Clinical features and outcomes of patients with severe acute pancreatitis complicated with gangrenous cholecystitis
2013-06-01
Shanghai, China
Clinical features and outcomes of patients with severe acute pancreatitis complicated with gangrenous cholecystitis
Er-Zhen Chen, Jie Huang, Zhi-Wei Xu, Jian Fei, En-Qiang Mao and Sheng-Dao Zhang
Shanghai, China
BACKGROUND:The effects of gangrenous cholecystitis (GC) and consequent surgical interventions on the clinical outcomes and prognosis of patients with severe acute pancreatitis are not clear. The present study was to characterize the clinical outcomes of patients with severe acute pancreatitis complicated with GC.
METHODS:We retrospectively analyzed 253 consecutive patients hospitalized for acute pancreatitis in intensive care unit. Among them, 68 were diagnosed as having severe acute pancreatitis; 10 out of the 68 patients had GC. We compared these 10 patients with GC and 58 patients without GC. The indices analyzed included sepsis/septic shock, pancreatic encephalopathy, acute respiratory distress syndrome, acute renal failure, multiple organ dysfunction syndrome, and death.
RESULTS:Specif i c CT images of GC in patients with severe acute pancreatitis included enlarged and high-tensioned gallbladder, wall thickening, lumenal emphysema, discontinuous and/or irregular enhancement of mucosa, and pericholecystic effusion. The rates of severe sepsis/septic shock (70.0% vs 24.1%,P<0.01), pancreatic encephalopathy (50.0% vs 17.2%,P<0.05), acute respiratory distress syndrome (90.0% vs 41.4%,P<0.01), multiple organ dysfunction syndrome (70.0% vs 24.1%,P<0.01), acute renal failure (40.0% vs 27.6%,P<0.05), and death (40.0% vs 13.8%,P<0.05) were signif i cantly higher in patients with GC than in those without GC.
CONCLUSION:CT scans can help to identify early GC in patients with severe acute pancreatitis; early diagnosis and intervention for patients with GC can reduce morbidity and mortality.
(Hepatobiliary Pancreat Dis Int 2013;12:317-323)
severe acute pancreatitis; gangrenous cholecystitis; surgical intervention
Introduction
Acute pancreatitis (AP) is a common cause of acute abdominal pain, and the incidence of AP is increasing in China.[1]AP is pathologically characterized by pancreatic enzymatic autodigestion of pancreatic parenchyma and is so called sterile pancreatic inf l ammation. The underlying causes of AP are varied geographically.[1]In Chinese populations, the most common pre-existing condition is gallstone disease (60%-70%), followed by crapulence, alcoholism, and hyperlipidemia.[1]The clinical course and outcome of AP are also highly variable, the disease is self-limiting in most patients and requires supportive treatment only.[2]
Approximately 20% of patients with AP progress to hemorrhagic necrotizing pancreatitis or severe acute pancreatitis (SAP).[3]SAP is frequently associated with systemic and/or locoregional complications, such as acute respiratory distress syndrome (ARDS), systemic inf l ammatory response syndrome (SIRS), multiple organ dysfunction syndrome (MODS), disseminated intravascular coagulation (DIC), and peritoneal abscess formation from intestinal bacterial translocation.[3]SAP, therefore, is potentially life-threatening, with an overall mortality rate of 20%-60% despite aggressive interventions, such as hospitalization in the intensive care unit (ICU) and surgery.[4]The major determinants of mortality in SAP patients include the presenceof MODS, the extent of pancreatic necrosis, and the severity of infection and sepsis.[4]Early diagnosis and prognostic evaluation of SAP, including complications and comorbidities, are extremely important in reducing SAP-associated morbidity and mortality.[5]
Gangrenous cholecystitis (GC), or gallbladder necrosis caused by compromised blood circulation, is the most severe form of acute cholecystitis (AC).[6]The mortality of AC patients complicated with GC is 15%-50% higher than that of those without GC, and it is even higher in elderly, immunocompromised and diabetic patients.[6]Patients with acute acalculous cholecystitis (AAC), especially critically ill patients in the ICU, may develop GC, particularly when AAC is overlooked because of the absence of typical gallstone colic.[7]Although several medical imaging modalities, including ultrasonography,[8]computed tomography (CT),[9]magnetic resonance imaging (MRI)[10]and radioisotope scanning,[11]are useful in distinguishing GC from uncomplicated AC, the preoperative diagnosis of GC remains challenging. Because the optimal treatment of GC is not def i ned, early cholecystectomy, usually performed laparoscopically, has been recommended to minimize the morbidity and mortality.[12]
Although GC is present in 30% of patients undergoing emergency cholecystectomy, it is rarely associated with SAP.[6]As GC can independently increase the risk of sepsis and multiple organ failure, GC likely worsens the prognosis of patients with SAP. To highlight the importance of early detection and treatment of GC in patients with SAP, we have retrospectively assessed the effects of GC and its surgical interventions on the clinical outcomes and prognosis of patients with SAP.
Methods
Patient enrollment
We retrospectively evaluated 253 consecutive patients with AP who were hospitalized in the surgical/ emergency ICU of Ruijin Hospital, Shanghai, China, between January 2008 and December 2010. SAP was diagnosed based on the Atlanta Symposium classif i cation system.[13]Inclusion criteria are as follows: (a) patients had been referred to and hospitalized in the ICU within 72 hours of the onset of abdominal pain; (b) patients received nonsurgical treatment in the ICU for at least 7 days; and (c) patients underwent a laparotomy during ICU stay. The cohort comprised both males and females who were 18-70 years old. Exclusive criteria were as follows: patients with chronic renal insuff i ciency and had a history of pacemaker implantation and women with a history of pregnancy. The patients were divided into GC and non-GC groups, based on the results of intraoperative pathology and postsurgical histology. The study protocol was approved by the Institutional Review Board of Ruijin Hospital, and most of the patients provided written informed consent prior to enrollment.
ICU treatment and evaluation
All patients had been hospitalized in the emergency/ surgical ICU and treated by critical care physicians and surgeons. Rehydration fl uids included normal saline, lactated Ringer's solution, plasma, and 6% hydroxyethyl starch at a crystal/colloid ratio of 2:1. Basic medical treatments included somatostatin infusion, inhibition of gastrointestinal secretion, and prophylactic antibiotics. EnteralRadix et Rhizoma Rhei(a Chinese herb) extracts and Glauber's salt (a Chinese medicinal mineral, consisting mainly of sodium sulfate, sodium chloride, and magnesium sulfur) were also administered as described.[14,15]Patients with jaundice on admission underwent endoscopic retrograde cholangiopancreatography (ERCP) and/or endoscopic nasal bile drainage. Vital signs, including body temperature, heart rate, and blood pressure, were measured daily for at least one week. Conventional hematology, arterial blood gas, electrolytes, and Glasgow's score were analyzed daily at 6:00 am. The volume of rehydration fl uid and APACHE II score were recorded daily. All patients underwent abdominal CT scan on admission and every week thereafter. Five (8.6%) of the 58 non-GC, but none of the 10 GC patients underwent preoperative ERCP because of suspected gallstone obstruction.
Surgical treatment
Intensive care treatments of infection were started within 48 hours after the diagnosis of infected pancreatic necrosis based on CT scan fi ndings. Laparotomy was performed only in 68 patients with uncontrollable severe sepsis/septic shock. Operative procedures included debridement of pancreatic and peripancreatic necrotic tissues, along with external drainage of infected extrapancreatic and pancreatic necroses (n=68), cholecystectomy (n=4) or cholecystostomy (n=64), and jejunostomy for nutritional support (n=68). Bile samples were collected at the initial surgery for bacterial culture.
Def i nitions of clinical entities
GC diagnosis is based on intraoperative gross pathology and postsurgical histology. GC has been pathologically def i ned as inf l ammatory changes,including edema, vascular congestion and leukocyte inf i ltration, plus (a) intramural hemorrhage, (b) gallbladder necrosis, or (c) microabscess. Pancreatic encephalopathy is characterized by abnormalities of mental status, including spatial disorientation, somnolence, agitation, delusion and hallucination, which were caused by SAP. ARDS is def i ned as progressive radiographic inf i ltrates into both lungs and a PaO2/FiO2ratio <200 without cardiac failure.[16]Acute renal failure (ARF)[17]sepsis/septic shock[18]and MODS[19]are as described previously. Timing of surgical intervention is def i ned as the time interval between the onset of abdominal pain and fi rst laparotomy.
Predictive parameters and outcome measures
Tested parameters included body temperature, white blood cell count (WBC), gallbladder images of CT scan, liver function, Balthazar CT severity index (CTSI)[20]and APACHE II score[21]within 72 hours after admission. Primary outcome measures included severe sepsis/septic shock, pancreatic encephalopathy, Glasgow coma score (GCS), ARDS, ARF, and MODS at the time of fi rst operation, and in-hospital mortality. Secondary outcome measures included frequency, timing and duration of surgical interventions, bacterial positivity of bile culture, and length of ICU stay.
Statistical analysis
All quantitative data were expressed as mean±SD and compared using two-tailed Student'sttest. All qualitative data were expressed as number (%) and analyzed using Fisher's exact test. APvalue less than 0.05 was considered statistically signif i cant.
Results
Baseline characteristics
In the 68 SAP patients eligible for the study, 10 (14.7%) patients were with GC and 58 (85.3%) patients without GC (Fig. 1). The two groups of patients had comparable baseline characteristics, including age, sex, body temperature, WBC count, liver function, CTSI, APACHE II score, and underlying comorbidities (allP>0.05; Table 1). Gallstones were the most common underlying condition, with an overall incidence rate of 58.8%, or an incidence rate of 70.0% and 56.9% for GC (Table 2) and non-GC groups respectively. Gallstones were followed by hyperlipidemia with an incidence rate of 33.8%. Alcoholism was associated with SAP in 3.4% of the patients, with 4.4% of the patients diagnosed with idiopathic SAP. Endoscopic ERCP did not result in either clinical improvement or additional complications.
Manifestations of GC on CT scan
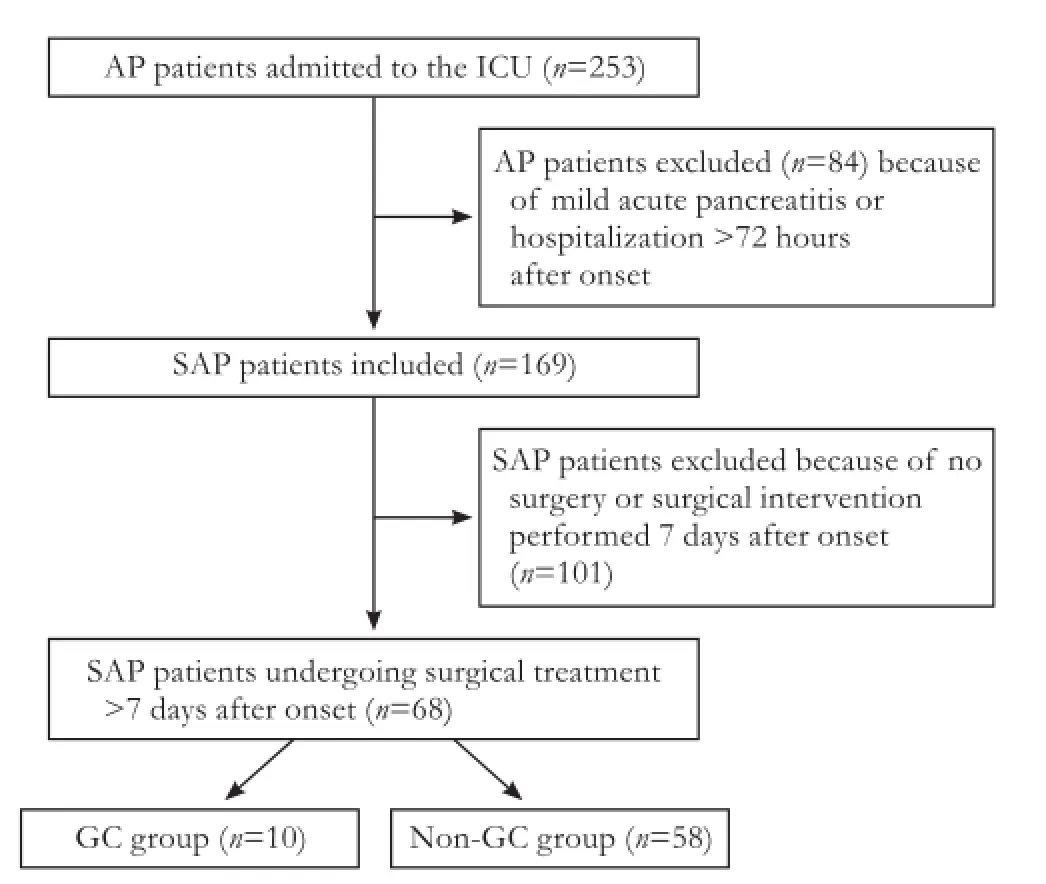
Fig. 1.Treatment algorithm fl ow chart of patients with SAP. AP: acute pancreatitis; SAP: severe acute pancreatitis; ICU: intensive care unit; GC: gangrenous cholecystitis.

Table 1.Baseline characteristics of SAP patients admitted to the ICU (n=68)
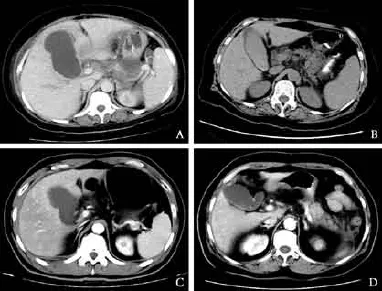
Fig. 2.Upper abdominal contrast-enhanced CT images of SAP patients with and without gangrenous cholecystitis (GC).A-C: CT images in SAP patients with GC, showing (A) gallbladder distention with an irregular wall, (B) the presence of biliary sludge and pericholecystic effusion, and (C) partially absent mucosal enhancement. (D) CT image in a patient with SAP but without GC enhancement, showing a non-distended gallbladder, of normal size and with a regular wall.
Although CT scan identif i ed some nonspecif i c radiological signs of GC, enlarged and high-tension gallbladder (P=0.01), wall thickening (P=0.02), lumenal emphysema (P=0.02), discontinuous and/or irregular enhancement of mucosa (P=0.09), and pericholecystic effusion (P=0.02) were signif i cantly more frequent in patients complicated with GC than in those without GC (Table 2). These manifestations became more evident on contrast-enhanced CT scans (Fig. 2).
Primary and secondary outcome measurements
As shown in Table 3, the rates of severe sepsis/septic shock, pancreatic encephalopathy, ARDS and MODS were signif i cantly higher in patients complicated with GC than in those without GC (allP<0.01). The rates of ARF and death were higher in patients complicated with GC than in those without GC, but these differences were not statistically signif i cant. Nine of SAP patients died of refractory septic shock and three died of massive intraperitoneal bleeding.
The timing of surgical intervention differed signif icantly in GC and non-GC patients (P<0.05). The bile of GC patients at initial laparotomies was more likely to be positive for bacteria than that of non-GC patients (P<0.01), and GC patients required a signif i cantly longer stay in the ICU than non-GC patients (P<0.01).
Surgical outcomes in SAP patients with GC
In addition to undergoing pancreatic and peripancreatic necrosectomy, 2 out of the 10 SAP patientswith GC underwent laparotomic cholecystectomy and 8 underwent cholecystostomy; whereas, of the 58 SAP patients without GC, 56 underwent cholecystostomy and 2 underwent cholecystectomy. The primary indication for cholecystostomy in SAP patients was a serious underlying systemic condition or high risk of bleeding in dissecting the gallbladder. The two groups of patients did not show signif i cant difference in the length of ICU stay and the rates of death, reoperation, septic shock, and encephalopathy. One of the two patients who had undergone cholecystectomy and laparotomy underwent a second laparotomy due to persistent septic shock following the fi rst operation, although the resection of the gangrenous gallbladder resulted in an immediate improvement in septic shock.
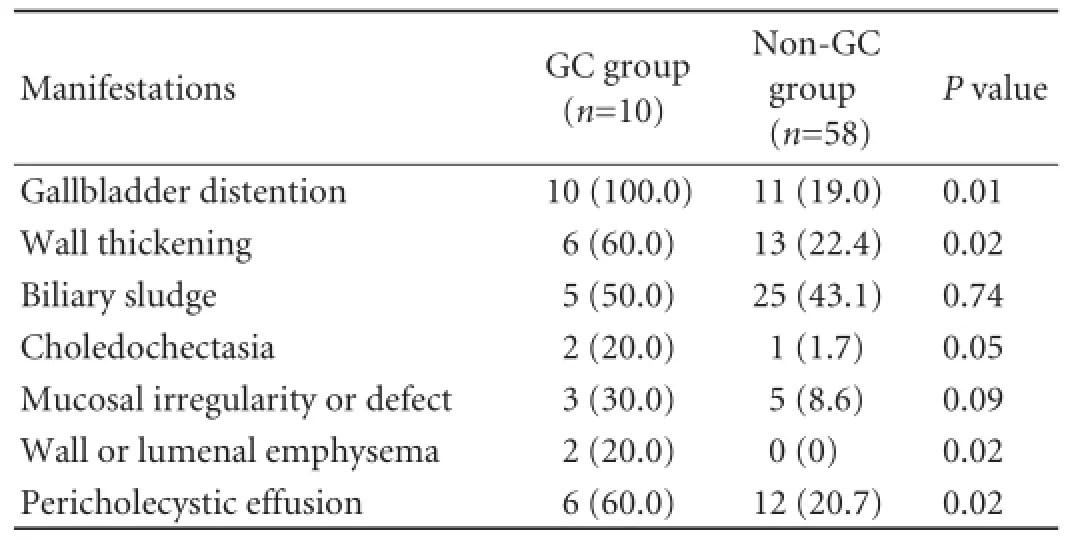
Table 2.Incidence of gallbladder manifestations on contrastenhanced CT scan in SAP patients admitted to the ICU (n, %)
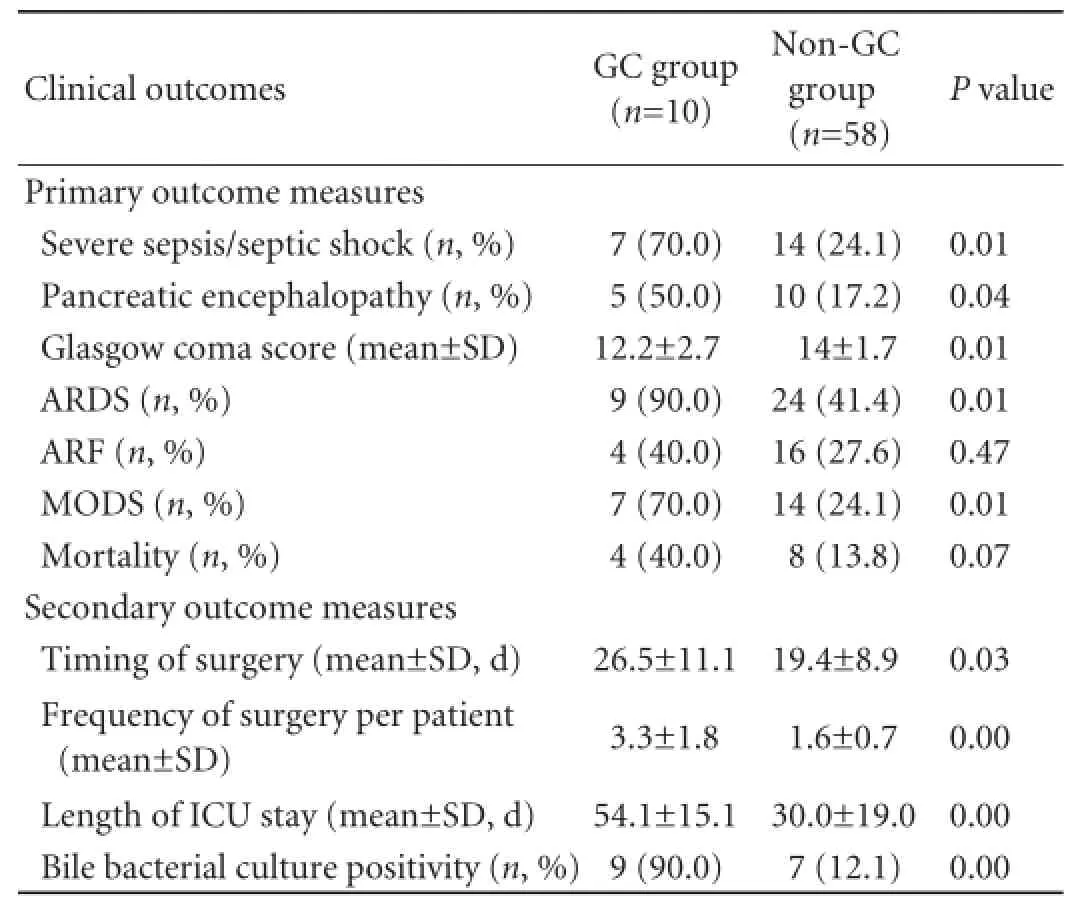
Table 3.Clinical outcomes of SAP patients admitted to the ICU
Discussion
GC is a rare complication in patients with AP or SAP. Patients with AC or cholecystolithiasis alone are less likely to have AP or SAP in the absence of secondary choledocholithiasis or ascending cholangitis. However, AC may progress to GC in patients with SAP.[23]The comorbidity of GC and SAP manifests more severe and has a higher mortality compared with SAP only. The pathogenesis and pathophysiology underlying the comorbidity of GC and SAP remain unknown. In general, the possible mechanism of GC in SAP patients is consistent with that of GC in AC patients: gallbladder ischemia plus biliary obstruction and inf l ammation. In our study, gallstone pancreatitis was observed in 58.8% of SAP patients with GC, indicating that GC in SAP patients resulted mainly from gallstones. Obstruction of the common bile duct (CBD) and/or cholecystic duct along with cholestasis not only results in injuries to the biliary mucosa but also aggravates AP-associated systemic inf l ammation.[6,26]Cholecystic duct obstruction and alterations in bile chemistry are apparently required for the progression of gallbladder inf l ammation. Secondary contamination with pyogenic or anaerobic organisms may exacerbate hyperemia and edema of the gallbladder, resulting in pyogenic infection or gangrene. This is consistent with the higher positive rate of bile culture in the GC group. Moreover, the presence of gallstones in the cholecystic duct can compress the cholecystic veins and compromise venous drainage. Thus, the presence of gallstones is regarded as an independent risk factor for GC in addition to AP. AC is also associated with a high incidence of gangrene (59%-63%).[7]This is due primarily to the compromise of the cholecystic artery. As a terminal blood vessel, the cholecystic artery insuff i ciency leads to ischemia and hypoxemia of the gallbladder. The later enhances sepsis or even septic shock.[27,28]
Prolonged conservative treatment in patients with SAP may increase the risk of GC, especially in longtime hospitalized patients. In our study, 10 patients with GC were not diagnosed preoperatively. We found that GC was present in 14.7% (10/68) of SAP patients hospitalized in the ICU. The overall rate of GC in our patients was lower than that (30%) reported in patients undergoing emergency cholecystectomy due to AC or cholecystolithiasis.[6]The incidence of GC associated with SAP may be underestimated because of the concentrated conservative treatment of SAP patients. Early diagnosis of GC leads to early surgical intervention.
The characteristics of GC in patients with AC may be adopted as screening criteria for GC in patients with SAP. Risk factors for GC in patients with AC include male gender, age>50 years, Mannheim peritonitis index (a scale predicting the prognosis of patients with abdominal sepsis) ≥29, a medical history of cardiovascular disease or diabetes mellitus, WBC count>15×109/mL, and elevated ALT/AST.[6,25,29]Nguyen and colleagues developed a predictive equation for detecting GC in patients with AC, they put diabetes mellitus, WBC count, ALT, AST and pericholecystic fl uid in this equation, if the cut off line is 0.724, the specif i city is 93% and sensitivity is 83%.[30]
In patients with SAP, however, these indicators may be indistinguishable from systemic inf l ammation, sepsis, and organ dysfunction due to SAP. We found that only age is a criterion for GC in patients with SAP. In critically ill patients with SAP, the clinical manifestations of GC are usually concealed by SAP. It is diff i cult in clinical practice to distinguish between the patients with SAP only and those with SAP and GC. We also could not identify specif i c factors for detecting GC in patients with SAP, as our GC and non-GC groups showed comparable clinical features, including APACHE II score and CTSI; however, the number of GC patients was relatively small (n=10). GC may be present in patients with gallstone pancreatitis and non-biliary pancreatitis hospitalized in the ICU. AAC is common in critical ill medical and surgical patients and may progress to GC.[7]
In current practice, the preoperative diagnosis of GC is extremely diff i cult in patients with SAP, even in AC patients, because the clinical and laboratory presentations of GC are nonspecif i c.[6]However, clinical practice and our results indicate that CT scan is more useful for early diagnosis of GC. The most striking CT presentations we observed included enlarged and hightension gallbladder, discontinuous and/or irregular enhancement of the mucosa, and pericholecystic effusion. The presence of gallstones in the cholecystic neck or duct is also suggestive of GC. Thus, the presence of one or more of these indicators on CT scans should be regarded as GC in SAP patients. Although these diagnostic criteria are obscure and less specif i c, they are clinically useful until better criteria are developed. The sensitivity and positive predictive value of discontinuous and/or irregular mucosal enhancement in the diagnosis of GC were 30.3% and 94.4%, respectively.[31]Moreover, it was reported that signif i cant gallbladder distention, intra-lumenal or wall gas, irregular wall, lack of mural enhancement, and pericholecystic fl uid on CT were specif i cally characteristic of GC, with an overall accuracy of 86.7%,[9]especially under infectious circumstances. We also found that GC occurred more often in SAP patients with infectious bile than those without.Unfortunately, these obscure and less specif i c features of GC are rarely recognized preoperatively due to unawareness of GC in SAP patients.
In addition to CT, which has a specif i city of >90% in the identif i cation of GC,[9]several radiological and nonradiological imaging modalities have been reported to play a paramount role in predicting and/or identifying GC and SAP, such as ultrasonography,[8]MRI and biliary scintigraphy. Natural orif i ce transluminal endoscopy may be promising because it is a minimally invasive diagnostic tool to identify intra-abdominal pathology such as GC.[32]
Both APACHE II and CTSI are comparable in GC and non-GC patients at baseline. Although GC does not worsen the intrinsic severity of SAP, lack of recognition of GC can further complicate the clinical course and result in a worse clinical outcome in SAP patients. Once GC occurs, especially when complicated by infected pancreatic necrosis, it can lead to organ dysfunction/failure and systemic infection-associated comorbidities occur more frequently in SAP patients, with these patients being more likely to undergo surgical intervention and require a longer stay in the ICU.
The timing of surgical intervention for SAP itself remains unclear, as no single valid clinical trial has shown that early laparotomy with debridement (<72 hours) results in better outcomes than late surgery (>12 days following the onset of AP).[33]Surgery is normally postponed at least 4 weeks for patients presenting with infected necrosis, or with sterile necrosis but showing clinical deterioration, despite receiving intensive medical care. However, several randomized studies have reported that, compared with open necrosectomy, a minimally invasive step-up approach reduces the risks of major complications and death among patients with necrotizing pancreatitis with complicating infected necrosis.[34-36]In SAP patients with GC, although immediate surgical intervention has not been proved to be benef i cial, cholecystectomy should be performed immediately to reduce GC-associated morbidity and mortality. In our study, only two patients underwent cholecystectomy because of lack of correct recognition. Our results suggest that untreated gallbladder and/or biliary tract disorders deteriorate the progression of GC and SAP. If radiologic results suggest potential gallbladder gangrene, surgical intervention should be considered, despite the stable pancreatic and peripancreatic lesions. Cholecystectomy is preferred to cholecystostomy, which can be performed synchronously or asynchronously with pancreatic debridement. Due to the complexity of these conditions, open laparotomy rather than laparoscopy should be performed, although the latter may be indicated in patients with uncomplicated GC.[12]In surgical practice, however, complete resection of a gangrenous and necrotic gallbladder is challenging. Percutaneous cholecystostomy may be a palliative treatment option for critically ill patients, such as those with SAP, but may be less effective in patients complicated with biliary obstruction and failure of continuous drainage of the common bile duct. In addition, percutaneous cholecystostomy is contraindicated for patients complicated with intraperitoneal sepsis. It may be cautiously attempted in the palliative treatment of SAP. Our results, however, suggest that patients undergoing cholecystostomy frequently require a second laparotomy and show less satisfactory outcomes. Therefore, cholecystectomy is preferred to cholecystostomy in SAP patients if their general condition permits.
In conclusion, GC is a rare complication in SAP patients, although early diagnosis and intervention for GC can reduce the morbidity and mortality of patients. CT scans are helpful in the early diagnosis and timely treatment of GC, although the onset of GC in SAP patients is insidious. Surgical interventions, especially cholecystectomy, provide better clinical outcomes in SAP patients with associated GC. Early diagnosis and treatment improve the prognosis of patients.
Contributors:CEZ and HJ contributed equally to this work. CEZ and HJ proposed the study, drafted the paper, collected the data and analyzed the data. All authors contributed to the design and interpretation of the study and to further drafts. MEQ is the guarantor.
Funding:This study was supported by a grant from Science and Technology Commission of Shanghai Municipality (12411950500).
Ethical approval:The study protocol was approved by the Institutional Review Board at Ruijin Hospital, Shanghai, China.
Competing interest:No benef i ts in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
1 Bai Y, Liu Y, Jia L, Jiang H, Ji M, Lv N, et al. Severe acute pancreatitis in China: etiology and mortality in 1976 patients. Pancreas 2007;35:232-237.
2 Beger HG, Rau BM. Severe acute pancreatitis: Clinical course and management. World J Gastroenterol 2007;13:5043-5051.
3 Al Mof l eh IA. Severe acute pancreatitis: pathogenetic aspects and prognostic factors. World J Gastroenterol 2008;14:675-684.
4 Milian JW, Portugal SJ, Laynez ChR, Rodríguez AC, Targarona J, Barreda CL. Necrotic acute pancreatitis in the intensive care unit: a comparison between conservative and surgical medical treatment. Rev Gastroenterol Peru 2010;30:195-200.
5 Swaroop VS, Chari ST, Clain JE. Severe acute pancreatitis.JAMA 2004;291:2865-2868.
6 Merriam LT, Kanaan SA, Dawes LG, Angelos P, Prystowsky JB, Rege RV, et al. Gangrenous cholecystitis: analysis of risk factors and experience with laparoscopic cholecystectomy. Surgery 1999;126:680-686.
7 Shapiro MJ, Luchtefeld WB, Kurzweil S, Kaminski DL, Durham RM, Mazuski JE. Acute acalculous cholecystitis in the critically ill. Am Surg 1994;60:335-339.
8 Maeda M, Ishida Y, Okamoto K. Ultrasound diagnosis of gangrenous cholecystitis due to gallbladder torsion. Rofo 1994;161:465-467.
9 Bennett GL, Rusinek H, Lisi V, Israel GM, Krinsky GA, Slywotzky CM, et al. CT fi ndings in acute gangrenous cholecystitis. AJR Am J Roentgenol 2002;178:275-281.
10 Watanabe Y, Nagayama M, Okumura A, Amoh Y, Katsube T, Suga T, et al. MR imaging of acute biliary disorders. Radiographics 2007;27:477-495.
11 Hayashi AK, Soudry G, Dibos PE. Rim sign. Radionuclide imaging in a patient with acute gangrenous cholecystitis and cholelithiasis after nonspecif i c abdominal ultrasonography. Clin Nucl Med 1997;22:388-389.
12 Habib FA, Kolachalam RB, Khilnani R, Preventza O, Mittal VK. Role of laparoscopic cholecystectomy in the management of gangrenous cholecystitis. Am J Surg 2001;181:71-75.
13 Bradley EL 3rd. A clinically based classif i cation system for acute pancreatitis. Summary of the International Symposium on Acute Pancreatitis, Atlanta, Ga, September 11 through 13, 1992. Arch Surg 1993;128:586-590.
14 Zhao YQ, Liu XH, Ito T, Qian JM. Protective effects of rhubarb on experimental severe acute pancreatitis. World J Gastroenterol 2004;10:1005-1009.
15 Zhang MJ, Zhang GL, Yuan WB, Ni J, Huang LF. Treatment of abdominal compartment syndrome in severe acute pancreatitis patients with traditional Chinese medicine. World J Gastroenterol 2008;14:3574-3578.
16 Bernard GR, Artigas A, Brigham KL, Carlet J, Falke K, Hudson L, et al. The American-European Consensus Conference on ARDS. Def i nitions, mechanisms, relevant outcomes, and clinical trial coordination. Am J Respir Crit Care Med 1994;149:818-824.
17 Bellomo R, Ronco C, Kellum JA, Mehta RL, Palevsky P; Acute Dialysis Quality Initiative workgroup. Acute renal failure-def i nition, outcome measures, animal models, fl uid therapy and information technology needs: the Second International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group. Crit Care 2004;8:R204-212.
18 Levy MM, Fink MP, Marshall JC, Abraham E, Angus D, Cook D, et al. 2001 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Def i nitions Conference. Crit Care Med 2003;31:1250-1256.
19 Deitch EA. Multiple organ failure. Pathophysiology and potential future therapy. Ann Surg 1992;216:117-134.
20 Balthazar EJ, Ranson JH, Naidich DP, Megibow AJ, Caccavale R, Cooper MM. Acute pancreatitis: prognostic value of CT. Radiology 1985;156:767-772.
21 Papachristou GI, Muddana V, Yadav D, O'Connell M, Sanders MK, Slivka A, et al. Comparison of BISAP, Ranson's, APACHE-II, and CTSI scores in predicting organ failure, complications, and mortality in acute pancreatitis. Am J Gastroenterol 2010;105:435-442.
22 Itah R, Bruck R, Santo M, Skornick Y, Avital S. Gangrenous cholecystitis-a rare complication of ERCP. Endoscopy 2007; 39:E223-224.
23 Attasaranya S, Fogel EL, Lehman GA. Choledocholithiasis, ascending cholangitis, and gallstone pancreatitis. Med Clin North Am 2008;92:925-960.
24 Sanchez-Ubeda R, Rousselot LM, Giannelli S. The signif i cance of pancreatitis accompanying acute cholecystitis. Ann Surg 1956;144:44-50.
25 Fagan SP, Awad SS, Rahwan K, Hira K, Aoki N, Itani KM, et al. Prognostic factors for the development of gangrenous cholecystitis. Am J Surg 2003;186:481-485.
26 Sharp KW. Acute cholecystitis. Surg Clin North Am 1988;68: 269-279.
27 Kalliafas S, Ziegler DW, Flancbaum L, Choban PS. Acute acalculous cholecystitis: incidence, risk factors, diagnosis, and outcome. Am Surg 1998;64:471-475.
28 Kusske AM, Rongione AJ, Reber HA. Cytokines and acute pancreatitis. Gastroenterology 1996;110:639-642.
29 Aydin C, Altaca G, Berber I, Tekin K, Kara M, Titiz I. Prognostic parameters for the prediction of acute gangrenous cholecystitis. J Hepatobiliary Pancreat Surg 2006;13:155-159.
30 Nguyen L, Fagan SP, Lee TC, Aoki N, Itani KM, Berger DH, et al. Use of a predictive equation for diagnosis of acute gangrenous cholecystitis. Am J Surg 2004;188:463-466.
31 Singh AK, Sagar P. Gangrenous cholecystitis: prediction with CT imaging. Abdom Imaging 2005;30:218-221.
32 Onders RP, McGee MF, Marks J, Chak A, Rosen MJ, Ignagni A, et al. Natural orif i ce transluminal endoscopic surgery (NOTES) as a diagnostic tool in the intensive care unit. Surg Endosc 2007;21:681-683.
33 Besselink MG, Verwer TJ, Schoenmaeckers EJ, Buskens E, Ridwan BU, Visser MR, et al. Timing of surgical intervention in necrotizing pancreatitis. Arch Surg 2007;142:1194-1201.
34 van Santvoort HC, Besselink MG, Bakker OJ, Hofker HS, Boermeester MA, Dejong CH, et al. A step-up approach or open necrosectomy for necrotizing pancreatitis. N Engl J Med 2010;362:1491-1502.
35 Bakker OJ, van Santvoort HC, van Brunschot S, Geskus RB, Besselink MG, Bollen TL, et al. Endoscopic transgastric vs surgical necrosectomy for infected necrotizing pancreatitis: a randomized trial. JAMA 2012;307:1053-1061.
36 Alsfasser G, Schwandner F, Pertschy A, Hauenstein K, Foitzik T, Klar E. Treatment of necrotizing pancreatitis: redef i ning the role of surgery. World J Surg 2012;36:1142-1147.
Received February 14, 2012
Accepted after revision November 1, 2012
AuthorAff i liations:Emergency Intensive Care Unit (Chen EZ), and Surgical Intensive Care Unit (Huang J, Xu ZW, Fei J, Mao EQ and Zhang SD), Ruijin Hospital, School of Medicine, Shanghai Jiaotong University, Shanghai 200025, China
En-Qiang Mao, MD, Surgical Intensive Care Unit, Ruijin Hospital, School of Medicine, Shanghai Jiaotong University, 197 Ruijin Second Road, Shanghai 200025, China (Tel: 86-21-64370045; Fax: 86-21-64370045ext666066; Email: maoeq@yeah.net)
© 2013, Hepatobiliary Pancreat Dis Int. All rights reserved.
10.1016/S1499-3872(13)60050-8
杂志排行
Hepatobiliary & Pancreatic Diseases International的其它文章
- Surgical treatment of hepatocellular carcinoma with inferior vena cava tumor thrombus:a new classification for surgical guidance
- Pancreatic duct disruption and nonoperative management: the SEALANTS approach
- Pancreatic Castleman disease treated with laparoscopic distal pancreatectomy
- Inferior vena cava obstruction and collateral circulation as unusual manifestations of hepatobiliary cystadenocarcinoma
- Double-blind randomized sham controlled trial of intraperitoneal bupivacaine during emergency laparoscopic cholecystectomy
- Propofol inhibits the adhesion of hepatocellular carcinoma cells by upregulating microRNA-199a and downregulating MMP-9 expression