Mental health literacy among residents in Shanghai
2013-12-09JingyiWANGYanlingHEQingJIANGJunCAIWeilingWANGQingzhiZENGJumingMIAOXuejunQIJianxinCHENQianBIANChunCAINingMAZiqingZHUMingyuanZHANG
Jingyi WANG, Yanling HE*, Qing JIANG, Jun CAI, Weiling WANG, Qingzhi ZENG, Juming MIAO,Xuejun QI, Jianxin CHEN, Qian BIAN, Chun CAI, Ning MA, Ziqing ZHU, Mingyuan ZHANG
•Original article•
Mental health literacy among residents in Shanghai
Jingyi WANG1, Yanling HE1*, Qing JIANG1, Jun CAI1, Weiling WANG1, Qingzhi ZENG1, Juming MIAO1,Xuejun QI1, Jianxin CHEN1, Qian BIAN1, Chun CAI2, Ning MA2, Ziqing ZHU1, Mingyuan ZHANG1
1. Introduction
Globally, there are approximately 450 million individuals with mental or behavioral disorders,[1]the majority of whom never receive treatment.[2,3]Lack of treatment– which is more common in low- and middle-income countries than in high-income countries (85% v. 54%)[4]– may be related to low community awareness about mental illness.[5,6]Interventions aimed at improving public awareness about mental health issues should,theoretically, increase care-seeking and result in the improved prevention and control of mental illnesses.[7,8]
Previous studies that assessed public awareness about mental health issues (often called ‘mental health literacy’)cover a variety of topics: community members’ knowledge about the causes and appropriate interventions for mental disorders; public attitudes about mental disorders and about persons with mental disorders; the ability of community members to identify different types of mental disorders; and public awareness about sources of information about mental health.[9,10]Most of these studies focused on depressive disorders or schizophrenia;some also considered other affective disorders, alcohol dependence, drug abuse, anxiety disorders and dementia.[11]However, it is difficult to compare results from these studies because they use different methods to assess mental health literacy.
In the current study we administered a questionnaire about mental health literacy to a representative sample of adults living in Shanghai. The survey instrument used was a modified version of subsections of the comprehensive‘Questionnaire of Mental Health Work’ developed by the Chinese Ministry of Health for use across China which includes case vignettes about five types of mental disorders.[12]Conducted prior to the passage of China’s new mental health law,[13]the study provides information about the use of standardized methods for assessing mental health literacy and establishes a baseline measure that can be reassessed periodically as the new law is implemented.
2. Methods
2.1 Sample
The target population was permanent residents of Shanghai 15 years of age or older. The process of identifying respondents is shown in Figure 1. The survey was conducted from September to November 2011 in all 19 districts of Shanghai. One sub-district that agreed to participate was identified from each district and then five neighborhoods were randomly sampled from each of these 19 sub-districts. Twenty-five residents were randomly selected from each neighborhood using the resident lists (that had been updated by collaborators at psychiatric hospitals in each district) of 10 of the 95 identified neighborhoods and 20 residents were randomly selected from each of the other 85 neighborhoods,resulting in a total sample of 1950 individuals. (The two districts that selected 25 subjects in each of its five neighborhoods did so in order to have a large enough sample to generate reliable district-specific results.)When a selected individual could not be reached, was unwilling to participate, or was unable to complete the survey, the first person of the same gender and similar age (within 5 years) after the original individual on the resident list was selected as a substitute. If the first substitute could not complete the questionnaire either, the next person served as the substitute using the same method of selection until the questionnaire wascompleted. A total of 245 substitutes were identified,including the selected substitutes for 3 individuals in the original sample who were subsequently located (and completed the survey) and the substitutes for 29 cases in which the first substitute was not located and so a 2ndsubstitute had to be identified. As shown in Figure 1, a total of 1953 individuals completed the survey,including 1737 who were in the original sample and 216 substitutes. Thus the completion rate for those initially sampled was 89.1% (1737/1950).

Figure 1. Identification of study participants
2.2 Assessments
The current study uses two subscales from the Questionnaire of Mental Health Work issued by the Chinese Ministry of Health: the Mental Health Knowledge Questionnaire (MHKQ) and the Case Assessment Questionnaire (CAQ).[12]The MHKQ contains 20 items, which are shown in Table 1; items 1 through 16 are about basic knowledge of mental health issues and the remaining four items ask about awareness of different mental health promotion days. One point is given for each correct answer, so the total score ranges from 0 to 20,with higher scores representing better ‘mental health literacy’. A previous study with an earlier version of this scale among 1237 middle school and high school students[14]reported a Cronbach’s alpha value of 0.73 for the 20 items in the scale, identified 4 factors in an exploratory factor analysis of the results, and reported acceptable test-retest reliability of the total knowledge score among 97 students who repeated the survey one week after the first administration of the survey (r=0.68,p<0.001). The reliability and validity of the final version of this scale in adult community members have not, as yet, been assessed.
The original version of the CAQ section has five cases that describe depression, mania, schizophrenia with positive symptoms, schizophrenia with negative symptoms, and obsessive-compulsive disorder (OCD).The current study changed the case of OCD into a case of generalized anxiety disorder (GAD). Respondents are asked to answer nine questions following each case description; the questions are shown in Table 2: the first two questions ask the respondent to identify the condition; the third question asks about the cause of the condition; the fourth question asks respondents to select the most appropriate intervention; and questions 5 to 9 ask about attitudes towards persons with the specified type of mental disorder.
In order to quantify respondents’ accuracy in recognizing different types of mental disorders, we developed a new measure, the ‘overall identification score’. For each of the five conditions described in the vignettes,a score ranging from 0 to 3 was computed based on responses to the first two questions as follows: (a) if the respondent correctly identifies the specific condition on the second question a full score (three points) is given regardless of the response on the first question;(b) if the respondent’s answer to question 2 identifies a condition that is in the same group as the correct response (depression, OCD, and GAD are considered one group; schizophrenia and mania are considered the second group) the score is 2, regardless of the response to question 1; (c) if the respondent’s answer to question 2 is not in the same group as the correct response but the response to question 1 indicates that this is a ‘mental problem’, the score is 1; and (d) if the respondent did not consider the condition a mental problem in question 1 and did not identify a condition in the same group as the correct response in question 2, the score is 0. The final ‘overall identification score’ was the sum of scores from the five cases, ranging from 0 to 15. The reliability and validity of this measure have never been assessed.
2.3 Survey method
In group sessions or home visits, interviewers explained the aim of the study and the confidentiality principles to participants and then obtained their oral consent. The survey was administered as a self-completion questionnaire that each respondent completed independently.But if a respondent had difficulty understanding the questionnaire or was unable to read the questionnaire due to poor sight or low literacy, interviewers read the items to the participant and recorded the answers. Most respondents completed the survey within 30 minutes.Interviewers include 125 staff members from the prevention departments of psychiatric hospitals in each of Shanghai’s 19 districts; they were collectively trained to administer the survey by the mental health division of the Shanghai Centers for Disease Control.
This study is part of an annual national survey on mental health literacy, the Shanghai component of which was approved by the Shanghai Municipal Bureau of Health.
2.4 Statistical analysis
Data were analyzed using SPSS software version 17.0.Descriptive statistics were presented for each item in both MHKQ and CAQ. The internal consistency of the MHKQ was assessed using alpha values. Exploratory principal component factor analysis with varimax rotation with Kaiser normalization of the 20 items in the MHKQ (and, separately, with the first 16 items specifically focused on mental health awareness) that identified factors with an eigenvalue of 1 or greater was conducted in a random sample of 976 of the surveys.A 5-factor model was selected from the exploratory factor analysis and assessed in a confirmatory factor analysis with the remaining 977 surveys. T-tests and ANOVA with post-hoc tests (Bonferroni) were used to compare the mental health literacy score and the overall identification scores of respondents by gender (male v.female), age group (<35 years of age v. >35 years of age),level of education (primary school or lower v. middle school and high school v. college or higher), and marital status (currently married v. not currently married).Multiple linear stepwise regression analysis (p<0.05 for inclusion and p>0.10 for exclusion) was used to identify factors significantly associated with the level of mental health literacy and with the overall identification score.
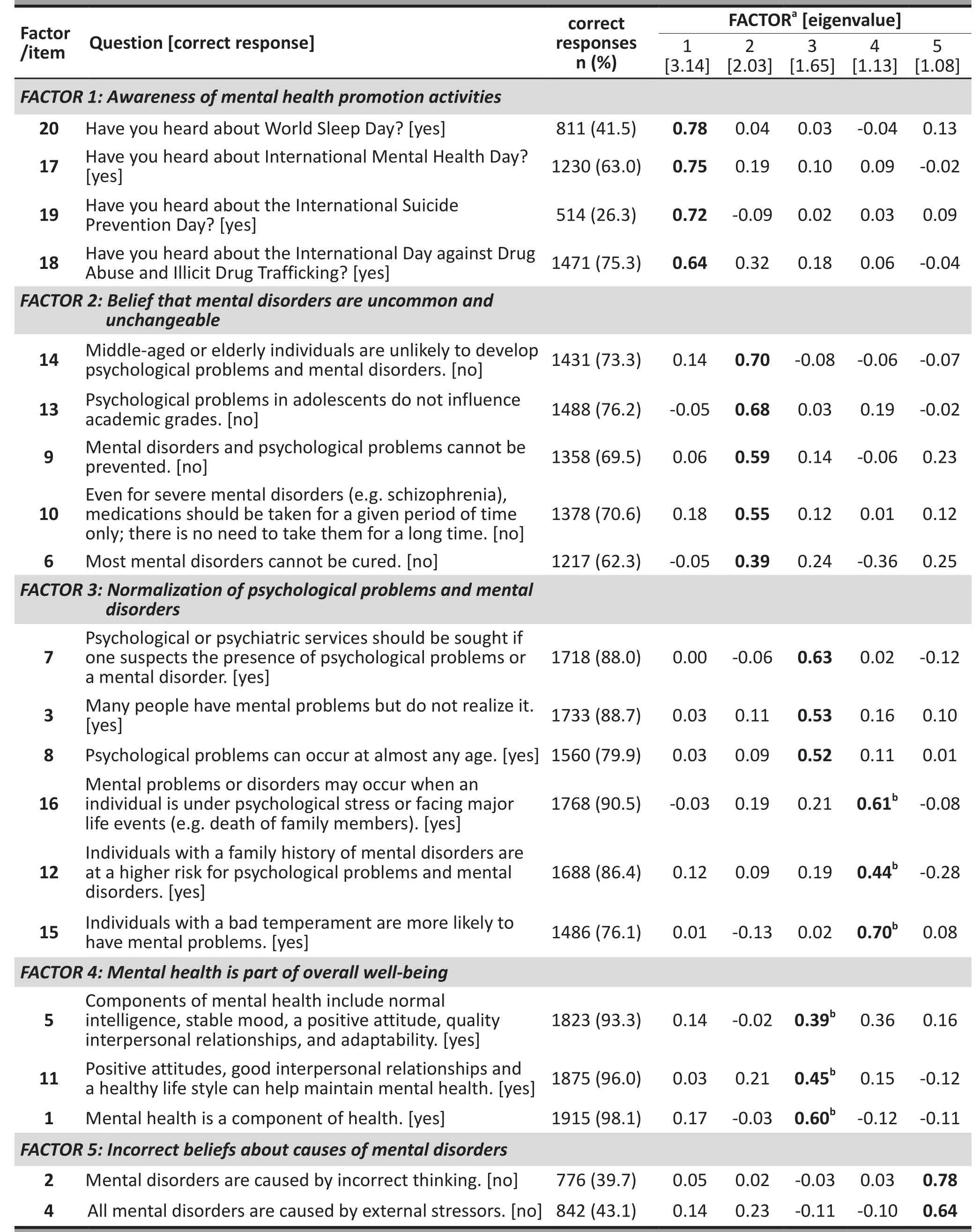
Table 1. Responses to the 20-item mental health knowledge questionnaire by 1953 community residents of Shanghai, and factor loadings in the confirmatory factor analysis (n=977) of the 5-factor model identified in the exploratory factor analysis

Table 2. Percent distribution of responses of 1953 Shanghai community members to questions about five case histories of individuals with different types of psychiatric problems
3. Results
3.1 Demographic characteristics of the sample
A total of 1953 valid questionnaires were collected including 996 (51.0%) from males and 957 (49.0%)from females. The mean (sd) age of all respondents was 50 (17) years. Of all respondents, 476 (24.4%) were under 35 years of age, 1132 (58.1%) were between 35 to 64 years of age, and 340 (17.5%) were 65 or older;277 (14.2%) had an elementary school education or less, 1137 (58.2%) had completed middle school or high school, and 539 (27.6%) had a college education or above. Two hundred and sixty three of the respondents(13.5%) had never married, 1567 (80.2%) were currently married, and 123 (6.3%) were divorced, separated or widowed.

Table 2. Percent distribution of responses of 1953 Shanghai community members to questions about five case histories of individuals with different types of psychiatric problems(continued)
3.2 Mental health literacy
As shown in Table 1, the proportion of respondents who answered each item correctly ranged from 26.3 to 98.1%; the mean correct response rate for the 20 items was 71.9%. The computed mental health literacy score ranged from 6 to 20 and the mean (sd) value was 14.4 (3.1).
The internal consistency of the 20-item MHKQ was fair (Cronbach’s α=0.69) and that of the first 16 items in the scale (excluding the 4 items about mental health promotion) was poor (α=0.59). In both the 20-item and 16-item version of the scale, removal of item 15(“Individuals with a bad temperament are more likely to have mental problems”) resulted in a somewhat higher alpha value, which indicates that the construct assessed by item 15 is different from that assessed by the other items in the scale.
The exploratory factor analysis of 976 randomly selected surveys identified 6 factors with eigenvalues greater than 1 and accounted for 50.3% of the variance.Exploratory factor analysis of the 16-item version of the scale (excluding the 4 items about mental health promotion activities) had essentially the same result.Considering the scree plot of the eigenvalues and the item loadings in the exploratory analysis, we selected a 5-factor model for the 20-item version of the scale as the best representation of distinct constructs considered in the scale (shown in Table 1): Factor 1 included four items about awareness of mental health promotion activities; Factor 2 included five items about beliefs that mental disorders are uncommon and unchangeable;Factor 3 included six items that reflected beliefs about the normalization of mental disorders; Factor 4 included three items related to mental health as a component of overall well-being; and Factor 5 included two items regarding incorrect beliefs about the causes of mental disorders. This model was then tested in a confirmatory factor analysis (which specified the number of factors as five) using the second half of the total sample of surveys(n=977).
The results of this confirmatory factor analysis are shown in Table 1. The model accounted for a total of 45.1% of the overall variance. Three of the factors (Factors 1, 2 and 5) remained the same as in the exploratory factor analysis, but for Factors 3 and 4, the items migrated differently than in the exploratory factor analysis: the three items from the original Factor 4 (items 1, 5 and 11 about mental health and well-being) combined with three of the items in the original Factor 3 (items 3,7 and 8 about normalization of psychological problems) to form a new Factor 3; and the remaining three items in the original Factor 3 (items 12, 15 and 16 about causes of mental disorders) separated from the other items in original Factor 3 to form a new Factor 4. Using the 977 surveys included in the confirmatory factor analysis, the internal consistency of the original items included in Factor 1 (Cronbach’s α=0.73) and Factor 2 (α=0.60) were acceptable, but the internal consistency of the original items included in Factor 3 (α=0.49), Factor 4 (α=0.39)and Factor 5 (α=0.42) were poor.
3.3 Identification of common mental disorders and attitudes about individuals with these conditions
The results for each item on the CAQ for the five vignettes are shown in Table 2. The mean (sd) overall identification score computed from the first two questions of each of the five vignettes on the CAQ was 7.5 (3.0) out of a maximum score of 15. As expected, this overall identification score was moderately correlated with the total mental health literacy score on the MHKQ (r=0.32, p<0.001). Averaging across all five cases, 72% of respondents identified mental problems as the main problem of the individuals described in the vignettes, this value ranged from a low of 50% for generalized anxiety disorder to a high of 87% for schizophrenia. More than 20% of respondents misclassified the main problem in individuals with depression or anxiety disorder as ‘burn-out’.
Correct identification of the specific disorder (question 2 for each vignette) ranged from a low of 19% for schizophrenia with predominantly negative symptoms to a high of 42% for mania. In 25% of cases the depression vignette was misclassified as ‘neurasthenia’, in 27% of cases positive-symptom schizophrenia was misclassified as depression, and in 24% of cases mania was misclassified as schizophrenia. For two of the vignettes more respondents misclassified the condition as another specific disorder than correctly identified the condition:46% of respondents misclassified negative-symptom schizophrenia as depression and 36% of respondents misclassified anxiety disorder as neurasthenia.
The three main causes of these conditions identified by respondents (question 3) were work stress, ‘problems with thinking’ (‘sixiang shang de wenti’, which has no direct translation but implies ‘worrying too much’ and‘poor psychological resilience’), and negative life events.Work stress was the most commonly reported cause of depression and anxiety disorder while problems with thinking were the most commonly reported cause of mania and schizophrenia. The other three potential causes of these conditions included in the survey –hereditary causes, spirit possession and any other cause considered by respondents – were much lesscommonly reported, accounting for a combined total of no more than 10% of attributed causes for depression,anxiety disorder, and schizophrenia and for 14% of the attributed causes for mania. Interestingly, a relatively high proportion of respondents (7.4%) identified spirit possession as the primary cause of mania.

Table 3. Univariate association of selected sociodemographic factors with the level of mental health literacy and the ‘identification score’ (based on the identification of five different psychiatric disorders) of 1953 community residents from Shanghai

Table 4. Stepwise linear regression of factors associated with level of mental health literacy among 1953 community residents from Shanghai
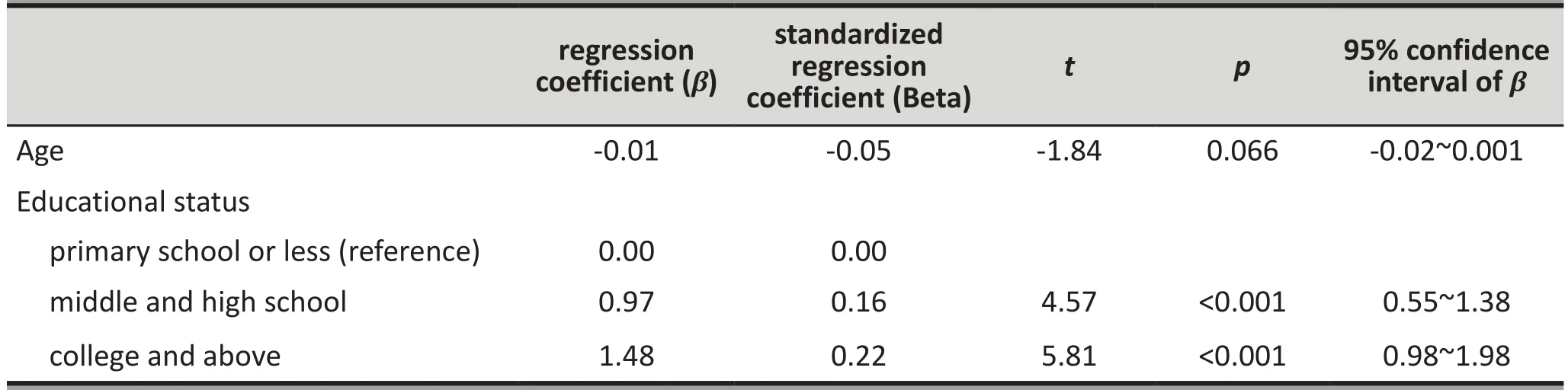
Table 5. Stepwise linear regression of factors associated with the recognition of five common psychiatric conditions by 1953 community residents from Shanghai
Respondents were also asked about help-seeking suggestions for each case (question 4). Seeking psychotherapy (34.2%) and psychiatric services (33.3%) were the two most common suggestions. For depression and anxiety disorder; there was also a substantial portion of respondents who suggested talking to friends and family or ‘relaxing more’.
Respondents’ attitudes about the five conditions described in the vignettes were assessed by CAQ questions 5 through 9. There was a relatively clear divide between the attitudes towards individuals with depression or anxiety disorders versus the attitudes towards individuals with positive-symptom schizophrenia or mania. Respondents were more likely to consider individuals with depression and anxiety ‘normal’, able to differentiate right from wrong, and able to continue working; respondents also felt it more likely that they themselves could (in the future) experience the symptoms of depression and anxiety than those of schizophrenia or mania. Respondents expressed fear about persons with positive-symptom schizophrenia and mania and believed that individuals with these conditions had a substantially increased risk of harming others. On the other hand, negative-symptom schizophrenia was likely to evoke sympathy and was not considered more dangerous to others than depression.
3.4 Association between demographic factors, mental health literacy and recognition of common mental disorders
The univariate and multivariate relationships between demographic factors and mental health literacy and the overall recognition score for common mental health disorders are shown in Tables 3 to 5. Gender and marital status were not significantly associated with either mental health literacy or with the overall recognition score, but younger respondents and those with higher levels of education had better mental health literacy and were more likely to correctly identify the five common mental disorders. When simultaneously considering all factors in the multivariate linear regression analysis, both age and educational status remained independently related to both mental health literacy and the recognition of common mental health disorders, but the relationship between age and the recognition score was only at a trend level (p=0.066).
4. Discussion
4.1 Main findings
4.1.1 Mental health literacy
The ‘2002-2010 China Mental Health Work Plan’[15]set the goal that by 2010 half of the general population would be aware of the characteristics and prevention of mental disorders. The mean overall mental health literacy score identified in this study of 71.9% suggests that this goal has been achieved in Shanghai, though the correct rate for some of the 20 items included in the survey – particularly those about the causes of mental disorders and about awareness of mental health promotion days – were less than 50%. This average correct response rate in Shanghai was higher than the corresponding rates (using the same scale) reported in Guangzhou (60.2%),[16]Changsha (68.5%)[17]and Xi’an(70.3%).[18]Previous studies about mental health literacy in Shanghai conducted in 2002[19]and 2005[20]used a different instrument so it is not possible to compare the current results with the previous results.
Further work – preferably involving both qualitative and quantitative components – is needed to assess the reliability and validity of the MHKQ and to make any necessary revisions. After removal of the four items that assess awareness about mental health promotion activities (and, thus, are not directly related to knowledge about mental illnesses) the internal consistency of the remaining 16 items was poor (Cronbach α=0.59). There were some differences between the results of the exploratory and confirmatory factor analysis and the internal consistency of items included in three of the five identified factors was poor. Moreover, the composition of these five factors was quite different from that of the four factors identified in a study using a slightly different version of the scale with middle school and high school students.[14]And the test-retest reliability of the scale needs to be assessed in adult respondents.
Once the reliability and validity of the scale is confirmed, follow-up studies using exactly the same scale in exactly the same manner at regular intervals are needed to determine whether or not Shanghai (and China) is experiencing the gradual increase in mental health literacy among community members that has been reported in western countries.[21]
4.1.2 Knowledge about cases of common mental disorders The recognition rates of common mental disorders found in this study were somewhat lower than those reported in a community-based study in Australia[5]that used openended questions to assess respondents’ recognition of common mental disorders (unlike the closed-ended questions in this study). The proportion of respondents in Australia who correctly identified depression was 74% versus 35% in this study; and the proportion who recognized schizophrenia in Australia was 37% versus 30% in the current study. In this study schizophrenia was commonly misclassified as depression, and mania was commonly misclassified as schizophrenia. Despite the relatively low rates of recognition of common mental disorders identified in this study from Shanghai, we expect that recognition rates would be even lower in rural areas of China. Clearly, continued effort is needed to increase public awareness about common mental health conditions.
Anxiety disorders are common mental disorders with a reported point prevalence of 5.6% in China[3]But there are few studies either in China or elsewhere that assess public awareness about anxiety disorders. In one study among college students in the United States,[22]41% of respondents were able to recognize generalized anxiety disorder (GAD), about double the 21% who identified the condition in the current study. Interestingly, less than half (49.5%) of Shanghai respondents considered the individual described in the GAD vignette as suffering from a mental disorder, and 41% reported that most people would consider these symptoms ‘normal’. It would appear that in Shanghai (and probably in China more generally) anxiety symptoms are considered a normal part of living that only occasionally justifies being classified as a psychological or psychiatric disorder.
The two main suggestions for help-seeking were psychological counseling and psychiatric services.This finding is consistent with those of another multicenter study in several urban centers in China.[23]But preferences for the source of help were influenced by the attribution of the condition. For example,depression and GAD were commonly considered the outcome of stress at work, ‘burnout’, physical problems,and negative life events, so a substantial proportion of respondents considered more relaxation and talking things over with associates as the most appropriate methods of dealing with the problem.
This study found that individuals with schizophrenia with positive symptoms (i.e., hallucinations and delusions)and individuals with mania are highly stigmatized. A large proportion of respondents expressed concern about adverse behaviors by individuals with these conditions, many believed that these individuals are unable to distinguish right from wrong, and most respondents considered these individuals at high risk of harming others. The relatively high stigma suggests that increased mental health literacy is not necessarily associated with decreased stigma towards mentally ill individuals, a finding that has been reported in western countries.[21]Nonetheless, many respondents also believed that individuals with schizophrenia or mania would be able to continue to work after treatment,suggesting that individuals with these conditions who seek care may experience lower levels of stigma.
4.2 Limitations
The reliability and validity of the MHKQ has not, as yet,been rigorously assessed. One study in middle school students[14]reported acceptable reliability and validity but another study in the general population[17]reported weak internal consistency. The internal consistency of the 20-items scale in this current study was acceptable(alpha=0.69) but correct response rates were over 90%for four items; these overly easy items produce a ‘ceiling effect’ and, thus, decrease the ability of the scale to discriminate persons with relatively high levels of mental health literacy. Further refinements of this scale are needed before it can confidently be employed as the standard for assessing the effectiveness of communitybased mental health promotion campaigns.
At present the CAQ is primarily a descriptive instrument that describes awareness and attitudes about a variety of common mental disorders. The method of assessing the ‘overall identification score’ from the first two questions for each vignette that was developed for this analysis is cumbersome and the reliability of the score is unknown. Moreover, the method of assessing the attributions, suggested treatments, and stigmatization for each of the considered conditions(forcing choices between overlapping categories) has not been standardized, so the interpretation of the results is, necessarily, subjective. And some emerging mental health problems – such as alcohol abuse, drug use and dementia – were not considered in the CAQ. Further research with this scale is needed to assess the reliability of the identification score, to standardize the assessments of attributes and attitudes, and to expand the range of mental health conditions considered.
The most important evaluation of the validity of the MHKQ and CAQ has not yet been attempted in China.The scales will only be useful if they can predict the subsequent behavior of respondents. It needs to be demonstrated that these scales can predict respondents’behavior towards individuals with mental illnesses or their willingness to seek mental health care when they(or their family members) develop a mental illness. The presumed benefits of raising mental health awareness remain controversial.[24,25]The long-held assumption that good mental health literacy improves communitylevel mental health needs to be confirmed in China using longitudinal intervention studies that demonstrate improved mental health outcomes in communities in which mental health promotion efforts have increased mental health literacy.
The selection of the target sub-district from each of the 19 urban districts was not done randomly, it was based on the willingness of the administrators of each subdistrict to participate in the study. The subsequent steps in the sample selection (identification of neighborhoods and of individuals in selected neighborhoods) did use random methods. The selection of cooperative subdistricts may have resulted in a slightly decreased representativeness of the overall sample to the total adult population in Shanghai, but it is unlikely that this had a substantial effect on the overall results of the study. However, the restriction of the study to permanent residents of Shanghai, excluding the large number of migrant workers, may have resulted in a slightly higher estimate of mental health literacy than would be the case if the migrant workers in the city were included in the sample.
4.3 Significance
This cross-sectional study establishes a baseline for the level of mental health literacy and for the level of recognition of common mental disorders in Shanghai.This baseline can be used to compare mental health literacy in Shanghai with that in other locations in the country and, more importantly, it can be used to monitor changes in mental health literacy over time as the mental health promotion activities envisaged in China’s new mental health law are implemented.It should be possible to use these measures to assess the effectiveness of community-based mental health education programs. However, more rigorous assessment of the psychometric properties of the scales used to assess mental health literacy in Chinese respondents (MHKQ and CAQ) is needed; the scales will need to be revised to improve their reliability, validity and utility.
Conflict of interest
The authors report no conflict of interest related to this paper.
Acknowledgment
Authors would like to thank the CDC staff for their support in data collection in the following 19 districts in the city of Shanghai: Songjiang, Changning, Qingpu, Jiading,Hongkou, Jinshan, Minhang, Huangpu, Putuo, Xuhui,Pudong, Zhabei, Yangpu, Nanhui, Chongming, Fengxian,Luwan, Baoshan, and Jing’an. We are also grateful for the cooperation and help in coordination from staff at the various survey sites.
Funding
The study was funded by the Shanghai Municipal Center for Disease Control and Prevention’s Mental Health Center.
1. Olson RP, editor. Mental health systems compared: Great Britain, Norway, Canada, and the United States. Illinois: Charles C Thomas Publisher; 2006.
2. World Health Organization (WHO). The world health report 2001. Mental health: New understanding, new hope. Geneva,Switzerland; 2001.
3. Phillips MR, Zhang JX, Shi QC, Song ZQ, Ding ZJ, Pang ST, et al. Prevalence, treatment, and associated disability of mental disorders in four provinces in China during 2001-05: an epidemiological survey. Lancet 2009; 373(9680): 2041-2053.
4. Institute of Medicine. Neurological, Psychiatric and Development Disorders: Meeting the Challenge in the Developing World. Washington, DC: National Academy Press; 2001.
5. Reavley NJ, Jorm AF. Recognition of mental disorders and beliefs about treatment and outcome: findings from an Australian National Survey of Mental Health Literacy and Stigma. Aust N Z J Psychiatry 2011; 45(11): 947-956.
6. Thompson A, Hunt C, Issakidis C. Why wait? Reasons for delay and prompts to seek help for mental health problems in an Australian clinical sample. Soc Psychiatry Psychiatr Epidemiol 2004; 39(10): 810-817.
7. Haller DM, Sanci LA, Sawyer SM, Patton GC. The identification of young people’s emotional distress: a study in primary care. Br J Gen Pract 2009; 59(560): 159-165.
8. Gulliver A, Griffiths KM, Christensen H. Perceived barriers and facilitators to mental health help-seeking in young people: a systematic review. BMC Psychiatry 2010; 10: 113.
9. Jorm AF, Korten AE, Jacomb PA, Christensen H, Rodgers B,Pollitt P. ‘’Mental health literacy’’: A survey of the public’s ability to recognise mental disorders and their beliefs about the effectiveness of treatment. Med J Aust 1997; 166(4):182-186.
10. Wang JY, He YL. Progress in mental health literacy. Journal of Neuroscience and Mental Health 2013; 13(1): 98-101. (in Chinese)
11. Angermeyer MC, Dietrich S. Public beliefs about and attitudes towards people with mental illness: a review of population studies. Acta Psychiatrica Scandinavica 2006; 113(3): 163-179.
12. Chinese Ministry of Health. Survey evaluation protocol of mental health work from the General Office of the Ministry of Health (MOHCDC[2010] Number 24).Beijing: Ministry of Health. Available from: http://www.gov.cn/gzdt/2010-03/08/content_1550552.htm. (accessed August 1, 2013) (in Chinese)
13. Chen HH, Phillips MR, Cheng H, Chen QQ, Chen XD, Fralick D, et al. Mental health law of the People’s Republic of China(English translation with annotations). Shanghai Archives of Psychiatry 2012; 24(6): 305-321.
14. Zhong BL, Chen HH, Xiao SY, Zhou L, Zhang JF, Xu HM. Reliability and validity of mental health knowledge questionnaire for middle school students. Chinese Journal of School Health 2011; 32(01): 49-50. (in Chinese)
15. Ministries of Health, Civil Affairs, Public Security, and All China Disabled Persons Federation. Mental Health Work Plan of China (2002-2010). Shanghai Archives of Psychiatry 2003; 15(2): 125-128.
16. Hu HY, Yan YZ, Chen LM, Pu WJ, Liao W, Li J. Knowledge about mental health and attitude to mental disorder in urban and rural residents in Guangzhou. Chinese Mental Health Journal 2012; 26(1): 30-35. (in Chinese)
17. Peng Y, Wang XL, Li PF, Liu K. Mental health literacy in Changsha, China. Shanghai Archives of Psychiatry 2011; 23(6):353-359.
18. Liang XP, Zhu XJ, Liu T, Zhang ZZ, Liang Y, Wang YJ. Crosssectional survey on awareness of mental health knowledge among communities in Xi’an. China Journal of Health Psychology 2011; 25(10): 1200-1202. (in Chinese)
19. Meng GR, Yao XW, Zhu ZQ, Zhang MY. A survey of knowledge about mental health in Shanghai: analysis of 2697 survey questionnaires. Shanghai Archives of Psychiatry 2002; 14(suppl): 56-57. (in Chinese)
20. Meng GR, Li XH, Yao XW, Zhu ZQ. Knowledge about mental health in a sample of 1783 people. Shanghai Archives of Psychiatry 2005; 17(suppl): 19-20. (in Chinese)
21. Schomerus G, Schwahn C, Holzinger A, Corrigan PW, Grabe HJ, Carta MG, et al. Evolution of public attitudes about mental illness: a systematic review and meta-analysis. Acta Psychiatrica Scandinavica 2012; 125(6): 440-452.
22. Coles ME, Coleman SL. Barriers to treatment seeking for anxiety disorders: initial data on the role of mental health literacy. Depress Anxiety 2010; 27(1): 63-71.
23. Li F, Xiao SY, Huang ZP, Shi JG, Cheng ZH, Luo WF, et al. Mental health literacy in three cities of China: A survey study. Chinese Mental Health Journal 2009; 23(12): 883-887. (in Chinese)
24. Petersen I, Lund C, Stein DJ. Optimizing mental health services in low-income and middle-income countries. Curr Opin Psychiatry 2011; 24(4): 318-323.
25. Deen TL, Bridges AJ. Depression literacy: rates and relation to perceived need and mental health service utilization in a rural American sample. Rural Remote Health 2011; 11(4):1803.
上海市居民精神卫生知识知晓度调查
王静夷1,何燕玲1*,蒋清1,蔡军1,王维玲1,曾庆枝1,缪菊明1,齐雪君1,陈建新1,卞茜1,蔡淳2,马宁2,朱紫青1,张明园1
1上海交通大学医学院附属精神卫生中心,上海市疾病预防控制精神卫生分中心 上海
2上海市卫生局疾控处 上海
背景: 近期中华人民共和国精神卫生法的实施是了解中国社区居民精神卫生知识知晓度基线数据的契机。目的了解上海市居民精神卫生知识和态度。方法来自上海市所有的19个区县1953名15岁及以上的常住居民完成了《精神卫生与心理保健知识问卷》及《案例》部分的调查。知识问卷满分20分,得分越高,表明对相关知识的了解程度越高。案例部分包括5个案例的描述,在每个案例后提出9个相关问题以评估受访者对这些精神障碍的知识和态度。结果精神卫生与心理保健知识问卷20个条目的正确回答率为26%~98%,平均72%。该问卷20个条目的内部一致性(α)为0.69,如果不纳入其中关于精神卫生健康促进的4个条目,α值则降至0.59。对一半的调查数据进行探索性因子分析,确定精神卫生与心理保健知识问卷20个条目的五因子模型,但用另一半数据进行验证性因子分析表明上述模型仅部分有效。案例相关知识调查发现,受访者对以下精神障碍的正确识别率分别为:躁狂症42%,抑郁症35%,阳性症状为主的精神分裂症30%,阴性症状为主的精神分裂症18%,焦虑症21%。工作压力太大(37.3%)、思想上的问题(30.0%)和受了打击(24.4%)被视为精神疾病的3个主要原因。找人做心理咨询(34.2%)和看精神科医生(33.3%)是建议求助的方法中2种最主要的方式。受教育程度愈高、愈年轻者对精神卫生知识的知晓率就愈高,对常见精神疾病的识别率也愈高。结论调查发现上海市居民对精神卫生与心理保健知识的知晓度有所提高。由于尚未充分评估精神卫生与心理保健知识问卷及案例部分问卷的信度和效度,所以本研究结果只能视为预初性的。需要进一步的工作,如首先从质和量两方面着手修订这些工具,才能将其用于评估精神卫生促进运动的有效性。
Background:The recent adoption of China’s new national mental health law provides a good opportunity to obtain baseline information about community mental health literacy in the country.mAim:Assess knowledge and attitudes about mental disorders among residents in Shanghai.Methods:A total of 1953 residents aged 15 or above selected from all 19 districts in Shanghai completed two self-report questionnaires – the Mental Health Knowledge Questionnaire (MHKQ) and the Case Assessment Questionnaire (CAQ). MHKQ total scores range from 0 to 20 (higher scores indicate better mental health literacy). The CAQ presents respondents with five case vignettes and possesses nine questions after each vignette measuring respondents’ knowledge and attitudes towards these mental illnesses.Results:Correct response rates for the 20 MHKQ items ranged from 26 to 98%, with a mean rate of 72%. The internal consistency (alpha) of the 20 items on the MHKQ was 0.69, but this decreased to 0.59 after removing four items about mental health promotion. A 5-factor model for the 20 items in the MHKQ was identified using exploratory factor analysis on one-half of the surveys, but the model was only partially validated in the confirmatory factor analysis using the second half of the surveys. On the CAQ, rates of correct recognition of mania, depression, schizophrenia with positive symptoms, schizophrenia with negative symptoms and anxiety were 42%, 35%, 30%, 19% and 21%, respectively. Work stress (37.3%), problems with thinking (30.0%) and negative life events (24.4%) were reported to be the three main causes of mental disorders. Seeing a counselor(34.2%) or a psychiatrist (33.3%) were the two most common suggestions for help-seeking. Higher education and younger age were related with better mental health literacy and higher rates of recognition of common mental disorders.Conclusions:Mental health literacy in Shanghai appears to be increasing, but the reliability and validity of the instruments used to assess mental health literacy (MHKQ and CAQ) have not been adequately assessed so this result must be considered preliminary. Further work, preferably including both qualitative and quantitative components, is needed to revise these instruments before they can be used to assess the effectiveness of mental health promotion campaigns.
10.3969/j.issn.1002-0829.2013.04.004
1Shanghai Mental Health Center, Shanghai Jiao Tong University School of Medicine, Shanghai, China
2Department of Disease Control and Prevention, Shanghai Municipal Health Bureau, Shanghai, China
*correspondence: heyl2001@163.com
(received: 2013-01-09; accepted: 2013-02-25)

Jingyi Wang graduated with a Bachelor’s degree in medicine from the Xiangya Medical School of Central-South University in 2010 and obtained a Master’s degree from the Shanghai Jiaotong University in 2013. Her Master’s thesis was on mental health literacy among community members. She is currently a PhD student at the University College London. Her research interests are public mental health and mental health services.
*通信作者:heyl2001@163.com
猜你喜欢
杂志排行
上海精神医学的其它文章
- Advances in genetic studies of substance abuse in China
- Prevalence of eating disorders in the general population:a systematic review
- Twelve-year retrospective analysis of outpatients with Attention-Deficit/Hyperactivity Disorder in Shanghai
- Effectiveness and safety of generic memantine hydrochloride manufactured in China in the treatment of moderate to severe Alzheimer’s disease: a multicenter, double-blind randomized controlled trial
- Should repetitive Transcranial Magnetic Stimulation (rTMS)be considered an effective adjunctive treatment for auditory hallucinations in patients with schizophrenia?
- A case of recurrent neuroleptic malignant syndrome