung cancer. Ann Surg 2011;254:1038-43.
5. Dong Q, Liang L, Li Y, et al. Anesthesia with nontracheal intubation in thoracic surgery. J Thorac Dis 2012;4:126-30.
6. Chen KC, Cheng YJ, Hung MH, et al. Nonintubated thoracoscopic lung resection: a 3-year experience with 285 cases in a single institution. J Thorac Dis 2012;4:347-51.
7. Rocco G, Martin-Ucar A, Passera E. Uniportal VATS wedge pulmonary resections. Ann Thorac Surg 2004;77:726-8.
8. Tseng YD, Cheng YJ, Hung MH, et al. Nonintubated needlescopic video-assisted thoracic surgery for management of peripheral lung nodules. Ann Thorac Surg 2012;93:1049-54.
9. Wu CY, Chen JS, Lin YS, et al. Feasibility and safety of nonintubated thoracoscopic lobectomy for geriatric lung cancer patients. Ann Thorac Surg 2013;95:405-11.
10. Yang HC, Cho S, Jheon S. Single-incision thoracoscopic surgery for primary spontaneous pneumothorax using the SILS port compared with conventional three-port surgery. Surg Endosc 2013;27:139-45.
11. Salati M, Brunelli A, Xiumè F, et al. Uniportal videoassisted thoracic surgery for primary spontaneous pneumothorax: clinical and economic analysis in comparison to the traditional approach. Interact Cardiovasc Thorac Surg 2008;7:63-6.
12. Berlanga LA, Gigirey O. Uniportal video-assisted thoracic surgery for primary spontaneous pneumothorax using a single-incision laparoscopic surgery port: a feasible and safe procedure. Surg Endosc 2011;25:2044-7.
13. Gonzalez-Rivas D, Fieira E, Mendez L, et al. Single-port video-assisted thoracoscopic anatomic segmentectomy and right upper lobectomy. Eur J Cardiothorac Surg 2012;42:e169-71.
14. Rocco G, Martucci N, Setola S, et al. Uniportal videoassisted thoracic resection of a solitary fibrous tumor of the pleura. Ann Thorac Surg 2012;94:661-2.
15. Rocco G, Romano V, Accardo R, et al. Awake single-access (uniportal) video-assisted thoracoscopic surgery for peripheral pulmonary nodules in a complete ambulatory setting. Ann Thorac Surg 2010;89:1625-7.
16. Rocco G, La Rocca A, Martucci N, et al. Awake singleaccess (uniportal) video-assisted thoracoscopic surgery for spontaneous pneumothorax. J Thorac Cardiovasc Surg 2011;142:944-5.
17. Gigirey Castro O, Berlanga González L, Sánchez Gómez E. Single port thorascopic surgery using the SILS tool as a novel method in the surgical treatment of pneumothorax. Arch Bronconeumol 2010;46:439-41.
18. Tsai TM, Chen JS. Nonintubated thoracoscopic surgery for pulmonary lesions in both lungs. J Thorac Cardiovasc Surg 2012;144:e95-7.
19. Chou SH, Li HP, Lee JY, et al. Is prophylactic treatment of contralateral blebs in patients with primary spontaneous pneumothorax indicated? J Thorac Cardiovasc Surg 2010;139:1241-5.
20. Pompeo E, Tacconi F, Mineo D, et al. The role of awake video-assisted thoracoscopic surgery in spontaneous pneumothorax. J Thorac Cardiovasc Surg 2007;133:786-90.
21. Passlick B, Born C, Sienel W, et al. Incidence of chronic pain after minimal-invasive surgery for spontaneous pneumothorax. Eur J Cardiothorac Surg 2001;19:355-8;discussion 358-9.
22. Sihoe AD, Au SS, Cheung ML, et al. Incidence of chest wall paresthesia after video-assisted thoracic surgery for primary spontaneous pneumothorax. Eur J Cardiothorac Surg 2004;25:1054-8.
Cite this article as: Li S, Cui F, Liu J, Xu X, Shao W, Yin W, Chen H, He J. Nonintubated uniportal video-assisted thoracoscopic surgery for primary spontaneous pneumothorax. Chin J Cancer Res 2015;27(2):197-202. doi: 10.3978/ j.issn.1000-9604.2015.03.01
10.3978/j.issn.1000-9604.2015.03.01
Submitted Jan 16, 2015. Accepted for publication Mar 01, 2015.
View this article at: http://dx.doi.org/10.3978/j.issn.1000-9604.2015.03.01
杂志排行
Chinese Journal of Cancer Research的其它文章
- A case of small intestinal hemorrhage secondary to metastatic lung cancer in the elderly
- Diffusion-tensor imaging as an adjunct to dynamic contrastenhanced MRI for improved accuracy of differential diagnosis between breast ductal carcinoma in situ and invasive breast carcinoma
- Activity estimation in radioimmunotherapy using magnetic nanoparticles
- Nab-paclitaxel (abraxane)-based chemotherapy to treat elderly patients with advanced non-small-cell lung cancer: a single center, randomized and open-label clinical trial
- Activation of Toll-like receptors signaling in non-small cell lung cancer cell line induced by tumor-associated macrophages
- Feasibility of cetuximab and chemoradiotherapy combination in Chinese patients with unresectable stage III non-small cell lung cancer: a preliminary report