A cross sectional study on antibiotic resistance pattern of Salmonella typhi clinical isolates from Bangladesh
2014-03-23AdnanMannanMohammadShohelSultanaRajiaNiazUddinMahmudSanjanaKabirImtiajHasan
Adnan Mannan, Mohammad Shohel, Sultana Rajia, Niaz Uddin Mahmud, Sanjana Kabir, Imtiaj Hasan
1Department of Genetic Engineering and Biotechnology, Faculty of Biological Sciences, University of Chittagong, Chittagong-4331, Bangladesh
2Department of Pharmacy, North South University, Dhaka, Bangladesh
3Department of Pharmacy, Varendra University, Rajshahi-6204, Bangladesh
4Department of Computer Science & Engineering, BGC Trust University Bangladesh, Chittagong, Bangladesh
5Department of Biochemistry and Molecular Biology, Rajshahi University, Rajshahi-6205, Bangladesh
6Laboratory of Glycobiology and Marine Biochemistry, Department of Life and Environmental System Science, Graduate School of Nano Biosciences, Yokohama City University, Yokohama-236-0027, Japan
A cross sectional study on antibiotic resistance pattern of Salmonella typhi clinical isolates from Bangladesh
Adnan Mannan1*, Mohammad Shohel2, Sultana Rajia3, Niaz Uddin Mahmud4, Sanjana Kabir2, Imtiaj Hasan5,6
1Department of Genetic Engineering and Biotechnology, Faculty of Biological Sciences, University of Chittagong, Chittagong-4331, Bangladesh
2Department of Pharmacy, North South University, Dhaka, Bangladesh
3Department of Pharmacy, Varendra University, Rajshahi-6204, Bangladesh
4Department of Computer Science & Engineering, BGC Trust University Bangladesh, Chittagong, Bangladesh
5Department of Biochemistry and Molecular Biology, Rajshahi University, Rajshahi-6205, Bangladesh
6Laboratory of Glycobiology and Marine Biochemistry, Department of Life and Environmental System Science, Graduate School of Nano Biosciences, Yokohama City University, Yokohama-236-0027, Japan
PEER REVIEW
Peer reviewer
Mohammad Arif Rahman, Research Fellow, Centre for AIDS Research, Kumamoto University, Japan.
Tel: +8180-4278-5892
E-mail: 111r5174@st.kumamoto-u.ac.jp
Comments
This is an interesting research work in which authors have demonstrated antibiotic resistance pattern of S. typhi clinical isolates in a highly populated developing country. The authos have showed that there is no relation between population density and evolving of resistant strains. Moreover, the authors have showed the overall resistant pattern of Salmonella typhi in population level, this information can be important for clinicians to provide treatment.
Details on Page 310
Objective:To investigate and compare the resistance and sensitivity of Salmonella typhi samples to commonly used antibiotics in three major divisions of Bangladesh and to evaluate the gradually developing resistance pattern.
Bangladesh, Salmonella typhi, Resistance, Susceptibility, Antibiotic
1. Introduction
Typhoid fever is an epidemic problem for Bangladesh, Indian subcontinent, South and Central America and Africa. Despite the use of newly developed antibacterial drugs, enteric fevers such as typhoid and paratyphoid caused by multidrug-resistant bacterial strains are one of major health problems in Bangladesh, especially for the children[1]. This disease is the most prevalent in South Central Asia and Southeast Asia with more than 100 cases per 100 000 persons per year. Regions of medium incidence (10-100 cases per 100 000 persons per year) include the rest of Asia, LatinAmerica, Africa and the Caribbean, and Oceania, except for Australia and New Zealand. It is estimated that there are 22 million new cases of enteric fever annually, with 200 000 deaths[2].
In early 1970s, emergence of plasmid-mediated chloramphenicol resistance was reported and the effectiveness of chloramphenicol as a first-line drug decreased gradually by outbreaks caused by resistant strains in countries as far apart as Mexico and India. Outbreaks occurred in Vietnam, Indonesia, Korea, Chile and Bangladesh in the next five years[3].Salmonella typhi(S. typhi) is now rapidly developing resistance to cipropfloxacin and fluoroquinolone along with other conventional antibiotics as reported in different parts of the world and emerged as new challenges to the treatment of typhoid fever[4-12].
It was reported that, in Bangladesh third generation cephalosporins (ceftriaxone and cefixime) are still the effective drugs for treating typhoid fever if used in proper dose and duration. Though azithromycin is prescribed as an alternative to ciprofloxacin in resistant cases, recently it has lost the credibility due to the emergence of resistance[1,13]. According to records of the public and private hospitals, enteric fever is a major infectious disease occurring at high fluctuating incidences all over Bangladesh.
Resistance to antibiotics is mainly driven by the selective pressure imposed by their inappropriate use. Especially in developing countries like Bangladesh, people do not have the minimal awareness of resistance, antibiotics and infections. They want symptomatic relief to which the health professionals respond by prescribing antibiotics for quick recovery. Infections with drug-resistant microorganisms are associated with severity of the patient’s illness, increased patient contact with healthcare personnel and length of stay in the hospital. Eventually it causes extra cost of health care, extended stay in the hospital, sudden or prolonged health complications including significant excess morbidity and mortality[14,15]. Sometimes it reaches an extreme level through the cross-infection of hospitalized patients with such drug-resistant organisms[16].
So it became inevitable to check and compare the current status of the susceptibility and resistance patterns ofS. typhiin a country to find any regional difference. Moreover, determining the responsible compounds for antibiotic resistance by observing the correlation betweenS. typhiand some biochemical parameters may become beneficial for both the drug designers as well as the manufacturers.
This is the first comparative study reporting the assessment of antimicrobial susceptibility and resistance ofS. typhifor two other big divisions (Rajshahi and Chittagong) of Bangladesh in addition to Dhaka that will provide ideas about the regional variations of this pattern, if any.
These observations with variations in the sensitivity and resistance patterns forS. typhiagainst particular antibiotics will provide suitable guidelines for clinicians to prescribe specific antibiotics for typhoid fevers in specific cases for the patients of Bangladesh. This information can become useful for some other tropical countries in Southeast Asia to face similar health problems.
2. Materials and methods
2.1. Sample collection
Blood, sputum, urine and pus samples were collected from 945 patients at different hospital and diagnostic centers in Dhaka, Chittagong and Rajshahi during November 2011 to November 2012. The patients were categorized in five age groups, <10, 10-20, 20-30, 30-40 and >40 years. Patients with systemic infection were selected for this study and their clinical history and examination findings were recorded on the standard form before preceding the blood culture.
2.2. Isolation of colonies
The aseptically collected samples were inoculated on nutrient agar media using a calibrated loop delivering 10 μL of the sample and incubated overnight at 37 °C. All bacterial specimens were cultured on blood agar and MacConkey agar, again incubated overnight at 37 °C and the isolates were identified by adopting standard microbiological procedure which includes colony morphology, Gram stain reaction and biochemical reaction such as oxidase, catalase, sulfide indole motility test, citrate agar slant, methyl red test, Voges Proskauer test, triple sugar iron agar test and urease test. The isolates ofSalmonellawere further confirmed by abblutination with polyvalen O antiserum A-S and individual H antisera (Denka Seiken, Japan).
2.3. Sensitivity test
Susceptibility and resistance of all isolates were checked by performing the Kirby-Bauer disc diffusion method according to the guidelines of Clinical and Laboratory Standards Institute, formerly National Committee for Clinical Laboratory Standards[17,18]. The antibiotic incorporated plates were incubated at 37 °C and zones of inhibition around the antibiotic were measured after 18 h and within 24 h of incubation.
The routinely used antibiotics, all from Hi Media, were chloramphenicol, azithromycin, cephalexin, ciprofloxacin, gentamicin, cloxacillin, azacitidine, cefixime, nitrofurantoin, nalidixic acid, levofloxacin and ampicillin. The isolates wereconsidered as multidrug resistant if they were resistant to at least two classes of antibiotics.
2.4. Statistical analysis
Data analysis was performed by employing Statistical Package for Social Science (SPSS version 10.0). To compare mean values between groupst-test was done as a test of significance.
3. Results
A total of 70S. typhiisolates were found from 945 clinical samples. Samples isolated from Dhaka, Chittagong and Rajshahi were evaluated for their sensitivity and resistance to antiobiotics. Twelve commonly prescribed and available antibiotics were used to assess.
Antibiogram of these isolates showed that,S. typhiwas most susceptible towards chloramphenicol in Dhaka (20.30%) and Rajshahi (16.66%) (P<0.05) whereas cefixime was found most sensitive in Chittagong (31.34%) (P<0.05). There was a significant percentage of susceptibility to ciprofloxacin in all three regions (P<0.05). Another susceptible antibiotic was levofloxacin. Sensitivity to levofloxacin was found in the samples of Dhaka (5.50%), Chittagong (17.34%) and Rajshahi (13.88%) (Figure 1).

Figure 1. Percentage of Salmonella clinical isolates susceptible to antibiotics in three divisions.Cro-Chloramphenicol, Azi-Azithromycin, Cep-Cephalexin, Cip-Ciprofloxacin, Gen-Gentamicin, Clox-Cloxacillin, Azac-Azacitidine, Cefi-Cefixime, Nit-Nitrofurantoin, Nal-Nalidixic acid, Levo-Levofloxacin, Amp-Ampicillin.
In case of resistance (Figure 2), highest resistance was observed against nalidixic acid in all three divisions. The percentage was significant (P<0.05) in Rajshahi (66.60%) and Chittagong (40.00%). Resistance to cefixime was also observed in Dhaka (11.45%), Chittagong (8.00%) and Rajshahi (16.66%). No resistance was found against chloramphenicol.
Antibiotic resistance varies depending on age (Figure 3). Rate of resistance was most among adult patients of 30-40 years. There were samples of infants and child resistant to all the antibiotics. Resistance to ciprofloxacin was also observed among all age groups.
In this study, report of multidrug resistance has been found. Significant multidrug resistance has been observed in Dhaka (79.41%) and Chittagong (60.00%). Multidrug resistance has also been found in Rajshahi but in a lower percentage than other divisions.
The overall study (Figure 4) shows that ciprofloxin (16%) is the mostly susceptible antibiotic in Bangladesh followed by chloramphenicol (15%) and cefixime (12%).

Figure 2. Percentage of Salmonella clinical isolates resistant to antibiotics in three divisions.Cro-Chloramphenicol, Azi-Azithromycin, Cep-Cephalexin, Cip-Ciprofloxacin, Gen-Gentamicin, Clox-Cloxacillin, Azac-Azacitidine, Cefi-Cefixime, Nit-Nitrofurantoin, Nal-Nalidixic acid, Levo-Levofloxacin, Amp-Ampicillin.
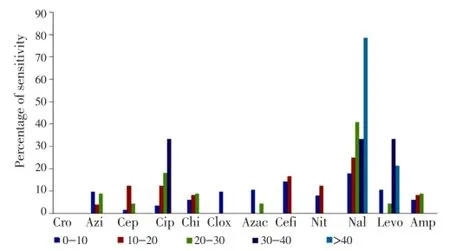
Figure 3. A comparison of the resistance of the drugs used according to age in this study in all the three divisions.Cro-Chloramphenicol, Azi-Azithromycin, Cep-Cephalexin, Cip-Ciprofloxacin, Gen-Gentamicin, Clox-Cloxacillin, Azac-Azacitidine, Cefi-Cefixime, Nit-Nitrofurantoin, Nal-Nalidixic acid, Levo-Levofloxacin, Amp-Ampicillin.

Figure 4. Pattern of percentages of antibiotic susceptibility among all isolated clinical samples of S. typhi.
On the other hand, nalidixic acid was found the mostresistant antibiotic (29%) againstS. typhi(Figure 5). Resistance against cefixime (12%) was also remarkable. Resistance against levofloxacin (9%) and ciprofloxacin (8%) was also observed in high rate.
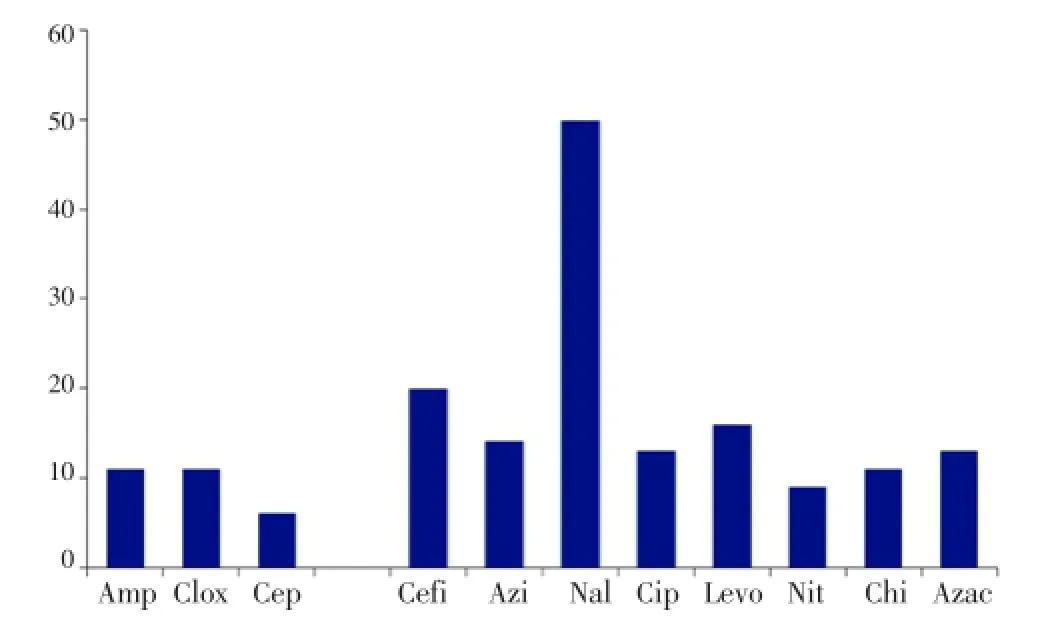
Figure 5. Pattern of percentages of antibiotic resistance among all isolated clinical samples of S. typhi.Amp-Ampicillin, Clox-Cloxacillin,Cep-Cephalexin, Cefi-Cefixime, Azi-Azithromycin, Nal-Nalidixic acid, Cip-Ciprofloxacin, Levo-Levofloxacin, Nit-Nitrofurantoin, Cro-Chloramphenicol, Gen-Gentamicin, Azac-Azacitidine.
4. Discussion
The occurrence of antibiotic resistance in lower-middleincome countries takes place due to the poor access to doctors. It eventually encourages the unacceptable practice of selling antibiotics over the country[19]. A relation between antibiotic use and its resistance in clinical isolates had been proven in many studies. Even though, a direct quantitative relationship between the amount of antibiotic used and the frequency of resistance is still lacking[20].
In the present study regional differences in antibiotic sensitivity againstS. typhiwere observed. Most isolates were resistant to nalidixic acid, ciprofloxacin, cefixime, azithromycin. In all of the three regions, nalidixic acid was found the most resistant antibiotic againstS. typhiwhereas the number of ciprofoloxacin and levofloxacin resistant strain was also higher in Chittagong region.
Although previous studies showed the growing resistance of ciprofloxacin[21-23], but we found both ciprofloxacin resistant and susceptible samples. It might be due to less resistance to ciprofloxacin in Rajshahi. Sixteen percent of the studied samples were susceptible to ciprofloxacin. On the other hand 8% of the samples were resistant to it.
Nalidixic acid was previously shown to be resistant in Dhaka[13]. Our study shows similar pattern of resistance to nalidixic acid in Chittagong and Rajshahi as well. Resistance to nalidixic acid has also been reported in India, China and Tunisia[11,12,24].
In our study we found that 64.28% isolates ofS. typhiare multidrug resistant. This shows alarming increase of multidrug resistance of this organism in Bangladesh supported by a number of previous studies[13,25-27].
Similar pattern of increase in multidrug resistance has been observed in the last 30 years in India[28]. Contributory factors may be drug overuse, misuse and inappropriate prescribing practices by physicians along with intrinsic microbiological plasmid-mediated factors[15,29].
The increase ofSalmonellastrains resistant to antibiotics may be an indicator of the ecological impact of use of antibiotics in animals[30]. A large amount of antibiotics have been used in veterinary medicine as therapy or feed additives, which producing resistant organism[31,32]. These resistant bacteria and/or their resistant genes can be transferred from animals to humans through the food chain[30,33]. Tetracycline and cephalosporin have been used in prevention and control of bacterial infection as veterinary medicine and in plant agriculture, other than in human[34]. Though Bangladesh is a land of cultivation, no isolates were found resistant to chloramphenicol in Dhaka, Rajshahi and Chittagong region whereas cefixime resistant strains were found in three of the regions.
Moreover, increased population can lead to increased dissemination of antibiotic resistant bacteria and resistant genes[35]. As Bangladesh is a developing country, increase in population density and urbanization may facilitate the spread of resistant bacteria and gene, which was also seen in other countries[36].
Our research shows that, antibiotic resistance is common among children. It might be due to use of antibiotic for other indications. Antibiotic resistance was also observed among the children of Europe, and the reason was misuse of antibiotic[37]. Continuous use of antibiotic in Bangladesh can be a reason for high occurrence of resistance among the adults in this study. Inconclusive diagnosis, over dependence on antibiotics can be causes for this[4].
According to our findings, ciprofloxacin and nalidixic acid cannot be a potential option for the treatment due to their resistance. Pattern of resistance varies due to geographical and environmental variance. Physicians should be more conscious in prescribing similar antibiotics all over the country. Multidrug resistance among typhoid patients is increasing in a threatening way. Finally this study suggests a national guideline for antibiotic use in Bangladesh.
Conflict of interest statement
We declare that we have no conflict of interest.
Acknowledgements
Authors would like to thank Chittagong University Research Cell for financial grant for conducting the work(Ref No. 5301/Res/Dir/CU/2012). Special gratitude to Chevron diagnostics (Chittagong), Surgiscope hospital (Chittagong), Comfort Diagnostic Center (Pvt.) Limited (Dhaka) and Popular Diagnostic Centre (Rajshahi) for their help during the study.
Comments
Background
Salmonella entericaserotype typhi is a human restricted pathogen, which causes typhoid fever, and leads to a high rate of global morbidity and mortality. Ideal antimicrobial treatment of patients with enteric fever depends on an understanding of local patterns of antimicrobial resistance and is enhanced by the results of antimicrobial susceptibility testing of theSalmonellaisolated from the individual patient. Drug resistant variants are evolving and clinicians need to be aware that patients infected with resistantSalmonellavariants may not respond adequately.
Research frontiers
The present research work depicts antibiotic resistance pattern ofS. typhiclinical isolates from Bangladesh. In this study the authors have collected samples from different part of the country. Although the sample size is small, it reflects the overall antibiotic resistance pattern againstS. typhiin the population.
Related reports
Previous reports also showed similar finding especially in Dhaka region. Ahmedet al.(2006) and Sahaet al.(2001) got same type of resistance pattern earlier.
Innovations and breakthroughs
Although the only source ofS. typhiis infected humans, and fecal contamination in drinking water and food supplies leads to this disease, the authors have showed that antibiotic resistance pattern does not depend on the population density. They also showed abundance of drug resistance strains in the population which is a matter of concern, since they have conducted the study in a highly populated developing country.
Applications
In case of invasive infections and enteric fever, antibiotics are administered. If not treated properly, enteric fever carries a high mortality rate, while the rate is reduced to minimal if treatment is available straightaway. In cases of enteric fever, it is often necessary to commence treatment before the laboratory sensitivity testing results are available. This often leads to treatment failure and multidrug resistance. Therefore, it is important to study the antibiotic resistance pattern ofS. typhiin a population to predict a better treatment strategy.
Peer review
This is an interesting research work in which authors have demonstrated antibiotic resistance pattern ofS. typhiclinical isolates in a highly populated developing country. Fecal contamination in drinking water and food supplies leads to spread ofS. typhiinfection. The general speculation would be higher resistant pattern in highly dense populated area; however, the authors have showed that there is no relation between population density and evolving of resistant strains. Moreover, the authors have showed the overall resistant pattern ofS. typhiin population level, this information can be important for clinicians to provide treatment.
[1] Islam M, Das K, Sharmin N, Hasan M, Azad A. Antimicrobial susceptibility of Salmonella serovars isolated from blood. J Innov Dev Strategy 2008; 2: 22-27.
[2] Nagshetty K, Channappa ST, Gaddad SM. Antimicrobial susceptibility of Salmonella typhi in India. J Infect Dev Ctries 2010; 4: 70-73.
[3] Harish B, Menezes G. Antimicrobial resistance in typhoidal Salmonellae. Indian J Med Microbiol 2011; 29: 223.
[4] Chandrasiri P, Elwitigala J, Nanayakkara G, Chandrasiri S, Patabendige G, Karunanayaka L, et al. A multi centre laboratory study of Gram negative bacterial blood stream infections in Sri Lanka. Ceylon Med J 2013; 58: 56-61.
[5] Rushdy AA, Mabrouk MI, Abu-Sef FA-H, Kheiralla ZH, All SMA, Saleh NM. Contribution of different mechanisms to the resistance to fluoroquinolones in clinical isolates of Salmonella enterica. Braz J Infect Dis 2013; 17(4): 431-437.
[6] Threlfall EJ, Ward LR, Skinner JA, Smith HR, Lacey S. Ciprofloxacin-resistant Salmonella typhi and treatment failure. Lancet 1999; 353: 1590-1591.
[7] Mulvey MR, Boyd DA, Finley R, Fakharuddin K, Langner S, Allen V, et al. Ciprofloxacin-resistant Salmonella enterica serovar Kentucky in Canada. Emerg Infect Dis 2013; 19: 999-1001.
[8] Lunguya O, Lejon V, Phoba MF, Bertrand S, Vanhoof R, Glupczynski Y, et al. Antimicrobial resistance in invasive nontyphoid Salmonella from the Democratic Republic of the Congo: emergence of decreased fluoroquinolone susceptibility and extended-spectrum beta lactamases. PLoS Negl Trop Dis 2013; 7: e2103.
[9] Zhang R, Eggleston K, Rotimi V, Zeckhauser RJ. Antibiotic resistance as a global threat: evidence from China, Kuwait and the United States. Global Health 2006; 2: 1-14.
[10] Dutta S, Sur D, Manna B, Sen B, Bhattacharya M, Bhattacharya SK, et al. Emergence of highly fluoroquinolone-resistant Salmonella enterica serovar typhi in a community-based fever surveillance from Kolkata, India. Int J Antimicrob Agents 2008; 31: 387-389.
[11] Choudhary A, Gopalakrishnan R, Nambi P, Ramasubramanian V, Ghafur K, Thirunarayan M. Antimicrobial susceptibility of Salmonella enterica serovars in a tertiary care hospital in southern India. Indian J Med Res 2013; 137: 800-802.
[12] Zhang J, Jin H, Hu J, Yuan Z, Shi W, Ran L, et al. Serovars and antimicrobial resistance of non-typhoidal Salmonella from human patients in Shanghai, China, 2006-2010. Epidemiol Infect 2013; 10: 1-7.
[13] Rahman A, Ahmed M, Begum R, Ghosh A, Hossain M. Multidrug resistant typhoid fever in children: a review. J Dhaka Med Coll 2008; 17: 121-126.
[14] Radji M, Fauziah S, Aribinuko N. Antibiotic sensitivity pattern of bacterial pathogens in the intensive care unit of Fatmawati Hospital, Indonesia. Asian Pac J Trop Biomed 2011; 1: 39-42.
[15] Sun L, Klein EY, Laxminarayan R. Seasonality and temporal correlation between community antibiotic use and resistance in the United States. Clin Infect Dis 2012; 55: 687-694.
[16] Bosso J, Mauldin P, Salgado C. The association between antibiotic use and resistance: the role of secondary antibiotics. Eur J Clin Microbiol Infect Dis 2010; 29: 1125-1129.
[17] Boyle VJ, Fancher ME, Ross RW Jr. Rapid, modified Kirby-Bauer susceptibility test with single, high-concentration antimicrobial disks. Antimicrob Agents Chemother 1973; 3: 418-424.
[18] Kiehlbauch JA, Hannett GE, Salfinger M, Archinal W, Monserrat C, Carlyn C. Use of the National Committee for Clinical Laboratory Standards guidelines for disk diffusion susceptibility testing in New York state laboratories. J Clin Microbiol 2000; 38: 3341-3348.
[19] Chandy SJ, Mathai E, Thomas K, Faruqui AR, Holloway K, Lundborg CS. Antibiotic use and resistance: perceptions and ethical challenges among doctors, pharmacists and the public in Vellore, South India. Indian J Med Ethics 2012; 10: 20-27.
[20] Adabara N, Ezugwu B, Momojimoh A, Madzu A, Hashiimu Z, Damisa D. The prevalence and antibiotic susceptibility pattern of Salmonella typhi among patients attending a military hospital in Minna, Nigeria. Adv Prev Med 2012; doi: 10.1155/2012/875419.
[21] Ahmed D, D’Costa LT, Alam K, Nair GB, Hossain MA. Multidrugresistant Salmonella enterica serovar typhi isolates with high-level resistance to ciprofloxacin in Dhaka, Bangladesh. Antimicrob Agents Chemother 2006; 50: 3516-3517.
[22] Rahman M, Siddique A, Shoma S, Rashid H, Salam M, Ahmed Q, et al. Emergence of multidrug-resistant Salmonella enterica serotype typhi with decreased ciprofloxacin susceptibility in Bangladesh. Epidemiol Infect 2006; 134: 433-438.
[23] Akter L, Hassan M, Ahmed Z. Present status and antibiotic sensitivity pattern of Salmonella typhi and S. paratyphi in different age group hospitalized patients in Dhaka city, Bangladesh. IOSR J Pharm Biol Sci 2012; 4: 27-30.
[24] Al-Gallas N, Abbassi MS, Gharbi B, Manai M, Ben Fayala MN, Bichihi R, et al. Occurrence of plasmid-mediated quinolone resistance determinants and rmtB gene in Salmonella enterica serovar enteritidis and typhimurium isolated from food-animal products in Tunisia. Foodborne Pathog Dis 2013; 10(9): 813-819.
[25] Leung DT, Das SK, Malek M, Ahmed D, Khanam F, Qadri F, et al. Non-typhoidal Salmonella gastroenteritis at a diarrheal hospital in Dhaka, Bangladesh, 1996-2011. Am J Trop Med Hyg 2013; 88: 661-669.
[26] Farmakiotis D, Varughese J, Sue P, Andrews P, Brimmage M, Dobroszycki J, et al. Typhoid fever in an inner city hospital: A 5-year retrospective review. J Travel Med 2013; 20: 17-21.
[27] Naheed A, Ram PK, Brooks WA, Hossain MA, Parsons MB, Talukder KA, et al. Burden of typhoid and paratyphoid fever in a densely populated urban community, Dhaka, Bangladesh. Int J Infect Dis 2010; 14: e93-e99.
[28] Gautam V, Gupta NK, Chaudhary U, Arora D. Sensitivity pattern of Salmonella serotypes in Northern India. Braz J Infect Dis 2002; 6: 281-287.
[29] Mishra MP, Debata NK, Padhy RN. Surveillance of multidrug resistant uropathogenic bacteria in hospitalized patients in Indian. Asian Pac J Trop Biomed 2013; 3: 315-324.
[30] Van den Bogaard A, London N, Driessen C, Stobberingh E. Antibiotic resistance of faecal Escherichia coli in poultry, poultry farmers and poultry slaughterers. J Antimicrob Chemother 2001; 47: 763-771.
[31] Cummings KJ, Perkins GA, Khatibzadeh SM, Warnick LD, Altier C. Antimicrobial resistance trends among Salmonella isolates obtained from dairy cattle in the northeastern United States, 2004-2011. Foodborne Pathog Dis 2013; 10: 353-361.
[32] Mahmud MS, Bari ML, Hossain MA. Prevalence of Salmonella serovars and antimicrobial resistance profiles in poultry of Savar area, Bangladesh. Foodborne Pathog Dis 2011; 8: 1111-1118.
[33] Nandi SP, Sultana M, Hossain MA. Prevalence and characterization of multidrug-resistant zoonotic Enterobacter spp. in poultry of Bangladesh. Foodborne Pathog Dis 2013; 10: 420-427.
[34] Thai TH, Hirai T, Lan NT, Yamaguchi R. Antibiotic resistance profiles of Salmonella serovars isolated from retail pork and chicken meat in North Vietnam. Int J Food Microbiol 2012; 156: 147-151.
[35] Kumarasamy KK, Toleman MA, Walsh TR, Bagaria J, Butt F, Balakrishnan R, et al. Emergence of a new antibiotic resistance mechanism in India, Pakistan, and the UK: a molecular, biological, and epidemiological study. Lancet Infect Dis 2010; 10: 597-602.
[36] Ioannidis A, Papavasileiou K, Papavasileiou E, Bersimis S, Chatzipanagiotou S. Distribution of six effector protein virulence genes among Salmonella enterica enterica serovars isolated from children and their correlation with biofilm formation and antimicrobial resistance. Mol Diagn Ther 2013; 17(5): 311-317.
[37] Koletzko S, Richy F, Bontems P, Crone J, Kalach N, Monteiro ML, et al. Prospective multicentre study on antibiotic resistance of Helicobacter pylori strains obtained from children living in Europe. Gut 2006; 55: 1711-1716.
10.12980/APJTB.4.2014C770
*Corresponding author: Adnan Mannan, Department of Genetic Engineering and Biotechnology, University of Chittagong, Chittagong-4331, Bangladesh.
Tel: +88-031716552 (4414)
E-mail: adnan_orko@yahoo.com
Foundation Project: Supproted by Chittagong University Research Cell (Grant No.: Ref No. 5301/ Res/ Dir/ CU/ 2012).
Article history:
Received 4 Feb 2014
Received in revised form 9 Feb, 2nd revised form 15 Feb, 3rd revised form 19 Feb 2014
Accepted 23 Mar 2014
Available online 28 Apr 2014
Methods:The antibiotic susceptibility of 70 clinical isolates collected from blood, sputum, urine and pus samples were identified by specific antisera and with standard biochemical tests. The patients were divided into 5 age groups. Susceptibility and resistance was also tested by Kirby-Bauer disc diffusion method using 12 regularly used antibiotics.
Results:Antibiotic susceptibility test demonstrated that 64.28% isolates of Salmonella typhi were multidrug resistant. Present study suggests that the clinical samples were mostly resistant against nalidixic acid with all age groups and in all three divisions with similar resistance pattern. Resistance is more common among adult people (30-40 years) and children (0-10 years). Salmonella typhi was mostly sensitive against gentamycin, chloramphenicol and ciprofloxacin.
Conclusions:Although the population density of Dhaka region is markedly higher than Rajshahi and Chittagong regions, no significant difference in resistance pattern was found. The rate of multidrug resistance is a matter of concern. Physicians should reconsider before prescribing nalidixic acid and cefixime. Further molecular study is needed to reveal the genomic and proteomic basis of resistance.
杂志排行

Asian Pacific Journal of Tropical Biomedicine的其它文章
- The effects of exposure to pesticides on the fecundity status of farm workers resident in a rural region of Fars province, southern Iran
- Phytochemical and in vitro biological investigations of methanolic extracts of Enhydra fluctuans Lour.
- Comparative susceptibility to permethrin of two Anopheles gambiae s.l. populations from Southern Benin, regarding mosquito sex, physiological status, and mosquito age
- Effects of melatonin on changes in cognitive performances and brain malondialdehyde concentration induced by sub-chronic coadministration of chlorpyrifos and cypermethrin in male Wister rats
- In vitro anti oxidant activity and acute oral toxicity of Terminalia paniculata bark ethanolic extract on Sprague Dawley rats
- Theoretical and experimental study on lipophilicity and wound healing activity of ginger compounds