The relationship between ischemic stroke and weather conditions in Duzce, Turkey
2015-02-08
1Department of Emergency Medicine, Duzce University School of Medicine, Duzce, Turkey
2Department of Neurology, Duzce University School of Medicine, Duzce, Turkey
3Department of Radiology, Duzce University School of Medicine, Duzce, Turkey
Corresponding Author:Harun Gunes, Email: haroonsun@hotmail.com
The relationship between ischemic stroke and weather conditions in Duzce, Turkey
Harun Gunes1, Hayati Kandis1, Ayhan Saritas1, Suber Dikici2, Ramazan Buyukkaya3
1Department of Emergency Medicine, Duzce University School of Medicine, Duzce, Turkey
2Department of Neurology, Duzce University School of Medicine, Duzce, Turkey
3Department of Radiology, Duzce University School of Medicine, Duzce, Turkey
Corresponding Author:Harun Gunes, Email: haroonsun@hotmail.com
BACKGROUND:Weather conditions are thought to increase the risk of stroke occurrence. But their mechanism has not yet been clarifi ed. We investigated possible relationships between ischemic stroke and weather conditions including atmospheric pressure, temperature, relative humidity, and wind speed.
METHODS:One hundred and twenty-eight patients with ischemic stroke who had been admitted to our hospital between January 1 and December 31, 2010 were enrolled in this study. We investigated the relationship between daily cases and weather conditions the same day or 1, 2, and 3 days before stroke.
RESULTS:A negative correlation was found between maximum wind speed and daily cases 3 days before stroke. As the relationship between daily cases and changes of weather conditions in consecutive days was evaluated, a negative correlation was found between daily cases and change of atmospheric pressure in the last 24 hours.
CONCLUSIONS:The maximum wind speed 3 days before stroke and change of atmospheric pressure in the last 24 hours were found to increase the cases of ischemic stroke. We recommend that individuals at risk of ischemic stroke should pay more attention to preventive measures, especially on days with low maximum wind speed, on subsequent 3 days, and on days with low atmospheric pressure in the last 24 hours.
Weather conditions; Ischemic stroke; Turkey
INTRODUCTION
It has been reported that weather conditions may increase the risk of stroke occurrence.[1]Well-known risk factors of ischemic stroke (IS) such as age, gender, genetic factors, and diseases like hypertension, diabetes mellitus, and heart disease cannot change day-by-day, thus weather conditions are thought to be the causative factors triggering stroke events.[2]
Weather conditions cause some physiologic changes. For example, blood pressure, erythrocyte and thrombocyte counts, and blood viscosity are increased in cold weather.[3]Plasma fibrinogen concentration is higher in older patients especially in cold weather.[4]An increase of body temperature is associated with increased levels of coagulation factors.[5]The existing theory suggests that changes in atmospheric pressure may exert stress on atherosclerotic plaque, resulting in rupture of the plaque.[6]
This study was conducted because there are four seasons and different weather conditions every year in Turkey. We evaluated the possible relationships between IS occurrence and weather conditions such as atmospheric pressure, weather temperature, relative humidity, and wind speed.
METHODS
The patients in our study retrieved the computerizedarchival system of our hospital. Name, gender, file number, complaints on admission, history of complaints, medical history, results of physical examination, results of laboratory tests, and results of imagings including computed tomography (CT) and magnetic resonance imaging (MRI), treatments, in-hospital and out-patient follow-up, and diagnoses of patients were reviewed. Print versions of the fi les of the patients in our hospital’s archive were also reviewed.
A total of 321 patients with cerebrovascular disease (International Classification of Diseases 10 diagnosis codes: G46, G46.8, I63.9, I66.3, I67, I67.8, I67.9, I69, I69.8) were retrieved using the computerized archival system in our hospital between January 1 and December 31, 2010. We reviewed both computerized records and archival fi les of the 321 patients retrospectively. Patients who were diagnosed with cerebrovascular disease due to hemorrhagic stroke, transient ischemic attack or stroke history, and those who were diagnosed with IS because of changes of consciousness on admission induced by hypoglycemia, septic shock, and intoxication were excluded. At last, 132 patients with IS were found. They were subjected to CT and/or MRI, and reports were written by a radiologist. Symptom onset time for each patient was taken from fi les of the patients. Four patients were excluded from the study because the exact time of their symptom onset was not known. The remaining 128 patients were found to meet the inclusion criteria for IS. Daily cases were determined on the day when patients started to complain.
Patient age, sex, hospitalization period, systolic blood pressure, diastolic blood pressure, mean arterial blood pressure, pulse rate, white blood cell count, hemoglobin, hematocrit, platelet count, serum glucose, urea, creatinine, Na+, K+, and Cl–values were obtained using the computerized archival system.
The maximum, minimum, and mean values of daily atmospheric pressure, weather temperature, and relative humidity, and daily maximum wind speed in Duzce between January 1 and December 31, 2010 were obtained from the Turkish State Meteorological Service.
The relationship was determined between daily cases and the following conditions: (1) daily weather conditions of the days in which patients began to complain; (2) weather conditions of 1, 2, and 3 days before the day in which patients began to complain; (3) changes in weather conditions in a day up to 3 days before the day in which patients began to complain; (4) changes in weather conditions in consecutive days up to 72 hours before the day in which patients began to complain.
The data of this study are shown in Tables 1–3. Oneway variance analysis (ANOVA) was used to determine the relationship between daily cases and daily weather conditions. Sidac and LSD tests were used in posthoc analysis by which a significant relationship was found with ANOVA analysis. SPSS version 18.0 for Windows was used for statistical analysis, and P<0.05 was considered statistically significant. This study was approved by the local ethics committee.
RESULTS
Fifty-nine (46.1%) of our patients were male, and their mean age was 72±10 years. Descriptive features of our patients are shown in Table 1. No significant relationship was found between daily cases and mean atmospheric pressure, air temperature, relative humidity and maximum wind speed in the same day (P=0.441; P=0.942; P=0.615; P=0.617, respectively).
There was a relationship between daily case numbers and weather conditions of the day and 1, 2, and 3 days before the event. But a signifi cant relationship was found between daily case numbers and maximum wind speed 3 days ago (P=0.048). Post-hoc analysis with LSD test revealed that if the maximum wind speed 3 days ago was low, the risk of IS increased markedly (P=0.015) (Table 2) (Figure 1).
No significant relationship was found between daily cases and change of weather conditions in a day (P>0.05). While evaluating the relationship between daily cases and change of weather conditions in consecutive days, we found a significant relationship between case numbers and change of atmospheric pressure in the last 24 hours (P=0.019). Post-hoc analysis using Sidak test showed that change of lower pressure in the last 24 hours increased the possibility of IS occurrence (P=0.048) (Table 3, Figure 2).
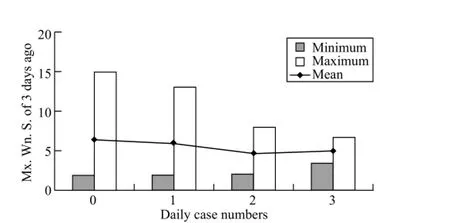
Figure 1. Maximum wind speed (Mx. Wn. S.) 3 days before the occurrence of stroke. LSD test in post-hoc analysis revealed a signifi cant difference between days with no patient and days with 2 patients (P=0.015).
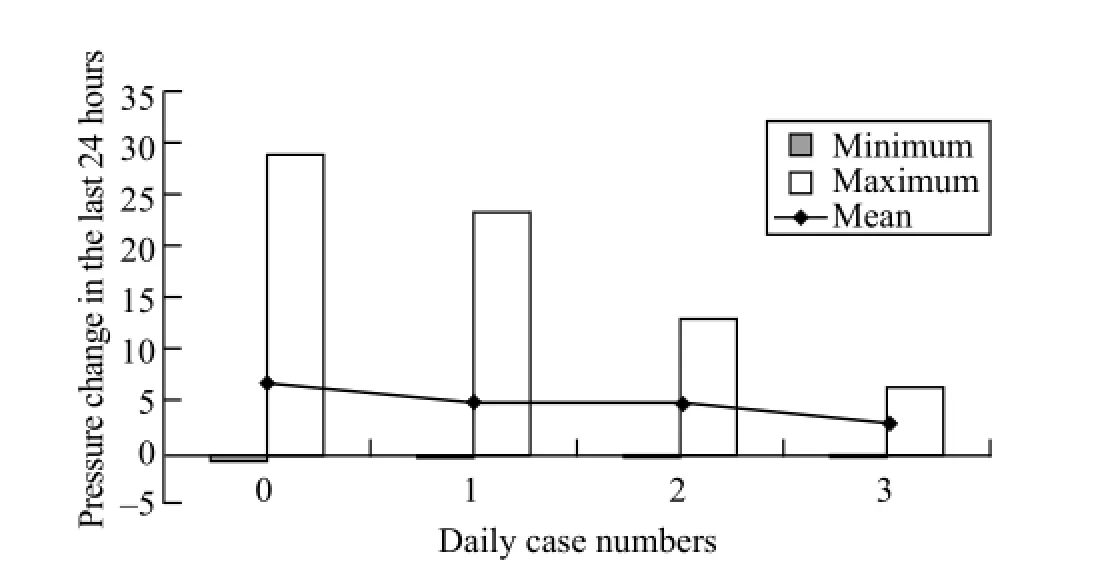
Figure 2. Minimum, maximum and mean values of atmospheric pressure in the last 24 hours for days with no patients (0) and with 1, 2, and 3 patients. A signifi cant difference was found between pressure change in days with no patients (0) and days with 1 patient (1) in posthoc analysis with Sidak test (P=0.048). Actually, a more prominent difference was observed between change of atmospheric pressure in the last 24 hours in days with no patient (0) and in days with 3 patients, but this difference was not statistically significant because the number of days with 3 patients was small (only 5 days).

Table 1. Demographic characteristics, hospital stay, blood pressure, complete blood count, and biochemical parameters of the patients
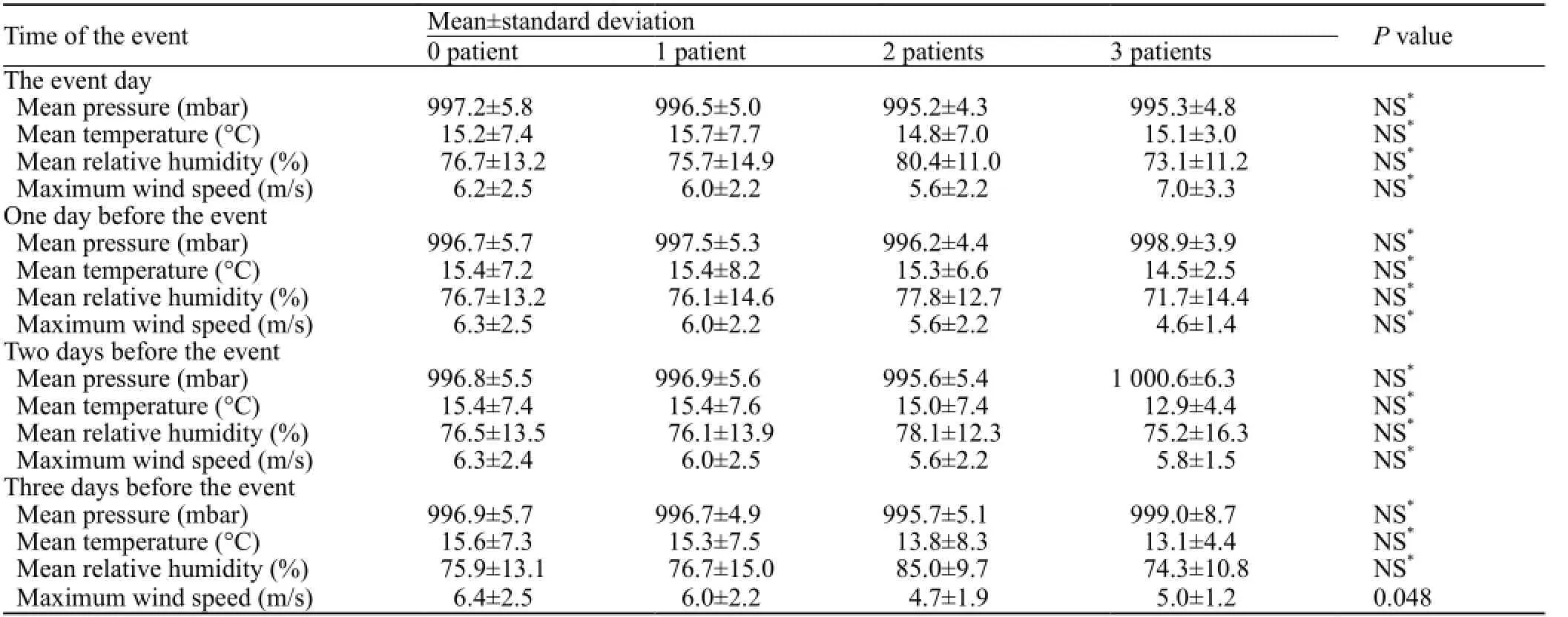
Table 2. The relationship between daily weather conditions and daily cases
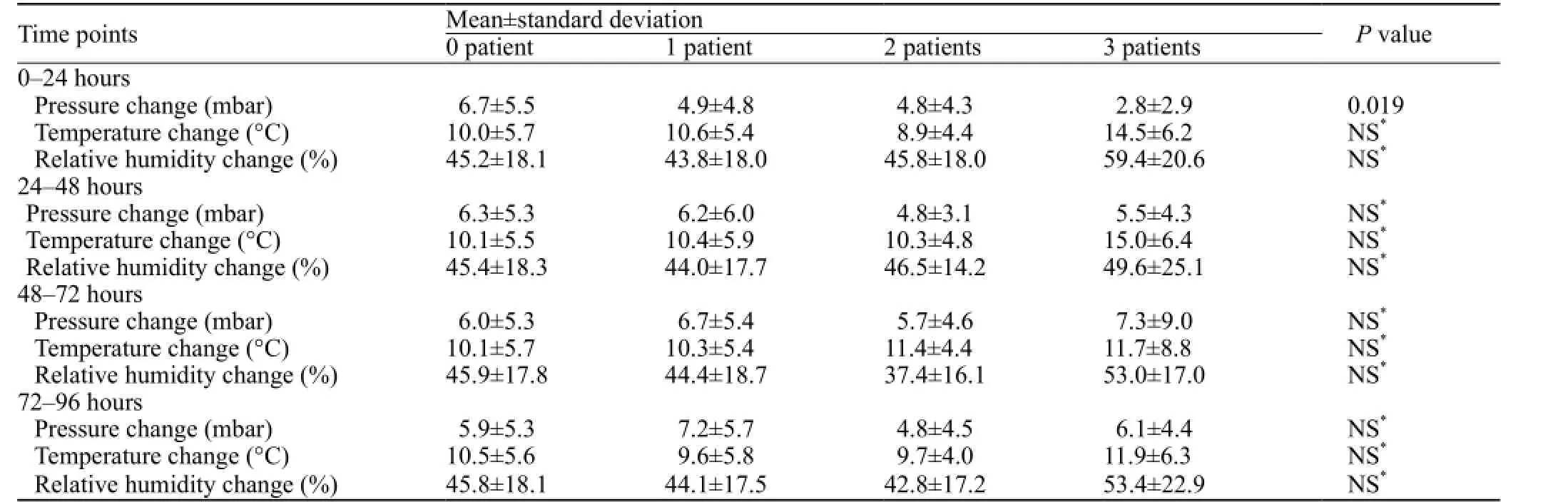
Table 3. The relationship between daily cases and change of atmospheric pressure in consecutive days
DISCUSSION
The possible relationship between weather conditions and IS occurrence has not yet been clarified. We found that IS cases increase daily when the maximum speed of wind is low 3 days before stroke or change of atmospheric pressure in the last 24 hours.
No significant relationships were observed between daily cases and weather conditions.[7–10]But some studies found such relationship.[2,11–14]
Possible relationships were noted between daily cases, daily mean temperature, and atmospheric pressure;[7]between daily temperature, air pressure, and relative humidity;[8]between daily mean temperature, air pressure, mean wind speed, maximum wind speed, relative humidity, and Chinook winds;[9]and between daily weather conditions[10]in different countries. However, there was no statistically signifi cant relationship.
Cases of stroke were seen predominantly in hot days.[2]Emergency transports coded as stroke decreased when temperature or relative humidity increased.[11]But the findings may be misleading because the cases were transported with ambulance and coded as stroke. However they were not definitely diagnosed until imaging studies were performed at the hospital. Feigin et al[12]found that low temperature and mean atmospheric pressure increased the risk of IS; but the study was conducted in the Siberia region of Russia where weather is cold, suggesting that the results may not reflect the true relationship between weather conditions and IS. Iwamoto et al[13]also found that IS occurs frequently in the elderly in hot days. They studied only five elderly cases which make us to think about whether generalization of the results is proper or not.
We did not fi nd any relationship between daily cases and weather conditions of the same day, which supports the conclusion that the effect of weather conditions is not seen in the same day. One study[14]reported a significant relationship between number of cases and weather conditions in previous days, and the other[7]found no signifi cant relationship. Hong et al[15]found that low temperature increased the risk of IS, and the most powerful effect was seen after exposure to cold weather.
Cowperthwaite and Burnett[7]found no significant relationship between daily cases and daily temperature, pressure and humidity 1, 2, 3, 5, and 7 days before stroke. We also did not fi nd any relationship between daily cases and mean temperature, pressure and humidity 1, 2, and 3 days before stroke. These studies[15,7]did not evaluate possible effects of wind speed, but we found that daily cases increased if maximum wind speed was low 3 days before stroke. Nonetheless, we are unable to explain how the lower wind speed may trigger IS 3 days later.
IS may be related not only to weather conditions but to changes of weather conditions. Studies[6,7,14,16]found that there was no relationship between daily cases and changes of weather conditions, and others[10,17–20]reported relationships between daily cases and changes of weather conditions.
In many countries, no relationship was found between changes of atmospheric pressure and stroke;[6]between daily cases and changes of atmospheric pressure, temperature, and relative humidity;[7]between changes of weather temperature and number of IS cases;[14]and between mean daily temperature and IS cases[16]each month. Studies[6,7]investigated possible relationships between stroke and changes of weather conditions in a single day. In our study there was a signifi cant relationship between daily cases and changes of atmospheric pressure in the last 24 hours.
Jimenez-Conde et al[10]found a significant relationship between non-lacunar ISs and a decrease in atmospheric pressure compared to previous days. But in our study, the risk of IS increased if change of atmospheric pressure in the last 24 hours was moderate; this fi nding is opposite to that of Jimenez-Conde et al.[10]It is possible that human body may need a daily atmospheric pressure cycle as it needs a light cycle and plays a role in pathophysiology of IS. Thus, IS may be triggered when the change of daily atmospheric pressure is not great. A strong relationship was observed between IS and decrease of air temperature.[17]Gomes et al[18]found a relationship between stroke incidence and a decline in minimum temperature ≥3 °C in 2 of consecutive 10 days. In another study Gomes et al[19]found that a decline of minimum temperature >2.4 °C in any 2 consecutive days in a week and stroke incidence are significantly correlated. These two studies were performed in Maputo, Mozambique where daily temperature varies between 14 °C and 30 °C throughout the year.[18]The temperature in Maputo may affect the results of these studies. Additionally, cases of stroke, hemorrhagic and ischemic, were included in the studies, but cases of ischemic and hemorrhagic stroke are significantly different in clinical entities and pathophysiology. The increased number of stroke cases after a decrease of air temperature may be due to increased cases of hemorrhagic stroke. Mostofsky et al[20]reported a higher risk of IS in hours and days after a moderate decrease of temperature. As mentioned above, we did not fi nd such relationship between decrease of air temperature and stroke occurrence. Because the small number of cases and the short study period, the possible relationship between IS and changes of weather conditions may be not statistically signifi cant.
No studies have shown a relationship between daily cases and maximum wind speed 3 days before the event. Our study showed that IS cases increased as the atmospheric pressure was low in the last 24 hours. But the mechanism that IS may be triggered by the two factors is not clear.
Our study has also limitations. First, the study was performed in one city, so the results may be identical to areas with similar weather conditions. Second, it was a retrospective study with the data of only one year, thus the number of cases are limited. Some possible relationships may be overlooked. Third, three IS cases were admitted to the hospital within 5 days. Finally, the data of our study were only from one center. We tried to decrease the impact of the limitations by screening patients to include patients with an exact diagnosis of ischemic stroke. We investigated the final diagnosis of patients while re-evaluating their imaging studies.
In conclusion, we found two factors that related to the occurrence of IS. First, the low maximum wind speed increased the number of IS cases after 3 days. Second, the number of cases increased when the change of atmospheric pressure was minimal in the last 24 hours. Hence, if patients are at risk clinicians should take preventive measures against IS in these periods.The two factors may play a role in stroke occurrence, and we suggest that long-term studies with a large number of cases are needed to confirm our findings and determine the role of the two factors in the pathophysiology of IS.
Funding:None.
Ethical approval:This study was approved by the ethics committee of the university.
Confl icts of interest:Authors have no commercial associations or sources of support that might pose a confl ict of interest.
Contributors:Gunes H proposed the study. All authors contributed to the design and interpretation of the study, and approved the fi nal manuscript.
1 Petrov D, Hidalgo A, Gandhi C, Prestigiacomo C. Decreases in temperature and relative humidity leading to an increased incidence of ischemic stroke. J NeuroIntervent Surg 2011; 3: A4.
2 Berginer VM, Goldsmith J, Batz U, Vardi H, Shapiro Y. Clustering of strokes in association with meteorologic factors in the Negev Desert of Israel: 1981–1983. Stroke 1989; 20: 65–69.
3 Keatinge WR, Coleshaw SRK, Cotter F, Mattock M, Murphy M, Chelliah R. Increases in platelet and red cell counts, blood viscosity, and arterial pressure during mild surface cooling: Factors in mortality from coronary and cerebral thrombosis in winter. Br Med J (Clin Res Ed) 1984; 24; 289: 1405–1408.
4 Woodhouse PR, Khaw KT, Plummer M, Foley A, Meade TW. Seasonal variation of plasma fibrinogen and factor VII activity in the elderly: winter infections and death from cardiovascular disease. Lancet 1994; 343: 435–439.
5 Schafer AI. The hypercoagulable states. Ann Intern Med 1985; 102: 814–828.
6 Houck PD, Lehten JE, Riggs MW, Gantt DS, Dehmer GJ. Relation of atmospheric pressure changes and the occurrences of acute myocardial infarction and stroke. Am J Cardiol 2005; 96: 45–51.
7 Cowperthwaite MC, Burnett MG. An analysis of admissions from 155 United States hospitals to determine the influence of weather on stroke incidence. J Clin Neurosci 2011; 18: 618–623.
8 Chen ZY, Chang SF, Su CL. Weather and stroke in a subtropical area: Ilan, Taiwan. Stroke 1995; 26: 569–572.
9 Field TS, Hill MD. Weather, Chinook, and stroke occurrence. Stroke 2002; 33: 1751–1757.
10 Jimenez-Conde J, Ois A, Gomis M, Rodriguez-Campello A, Cuadrado-Godia E, Subirana I, et al. Weather as a trigger of stroke. Daily meteorological factors and incidence of stroke subtypes. Cerebrovasc Dis 2008; 26: 348–354.
11 Ohshige K, Hori Y, Tochikubo O, Sugiyama M. Influence of weather on emergency transport events coded as stroke: population-based study in Japan. Int J Biometeorol 2006; 50: 305–311.
12 Feigin VL, Nikitin YP, Bots ML, Vinogradova TE, Grobbee DE. Population-based study of the associations of stroke occurrence with weather parameters in Siberia, Russia (1982–92). Eur J Neurol 2000; 7: 171–178.
13 Iwamoto T, Akazawa M, Ami M, Shimizu T, Umahara T, Takasaki M. Five elderly patients with cerebral infarction seen during a heat wave. Nihon Ronen Igakkai Zasshi 1999; 36: 565–571.
14 Low RB, Bielory L, Qureshi AI, Dunn V, Stuhlmiller DFE, Dickey DA. The relation of stroke admissions to recent weather, airborne allergens, air pollution, seasons, upper respiratory infections, and asthma incidence, September 11, 2001, and day of the week. Stroke 2006; 37: 951–957.
15 Hong YC, Rha JH, Lee JT, Ha EH, Kwon HJ, Kim H. Ischemic stroke associated with decrease in temperature. Epidemiology 2003; 14: 473–478.
16 Shinkawa A, Ueda K, Hasuo Y, Kiyohara Y, Fujishima M. Seasonal variation in stroke incidence in Hisayama, Japan. Stroke 1990; 21: 1262–1267.
17 Rufca GF, Zaffani E, Zerbini R, Gaia FF, Oliveira Fde N, Tognolla WA. Infl uence of circadian and temperature variations on the ischemic stroke. Rev Assoc Med Bras 2009; 55: 60–63.
18 Gomes J, Damasceno A, Carrilho C, Lobo V, Lopes H, Madede T, et al. The effect of season and temperature variation on hospital admissions for incident stroke events in Maputo, Mozambique. J Stroke Cerebrovasc Dis 2014; 23: 271–277.
19 Gomes J, Damasceno A, Carrilho C, Lobo V, Lopes H, Madede T, et al. Triggering of stroke by ambient temperature variation: A case-crossover study in maputo, mozambique. Clin Neurol Neurosurg 2015; 129: 72–77.
20 Mostofsky E, Wilker EH, Schwartz J, Zanobetti A, Gold DR, Wellenius GA, et al. Short-Term Changes in Ambient Temperature and Risk of Ischemic Stroke. Cerebrovasc Dis Extra 2014; 4: 9–18.
Received December 18, 2014
Accepted after revision April 6, 2015
10.5847/wjem.j.1920–8642.2015.03.008
World J Emerg Med 2015;6(3):207–211
杂志排行

World journal of emergency medicine的其它文章
- Albuterol in the treatment of acute respiratory distress syndrome: A meta-analysis of randomized controlled trials
- Effi cacy and safety of glucocorticoids in the treatment of community-acquired pneumonia: A meta-analysis of randomized controlled trials
- Performance of cardiopulmonary resuscitation during prolonged basic life support in military medical university students: A manikin study
- Peer-assisted learning to train high-school students to perform basic life-support
- Feasibility study of fi rst-year medical students identifying cardiac anatomy using ultrasound in rural Panama
- Sequential invasive-noninvasive mechanical ventilation weaning strategy for patients after tracheostomy