锚定法在单开门椎管扩大成形术治疗颈椎管狭窄症中的应用
2015-10-21聂邦旭周曙光段洪胡军胡志军袁晓峰蔡云华张云峰
聂邦旭 周曙光 段洪 胡军 胡志军 袁晓峰 蔡云华 张云峰
摘要:目的:探讨锚定钉在颈椎单开门椎管扩大术(expansive open door laminoplasty,ELAP)治疗多节段脊髓型颈椎病中的临床应用价值。方法:2007年1月~2013年3月,采用颈椎单开门椎管扩大术治疗多节段脊髓型颈椎病39例,男17例,女22例。年龄48~78岁,平均62.4岁。病程1.6~6年,平均2.8年。4节段24例,5节段15例。24例合并发育性或退变性颈椎管狭窄,均有颈脊髓受压症状,JOA评分3~11分,平均7.1±2.1分。均行颈椎單开门椎管扩大术,开门节段均为C3~C7,均采用锚定钉固定,固定节段为C3-7。结果:锚定钉均顺利置入,手术时间60~90min,平均70min。3例术后有颈肩部疼痛,给予对症处理1个月后疼痛消失。术后随访9月-30月,平均23月,末次随访时JOA评分10~16分,平均13.1±1.5分,与术前比较差异有统计学意义(P<0.01),平均改善率为(69.5±5.5)%,优良率为89.7%。X线片检查显示颈椎曲度基本正常,椎管中矢状径与椎体中矢状径比值平均为1.2,锚钉无松动,无颈椎不稳及关门。结论:颈椎后路单开门椎管扩大成形术治疗颈椎管狭窄合并脊髓型颈椎病是一种有效、简单可靠的方法,可避免“关门”,临床疗效满意,且费用也较少。
关键词:颈椎管狭窄症;单开门;椎管扩大术;锚定钉
Abstract:Objective:To investigate the clinical application value of anchoring nails in open door expansive laminoplasty treating the cervical spondylotic myelopathy.Method:From January 2007 to March 2013,39 patients with cervical spondylotic myelopathy received operations of the cervical open door expansive laminoplasty.Among them,there were 17 male patients and 22 female patients.Their ages ranged from 48 to 78 years with a mean age of 62.4 years.The course of disease ranged from 1.6 to 6 years and a mean was 2.8 years.4 segments were involved in 24 patients,5 segments in 15 patients and 20 patients combined with developmental or degenerative cervical spinal stenosis.All patients had clinical symptom of cervical cord compression.The JOA scores were 3-11 points and a mean was 7.1±2.1 points before the operation.All of them received operations of cervical expansive laminoplasty,the segments were from C3 to C7,and C3-C7 segments were anchorred with the anchoring nails.Result:During the operation,all nails were smoothly placed,The mean operative time was 70min and ranged from 60min to 90min.There was 3 patients having neck and shoulder pain after operation,and the pain disappeared with symptomatic treatment of 1 months.All patients were obtained follow-up for 9-30 months with an average of 23.5 months.The JOA scores were 10-16 points and a mean was 13.1±1.5 points at the last follow-up after operation.There were statistically significant differences compared with the results before operatin (P<0.01).The average improvement rate was (69.5±5.5)% and the rate of excellent and good results was 89.7%.Postoperative radiograph showed,the physiological curvature of cervical vertebra was basically normal,and the anchoring nails had no loosening and there was no case with cervical instability and door re-closure.Conclusion:The anchoring nail method is simple and reliable during the expansive laminoplasty treating the cervical spondylotic myelopathy.It can avoid "door reclosure",and clinical efficacy is satisfactory and expend less than others methods.
Keywords:Cervical spondylotic myelopathy;Open door ;Expansive laminoplasty;Anchoring nail
脊髓型颈椎病(cervical spondylotic myelopathy,CSM)在临床常见,诊断一旦确立,大多数学者认为应尽早手术减压治疗。可根据患者的具体情况采用不同的手术入路。经后路单开门椎管扩大术可以为脊髓提供后移空间, 使大多数病例解除脊髓壓迫。开门椎板多采用丝线缝合等方法固定,但存在关门和操作不够简便的弊病。2007年1月~2013年3月,我们在颈椎单开门椎管扩大术治疗多节段脊髓型颈椎病时应用锚定钉固定开门椎板,取得了满意疗效,报告如下。
1.一般资料
共治疗39例多节段CSM患者,男17例,女22例。年龄48~78岁,平均62.4岁。病程1.6~6年,平均2.8年。4节段24例,5节段15例。24例合并发育性或退变性颈椎管狭窄,其中11例发育性颈椎管狭窄患者颈椎管中矢状径与颈椎体中矢状径的比值平均为0.69±0.04,至少有3个节段低于0.75。临床表现为肌张力增高,肌力减退,四肢麻木、疼痛,胸腹部束带感,握力差,行走不稳,霍夫曼征阳性等。JOA评分3~11分,平均7.1±2.2分。术前均行颈椎正、侧位X 线片和MRI或(和)CT检查。
1.2手术方法 所有患者均采用全身麻醉,俯卧位。头部头低位并用垫圈预防眼球受压,作颈后正中切口,显露C2-T1棘突及两侧椎板,切断C2,3和C7,T1间棘上韧带及棘间韧带。将C3-C7棘突部分咬除,并在C3-C7棘突基部打孔。根据症状轻重,在双侧椎板与侧块交界部用尖嘴咬骨钳开槽,门轴侧保留内板并咬成“V”形槽作为门轴,开门侧咬透椎板全层。逐一掀开C7~C3椎板开门,边开边分离硬膜外粘连,开门宽约1cm以上。在C3-C7 门轴侧椎弓根处定点锚钉部位,选用18mm长,3.5mm直径的皮质骨螺钉作为锚钉,将10号丝线在皮质骨螺钉上打结系紧,一股穿过棘突根部的孔,逐一抽紧锚钉线,打结、固定,同时C3与C4的丝线相互收紧打结,C4与C5的丝线相互收紧打结,直到C6与C7的丝线相互收紧打结。查看开门固定牢靠后,用生理盐水冲洗,将切除的棘突咬碎与3克同种异体骨粒混匀后植与门轴侧,置引流管1根,逐层关闭切口。
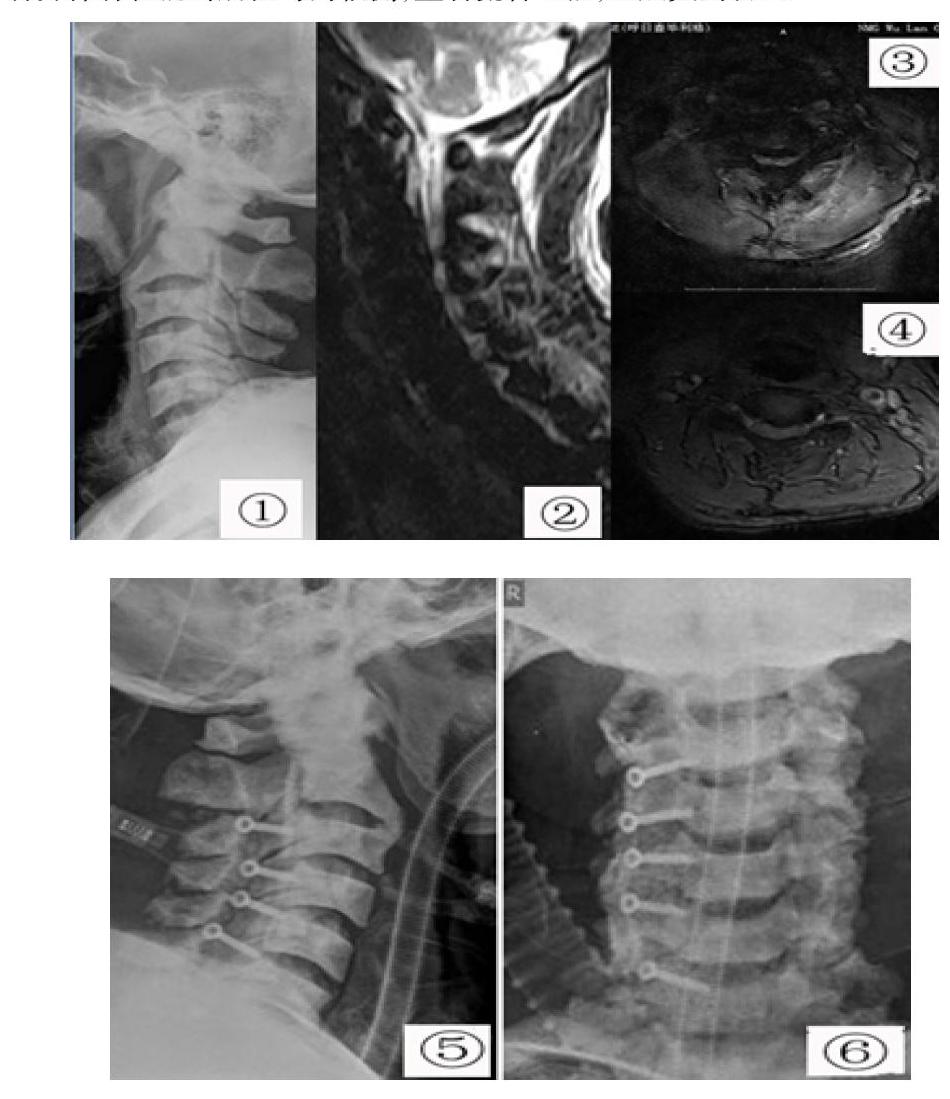
图示:患者,男,65岁,行走不稳3年,加重五月;1~4为术前X光片、MRI片所示椎管狭窄明显,图5~6所示经后路单开门减压术锚钉因定术后
1.3术后处理 术后常规应用脱水剂和搞生素3天,术后应用颈围领制动颈部6-8 周。24-48小时后拔除引流管后戴颈围下床活动,尽早开始颈后肌群的等长和等张锻炼。
1.4疗效评价标准 根据JOA评分评估患者手术后恢复的情况,术后改善率=(术后评分-术前评分)/(17-术前评分)×100,改善率≥75%为优,75%>改善率≥50%为良,50%>改善率≥25%为可,改善率<25%为差。影像学观察脊髓减压情况和有无关门等。
2结果
术后即刻多数患者即感四肢麻木感、胸腹部束带感明显减轻。术后随访9~30月,平均23.5月,临床疗效用JOA评分进行评估:术前JOA评分为6-12 分,平均为(7.1±2.1分;末次随访时JOA评分为10~16分,平均13.1±1.5分,统计学方法采用配对t检验,采用SPSS11软件进行t检验统计学分析,显示两者差异有统计学意义(P<0.01),其中优19例,良16例,可2例,差2例,优良率为89.7%。颈椎活动屈伸稍受限,术后有3例出现肩部疼痛或麻木,给予对症营养神经等处理,术后一月症状消失或明显减轻。术后X 线检查显示颈椎曲度基本正常。随访期间锚定钉无松动,无颈椎后凸畸形、颈椎不稳及关门等,脊髓减压彻底(如图所示)。
3讨论
颈椎管狭窄时对脊髓的压迫可导致不同程度的颈椎病发生。此时脊髓在椎管内已无可缓冲空间,轻微的外伤可导致脊髓损伤[1]。保守治疗一般无效,惟一有效方法是对脊髓进行有效地减压。
椎管扩大成形术的优点在于减压的同时不破坏椎体后柱结构,可预防硬膜外组织瘢痕形成对脊髓的再压迫,降低术后颈椎不稳、颈部疼痛不适等的发生率[2]颈椎椎板成形术于20世纪70年代作为椎板切除术的一种替代方式得到发展,被普遍用于治疗发育性颈椎管狭窄、颈椎后纵韧带骨化、多节段颈椎间盘突出等因素引起的颈椎管狭窄症[3,4]。
单开门颈椎管扩大成形的维持单开门颈椎管扩大成形术的远期疗效取决于如何维持椎板在开门位置,防止掀起的椎板“再关门”引起颈椎管再狭窄。最早的单开门颈椎管扩大成形是用缝线固定是把缝线固定在棘突和周围,由于颈部活动、椎旁肌收缩,可使掀起的椎板还能出现再关门, 同时缝合于软组织及关节囊上后,对局部刺激引起的轴性症状发生率较高。孙宇等[5] 认为后路悬吊使颈神经后支受到刺激或损伤,甚至将神经和其他组织缝扎在一起,导致肌肉痉挛或疼痛。或侧块螺钉之间,其固定强度较弱,难以对抗颈部外力,所以术后容易出现椎板“再关门”现象[6]。为解决这一问题,国内外学者不断尝试,提出单开门颈椎管成形术的改良术式,目前的改良ELAP 多借助FASTIN 锚钉系统、衬垫置入和ARCH钛板等内固定器械,因其价格昂贵以及操作复杂而较难在基层医院广泛应用。而用皮质骨螺钉植入椎弓根作为锚钉,用丝线将棘突与螺钉系紧起支撑作用,为真正的椎管扩大,同时避免了缝线的牵拉或刺激,也不存在缝扎小神经支,对小关节囊和周围神经的刺激降低到较低的程度,可早期功能锻炼,减少轴性症状的发生。说明椎弓根皮质骨用螺钉用为锚钉,用丝线将棘突与螺钉系紧起支撑减少轴性症状方面有优势;并且能有效避免因椎旁肌的弹性归位而造成关门;避免瘢痕组织回缩进入椎管的可能。且在材料费用方面也容易接受。随访中无再关门现象发生。
本组病例,有4例术后效果不满意,其中有两位是因其就诊时病程较晚,脊髓损伤明显,别外两例是因其颈椎前凸消失,在做单开门椎管扩大成形术后,脊髓向后漂移的空间不大,而致减压效果不明显,故CSM伴有颈椎生理曲度发生改变不是应用经后路单開门颈椎管扩大成形术的手术适应征。另3例出现肩部疼痛或麻木,颈4/5是颈椎前凸的顶点,故术后脊髓向背侧漂移,所受牵拉力量较大所致,有报导认为在经后路单开门颈椎管扩大成形术中预防性行颈4/5椎间孔扩大成形术可预防颈5 神经根损伤[7]。但是该手术危险性大技术要求高,所需时间长,故没有采用。我院在ELAP中尝试使用直皮质骨螺钉植入椎弓根作为锚钉,省了患者的住院费用,也取得了较为满意的手术效果。
颈椎后路单开门联合皮质骨螺钉植入椎弓根作为锚钉治疗颈椎复杂性多节段椎管狭窄症疗效较好,但仍存在较多问题,本院随访病例有限。
参考文献:
1.Do SY,Sang BL,Pil WH,et al.Spinal cord injury in cervical spinal st enosis by minor trauma[ J ]. World Neurosurgery,2010,73( 1):50-2.
2.Michael PS,Daniel KR.Cervicallam inoplasty [J]. The Spine Journal,2006,6( 6 S uppl):274-81.
3.Chiba K,Ogawa Y,Ishii K,et al.Long term results of expansive open door laminoplasty for cervical myelopathy:average 14 year follow up study [J].Spine,2006,31(26):2998-3005.
4.Ogawa Y,Toyama Y,Chiba K,et al.Long term results of expansive open door laminoplasty for ossification of the posterior longitudinal ligament of the cervical spine[J].J Neurosurg Spine,2004,1,(2):168-74.
5.孙宇,张风山,潘胜发,等.锚定法改良单开门椎管成形术及临床应用[ J ]。 中国脊髓脊柱杂志,2004,14(9):517-519。
6.Lee JY,Hanks SE,Oxner W,et al.Use of small suture anchors in cervical laminoplasty to maintain canal expansion:a technical note[J].J Spinal DisordTech,2007,20(1):33-35
