布洛芬及吲哚美辛治疗婴儿动脉导管未闭的Meta分析
2014-03-04杨琼芳
杨琼芳
(重庆医科大学附属儿童医院药房 400014)
动脉导管未闭(patent ductus arteriosus,PDA)是早产儿最常见的先天性心脏病,其在早产儿发生率约为55%~70%,其发生率女孩明显高于男孩[1]。尽管动脉导管在健康及成熟的新生儿有自行闭合的可能,但是如果并发呼吸窘迫综合征(respiratory distress syndrome,RDS),其可以加重呼吸衰竭的发生[1-2]。研究发现PDA可增加成熟婴儿其患慢性肺疾病、坏死性小肠结肠炎(necrotizing enterocolitis,NEC),心室内出血的风险,同时这类患儿往往神经发育较差和相对较高的死亡率[3-4]。吲哚美辛是一种前列腺素合成酶抑制剂,1976年首次报道用于临床关闭PDA[5]。后续研究发现吲哚美辛可以影响婴儿肾、胃肠道、脑灌注,并可能导致并发症,如NEC、肾功能(blood urea nitrogen,Bun)不全、消化道出血、并减少脑细胞的氧供应[6-7]。
布洛芬是一种非甾体类抗炎药,近年来研究被证明能有效地关闭PDA,而不降低脑血流量或影响肠道或肾脏血流动态[8-9]。目前,有较多关于布洛芬和吲哚美辛治疗PDA的对照研究,但结果不尽相同。为探讨两药疗效和不良反应的差异,本文应用Meta分析对这些研究进行系统评价,得出客观的结论。
1 资料与方法
1.1 一般资料 通过检索Medline、Cochrane Controlled Trials Register、EMBASE、EDOS数据库,检索系统以“ibupr ofen&indo methacin &patent ductus arteriosus”为主题词进行检索。
1.2 入选标准 选择纳入的研究必须满足:(1)随机对照研究;(2)疗效监测报告中,至少包括用药后PDA的关闭情况;(3)使用类似的患者特性:所有纳入研究的患者均是诊断PDA未经过其他治疗措施;(4)必须超声心动图证实PDA;(5)纳入的研究均是以布洛芬和吲哚美辛分别作为实验组及对照组进行的研究。
1.3 文献筛选及数据提取 由2名评价者独立阅读文献全文,按照纳入和排除标准筛选文献,意见不统一时通过集体讨论解决。数据提取由2名评价者独立完成,交叉对比,并且删除文献作者、刊名、年份等资料后开始提取,不足的数据通过联系作者补充。
1.4 数据收集 数据收集包括用药后PDA的闭合率、NEC的发生率、血清尿素氮水平、尿量。2名研究者独立阅读相同的文献,提取数据,完成后共同比较讨论数据以达到一致的结果。
1.5 纳入研究方法学质量评价结果 根据Jadad Scale推荐的质量评价方法,文献得分3~5分视为高质量,纳入的17篇文献方法学质量评价结果见表1。
1.6 统计学处理 采用Cochrane协作网提供的Rev Man5.2统计学软件计算统计学异质性和疗效的效应量,对具有临床同质性的资料计算合并效应量。文献的发表偏倚采用漏斗图统计,漏斗图左右对称表示无发表偏倚。资料的同质性检验采用χ2检验,并采用χ2检验对同质性进行定量分析。当χ2检验P>0.1,且I2<50%时,表明无统计学异质性,采用固定效应模型;当P<0.1,且I2>50%时,表明有统计学异质性,采用随机效应模型。计量资料以均数差(difference in means)表示,计数资料以相对危险度(relative risk)表示。疗效的合并效应量采用区间估计和假设检验,区间估计采用95%CI,假设检验显著性水平设定为0.05,以P<0.05为差异有统计学意义。
2 结 果
2.1 文献检索结果 共检索到102篇文献,2名研究者通过独立及讨论仔细阅读文献全文,排除不符合纳入标准、综述性、单个干预措施、重复发表的研究,排除回顾性研究及原始资料无法获取的研究,最终纳入17个研究,均为RCT。共纳入974例患者,见表2。
2.2 Meta分析结果
2.2.1 发表偏倚 采用漏斗图分析各个统计分析的发表偏倚,如图1所示,各漏斗图基本对称,说明17个研究之间无明显发表偏倚。
2.2.2 PDA闭合率 全部17篇文献均报道患儿的PDA的闭合率,共纳入974例患儿,其中布洛芬组508例,吲哚美辛组466例。统计闭合率的17篇文献中,各研究间无统计学异质性(I2=0,P=0.70),故采用固定效应模式合并效应量。Meta分析显示布洛芬与吲哚美辛对治疗PDA的闭合率比较差异无统计学意义[95%CI:0.97~1.10,P=0.34],图2。

表1 纳入文献方法学质量评价结果

表2 纳入研究文献的基本情况
2.2.3 尿量的比较 纳入的研究中6篇文献报道两组治疗后尿量情况[12-13,17-18,21,24],共506例 患 儿,其 中 布 洛 芬 组261例,吲哚美辛组245例。分析发现各研究间存在统计学异质性(I2=87%,P<0.05),故采用随机效应模式合并效应量。Meta分析显示布洛芬与吲哚美辛在治疗PDA对患儿尿量的影响差异有统计学意义[95%CI:0.17~1.00,P=0.005],图3。吲哚美辛治疗PDA明显减少患儿尿量,对患儿肾脏影响较布洛 芬大。

图1 各篇研究文献之间发表偏倚情况
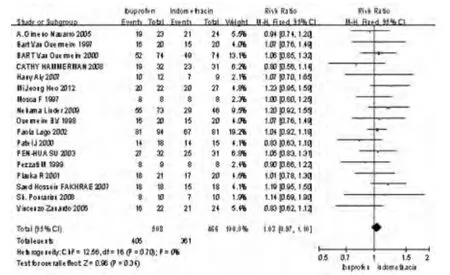
图2 布洛芬及吲哚美辛治疗PDA闭合率
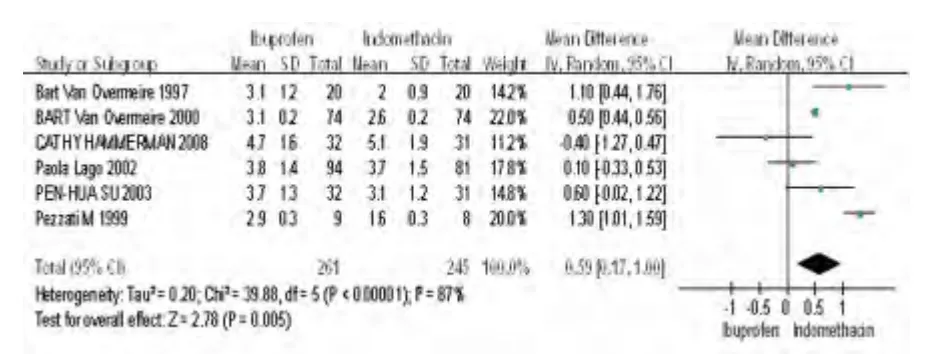
图3 布洛芬及吲哚美辛治疗PDA对患儿尿量的影响
2.2.4 对Bun的影响 本Meta分析中共4篇文献报道治疗后患儿Bun情况[10-12,16],共169例患儿,其中布洛芬组84例,吲哚美辛组85例。分析发现各研究间无统计学异质性(I2=0,P<0.85),故采用固定效应模式合并效应量。Meta分析显示布洛芬与吲哚美辛在治疗PDA对患儿Bun的影响差异有统计学意义[95%CI:-8.28~-0.63,P=0.02],吲哚美辛治疗PDA对患儿Bun影响较布洛芬大(图4)。

图4 布洛芬及吲哚美辛治疗PDA对患儿Bun的影响
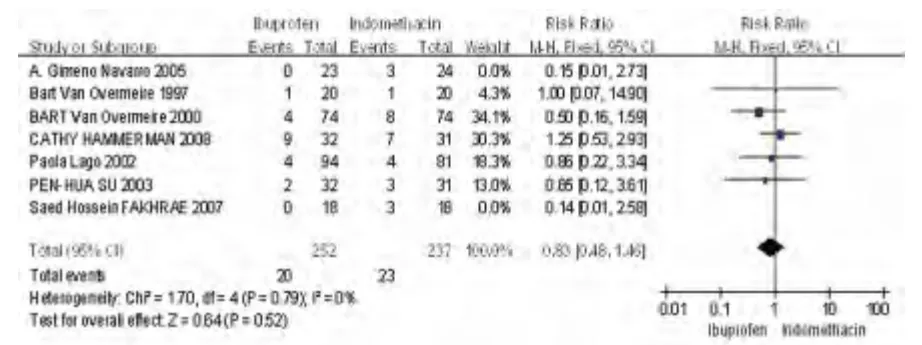
图5 布洛芬及吲哚美辛治疗PDA对患儿NEC的发生率
2.2.5 NEC发生率 纳入的研究中7篇文献报道2组的NEC发生情况[11-13,15,17-18,21],共572例患儿,其中布洛芬组293例,吲哚美辛组279例。其中文献[11,21]中有频数0,故排除这2篇文献合并效应量。各研究间无统计学异质性(I2=0,P=0.79),故采用固定效应模式合并效应量。Meta分析显示布洛芬与吲哚美辛在治疗PDA的NEC比较差异无统计学意义[95%CI:0.48~1.46,P=0.52],见图5。
3 讨 论
PDA是早产儿常见的先天性心脏病,发生率较高。这是早产儿由于动脉导管壁平滑肌发育不成熟,管径大、管壁薄,缺乏肌肉组织,生后导管常不能很快闭合,出现左向右分流和左室容量负荷过重而发生充血性心力衰竭;是影响早产儿存活率和后遗症发生率的主要原因之一,故应积极治疗。
吲哚美辛是较早治疗PDA的药物,该药是一种前列腺合成抑制剂,能有效治疗PDA。但有文献报道,吲哚美辛治疗PDA会导致患儿肾功能、颅内出血、NEC、出血倾向、血糖降低,所以限制了其在临床上的应用[27]。近年来,有文献报道布洛芬同样有治疗PDA的疗效,同时对患儿肾脏功能的影响较小[17]。目前,国内外有较多的关于布洛芬及吲哚美辛治疗PDA的随机对照研究,但其结果不尽相同。
本文通过对17篇纳入的文献进行Meta分析,系统评价其对PDA的疗效。纳入的17篇文献,通过Jadad Scale推荐的质量评价方法对其进行质量评价,结果显示各文献质量较高,均符合纳入研究进行Meta分析。本文Meta分析结果显示,布洛芬及吲哚美辛治疗PDA有相似的效果,差异无统计学意义(P>0.05);但吲哚美辛对患儿的尿量有明显的影响,减少患儿尿量,差异有统计学意义(P<0.05),其原因可能是吲哚美辛影响患儿肾脏灌注[18]。本文同时分析2种药物治疗PDA对患儿Bun的影响,分析发现吲哚美辛组Bun较布洛芬组明显升高,提示吲哚美辛对患儿Bun影响较布洛芬大。
Meta分析结果显示,2种药物治疗PDA的NEC发生率吲哚美辛虽然高于布洛芬,但差异无统计学意义(P>0.05),说明2种药物治疗患儿PDA时NEC的发生率无明显差异,这与国外其他研究结果相似[28]。
综上所述,布洛芬在治疗PDA方面,具有与吲哚美辛相似的效果,同时布洛芬对患儿肾脏影响明显小于吲哚美辛,其他方面不良反应2种药物基本相似,故本文通过对大量随机对照研究分析提示布洛芬在治疗PDA方面较吲哚美辛安全,具有临床用药优越性。
[1]Hermes-DeSantis ER,Clyman RI.Patent ductus arteriosus:pathophysiology and management[J].J Perinatol,2006,26(Suppl 1):S14-S18.
[2]Sekar KC,Corff KE.Treatment of patent ductus arterio-sus:indomethacin or ibuprofen?[J].J Perinatol,2008,28(Suppl 1):S60-S62.
[3]Bancalari E,Claure N,Gonzalez A.Patent ductus arteriosus and respiratory outcome in premature infants[J].BiolNeonate,2005,88(3):192-201.
[4]Meyers RL,Alpan G,Lin E,et al.Patent ductus arteriosus,indomethacin,and intestinal distension:effects on in-testinal blood flow and oxygen consumption[J].PediatrRes,1991,29(6):569-574.
[5]Friedman WF,Hirschklaw MJ,Printz MP,et al.Pharma-cologic closure of patent ductus arteriosus in the premature infant[J].N Engl J Med,1976,295(10):526-529.
[6]Yeh TF,Car I.Pharmacologic closure of patent ductus arteriosus[M].2 nd edn.St Louis:Neonatal Therapeutics,Mosby Year Book,1991:123-138.
[7]Patel J,Roberts I,Azzopardi D,et al.Randomized double-blind controlled trial comparing the effects of ibuprofenwith indomethacin on cerebral hemodynamics in preterminfants with patent dutus arteriosus[J].Pediatr Res,2000,47(1):36-42.
[8]Chemtob S,Beharry K,Rex J,et al.Prostanoids determinethe range of cerebral blood flow autoregulation of new-born piglets[J].Stroke,1990,21(5):777-784.
[9]Chemtob S,Roy MS,Abran D,et al.Prevention of post-asphyxial increase in lipid peroxides and retinal functiondeterioration in the newborn pig by inhibition of cycloox-ygenase activity and free radical generation[J].PediatrRes,1993,33(4 Pt 1):336-340.
[10]Heo MJ,Lee OS,Lim SC.Comparative evaluation for theuse oforal ibuprofen and intravenous indomethacin in Korean infants with patent ductus[J].Arch Pharm Res,2012,35(9):1673-1683.
[11]Fakhraee SH,Badiee Z,Mojtahedzadeh S,et al.Comparison oforal ibuprofen and indomethac in therapy for patent ductus arter iosus in preterm infants[J].Chin J Con-temp Pediatr,2007,9(5):399-403.
[12]Su PH,Chen JY,Su CM,et al.Comparison of ibuprofenand indomethacin therapy for patent ductus arteriosus inpreterm infan[J].Pediatrics International,2003,45(6):665-670.
[13]Hammerman C,Shchors I,Jacobson S,et al.Ibuprofenversus continuous indomethacin in premature neonateswith patent ductus arteriosus:is the difference in themode of administration?[J].Pediatr Res,2008,64(3):291-297.
[14]Overmeire BV,Follens I,Hartmann S,et al.Ibuprofen vsIndomethacin for treatment of PDA in preterm infants[J].Indian Pediatrics,1998,35(3):292-293.
[15]Gimeno Navarro A,Cano Sánchez A,Femández Gilino C,et al.Ibuprofeno frente a indometacina en el tratamientodel conducto arterioso persistente del prematuro[J].AnPediatr(Barc),2005,63(3):212-218.
[16]Aly H,Lotfy W,Badrawi N,et al.Oral Ibuprofen andductus arteriosus in premature infants:a randomized pilotstudy[J].Ame J Perinatol,2007,24(5):267-270.
[17]Lago P,Bettiol T,Salvadori S,et al.Safety and efficacy ofibuprofen versus indomethacin in preterm infants treatedfor patent ductus arteriosus:a randomised controlled trial[J].Eur J Pediatr,2002,161(4):202-207.
[18]Overmeire BV,Follens I,Hartmann S,et al.Treatment ofpatent ductus arteriosus with ibuprofen[J].Arch DisChild,1997,76(3):179-184.
[19]Linder N,Bello R,Hernandez A,et al.Treatment of patent ductus arteriosus:indomethacin or ibuprofen?[J].Ame J Perinatol,2010,27(5):399-404.
[20]Pourarian SH,Pishva N,Madani A,et al.Comparison oforal ibuprofen and indomethacin on closure of patent ductus arteriosus in preterm infants[J].East MediterrHealth J,2008,14(2):360-365.
[21]Van Overmeire B,Smets K,Lecoutere D,et al.A comparison of ibuprofen and indomethacin for closure of patentductus arteriosus[J].New Engl J Med,2000,343(10):674-681.
[22]Zanardo V,Vedovato S,Lago P,et al.Effects of ibuprofenand indomethacin on urinary antidiuretic hormone excretion in preterm infants treated for patent ductus arteriosus[J].Fetal Diagn Ther,2005,20(6):534-539.
[23]Mosca F,Bray M,Lattanzio M,et al.Comparative evaluation of the effects of indomethacin and ibuprofen on cerebral perfusion and oxygenation in preterm infants withpatent ductus[J].J Pediatr,1997,131(4):549-554.
[24]Pezzati M,Vangi V,Biagiotti R,et al.Effects of indom-ethacin and ibuprofen on mesenteric and renal blood flowin preterm infants with patent ductus arteriosus[J].J Pediatrics,1999,135(6):733-738.
[25]Patel J,Roberts I,Azzopardi D,et al.Randomized double-blind controlled trial comparing the effects of ibuprofenwith indomethacin on cerebral hemody namics in preterminfants with patent ductus arteriosus[J].Pediatric Res,2000,47(1):36-42.
[26]Plavka R,Svihovec P,Borek I,et al.Ibuprofen vs indom-ethacin in the treatment of patent ductus arteriosus invery premature neonates[J].Pediatr Res,2001,49:375A.
[27]Hosono S,Ohno T,Kimoto H,et a1.Reduction in bloodglucose values following Indomethacin therapy for patentductus arterious[J].Pediatr Int,1999,41(5):525-528.
[28]Thomas RL,Parker GC,Overmeire BV,et al.A meta-a-nalysis of ibuprofen versus indomethacin for closure ofpatent ductus arteriosus[J].Eur J Pediatr,2005,164(3):135-140.