Outcomes of early physiotherapy in patients with cerebral aneurysms treated by surgical clipping or endovascular embolization☆●
2012-01-04ArzuGucluGunduzSevilBilginNezireseHakanOruckaptan
Arzu Guclu-Gunduz, Sevil Bilgin, Nezire Köse, Hakan Oruckaptan
1 Department of Physiotherapy and Rehabilitation, Faculty of Health Sciences, Gazi University, Ankara, Turkey
2 Department of Physiotherapy and Rehabilitation, Faculty of Health Sciences, Hacettepe University, Ankara, Turkey
3 Department of Neurosurgery, Faculty of Medicine, Hacettepe University, Ankara, Turkey
Outcomes of early physiotherapy in patients with cerebral aneurysms treated by surgical clipping or endovascular embolization☆●
Arzu Guclu-Gunduz1, Sevil Bilgin2, Nezire Köse2, Hakan Oruckaptan3
1Department of Physiotherapy and Rehabilitation, Faculty of Health Sciences, Gazi University, Ankara, Turkey
2Department of Physiotherapy and Rehabilitation, Faculty of Health Sciences, Hacettepe University, Ankara, Turkey
3 Department of Neurosurgery, Faculty of Medicine, Hacettepe University, Ankara, Turkey
Early physiotherapy was given to 124 patients with ruptured or unruptured cerebral aneurysms who were treated by surgical clipping or endovascular embolization. Patients were divided into four groups according to their Hunt and Hess grade at admission and aneurysm treatment modality:Group 1, Hunt and Hess grade ≤ II and surgical clipping; Group 2, Hunt and Hess grade ≤ II and endovascular embolization; Group 3, Hunt and Hess grade ≥ III and surgical clipping; Group 4, Hunt and Hess grade ≥ III and endovascular embolization. Level of consciousness was evaluated using the Glasgow Coma Scale, functional status using the Glasgow Outcome Scale, level of the mobility using the Mobility Scale for acute stroke patients, and independence in activities of daily living using the Barthel Index. After early physiotherapy, the level of consciousness and functional status improved significantly in Groups 1, 3, and 4; mobility improved significantly in all groups; and independence in activities of daily living improved significantly in Groups 1 and 3. At discharge, Groups 1 and 2 had better functional status than Groups 3 and 4. Level of consciousness, functional status, mobility and independence in activities of daily living improved after early physiotherapy. These findings suggest that early physiotherapy improved the prognosis of patients with cerebral aneurysms who were treated by surgical clipping or endovascular embolization. Patients with a worse clinical status at presentation had a poorer functional status at discharge. The outcome of physiotherapy was not affected by whether surgical clipping or endovascular embolization was chosen for treatment of the aneurysm.
cerebral aneurysm; Hunt and Hess grade; Glasgow Coma Scale; Glasgow Outcome Scale; functional status; surgical clipping; endovascular treatment; physiotherapy; neural regeneration
Research Highlights
(1) Patients with cerebral aneurysms who underwent surgical clipping or endovascular embolization and early physiotherapy were grouped according to their Hunt and Hess grade at admission.
(2) Level of consciousness, functional status, mobility and independence in activities of daily living improved after early physiotherapy.
(3) Patients with a worse clinical status at admission had a poorer functional status at discharge.
Abbreviations
GCS, Glasgow Coma Scale; GOS, Glasgow Outcome Scale; MSAS, Mobility Scale for Acute Stroke patients; BI, Barthel Index
INTRODUCTION
A cerebral aneurysm is an abnormal bulging outward of one of the arteries in the brain. Cerebral aneurysms are often discovered after rupture, which causes subarachnoid, or rarely parenchymal, hemorrhage[1]. Unruptured intracranial aneurysms are frequently diagnosed incidentally in patients who undergo evaluation for various complaints such as mild headache or minor head trauma, or who undergo central nervous system evaluation for other reasons[2-4]. A cerebral aneurysm can cause motor and cognitive impairments as a result of subarachnoid hemorrhage, mass effects or complications of treatment. These impairments reduce quality of life[5-6]. Clinical experience and observation suggest that early physiotherapy might improve functional outcomes. It has been reported that early physiotherapy improves outcomes in patients with ruptured and especially unruptured aneurysms[6-9]. The aim of this study was to analyze outcomes in patients with Hunt and Hess grades of ≤ II and ≥ III who received early physiotherapy after surgical clipping or endovascular embolization of a cerebral aneurysm.
RESULTS
Quantitative analysis of subjects
A total of 149 patients with cerebral aneurysms received early physiotherapy, of which 101 (67.8%) underwent surgical clipping and 48 (32.2%) underwent endovascular embolization. The aneurysm had ruptured causing subarachnoid hemorrhage in 110 patients (73.8%), and 39 patients (26.2%) were treated for unruptured aneurysms. Twenty-five patients (16.9%) died during hospitalization, and the remaining 124 patients were included in this study. Among patients with a Hunt and Hess grade of ≤ II, 51 (41.1%) underwent surgical clipping (Group 1) and 18 (14.5%) underwent endovascular embolization (Group 2). Among patients with a Hunt and Hess grade of ≥ III, 29 (23.4%) underwent surgical clipping (Group 3) and 26 (21.0%) underwent endovascular embolization (Group 4) (Table 1).
总之,从职业这个方面去讨论自主性,不仅将社工职业放入整体的社会大环境中思考,思考其当下的定位,思考日后的发展,而且也能最大限度地揭示出作为职业从业人员——一线社工自身的能动性。同时,这两个方面也不是孤立的,而是相互影响且相互改变着,即职业定位和未来发展影响一线社工在社工职业发展上的规划,一线社工对于自身职业的定位也塑造着社工职业的现在和未来。
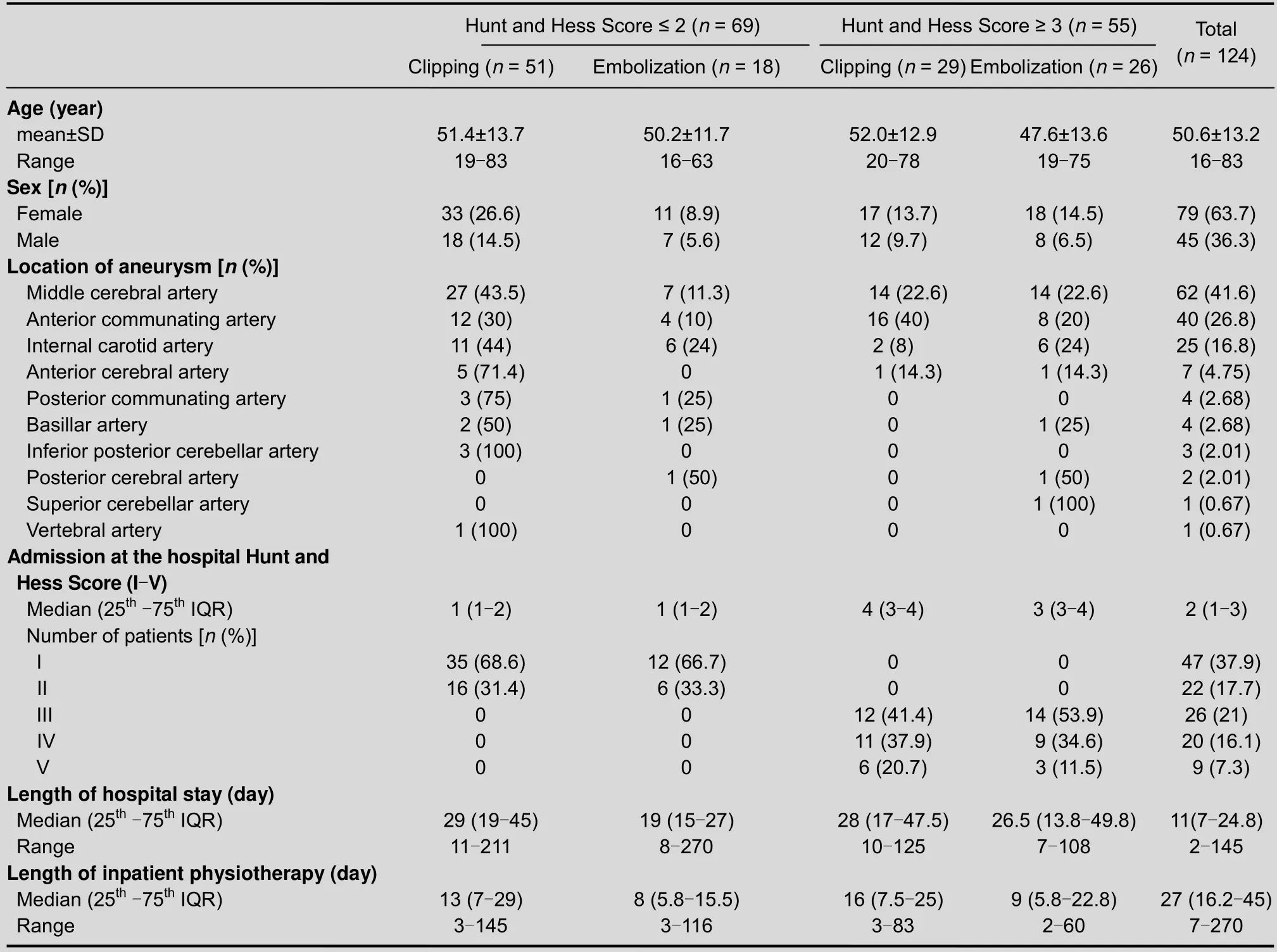
Table 1 Patient characteristics
Demographic characteristics of patients
The demographic characteristics of patients are shown in Table 1. The study included 79 females and 45 males with a mean age of 51 years (range 16-83 years).
There were no significant differences in gender distribution (P> 0.05) or age (P> 0.05) among the four groups. Twenty-three patients had multiple aneurysms. Aneurysms were mainly located in the middle cerebral artery (41.6%), anterior commutating artery (26.8%) and internal carotid artery (16.8%). There were no significant differences in length of hospital stay or length of physiotherapy among the study groups (P> 0.05).
Changes in Glasgow Coma Scale (GCS), Glasgow Outcome Scale (GOS), Mobility Scale for Acute Stroke patients (MSAS) and Barthel Index (BI) scores after early physiotherapy
The GCS and GOS scores had improved significantly at the time of discharge in Groups 1, 3 and 4 (P< 0.05) but not in Group 2 (P> 0.05). The MSAS score improved significantly in all groups after early physiotherapy (P<0.05). The BI score improved significantly in Groups 1 and 3 only (P< 0.05). The GOS, MSAS and BI scores showed that all patients were severely disabled at the time of discharge (Table 2; Figure 1).

Table 2 GCS, GOS, MSAS and BI scores before and after early physiotherapy
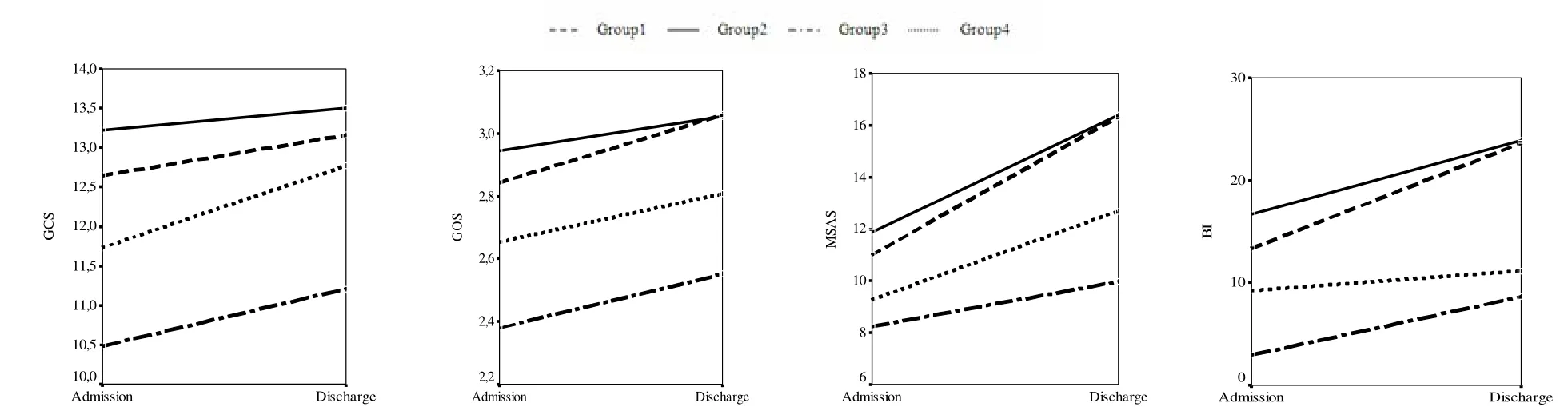
Admission DischargeAdmission DischargeAdmission DischargeAdmission Discharge Figure 1 Changes in Glasgow Coma Scale (GCS), Glasgow Outcome Scale (GOS), Mobility Scale for Acute Stroke Patients (MSAS) and Barthel Index (BI) scores after early physiotherapy.
Comparison of GCS, GOS, MSAS and BI scores at admission and discharge
There were significant differences among groups in the GCS, GOS, MSAS and BI scores at admission and discharge (P< 0.05; Table 2). At admission, these differences were most significant between Groups 1 and 3 and between Groups 2 and 3 (P< 0.008). At discharge, the GCS, GOS and BI scores were significantly different only between Groups 1 and 3 (P<0.008), and the MSAS score was significantly different between Groups 1 and 3 and between Groups 2 and 3 (P< 0.008). These results indicate that patients with a Hunt and Hess grade of ≤ II had a better functional status than those with a Hunt and Hess grade of ≥ III after treatment with surgical clipping or endovascular embolization (Figure 1, Table 2).
The changes in GCS and GOS scores were not significantly different among the study groups (P> 0.05; Table 2). The changes in the MSAS and BI scores were more significantly different in patients with a Hunt and Hess grade of ≤ II than with a Hunt and Hess grade of ≥ III (P< 0.008) (Figure 1, Table 2).
DISCUSSION
The results of this study demonstrate that level of consciousness, functional status, mobility and independence in activities of daily living improved after early physiotherapy in patients with cerebral aneurysms who had undergone surgical clipping or endovascular embolization. Additionally, patients with a worse clinical status at onset tended to have a poorer functional status at discharge.
Only a few studies have described the outcomes of early physiotherapy in patients with cerebral aneurysms[6-9]. Clinchotet al[7]reported that the average length of rehabilitation stay was 41 days (range 11-188 days) in patients with aneurysmal subarachnoid hemorrhage. Saciriet al[6]reported that the average length of hospital stay was 21 days (range 8-105 days) and the average duration of early physiotherapy was 21 days (range 6-85 days) in patients who had undergone surgical repair of ruptured aneurysms, which is similar to our results.
The results of previous studies and the current study show that early physiotherapy after treatment for cerebral aneurysms is not sufficient for patients to achieve full independence[6-8]. Rehabilitation should therefore be continued after discharge. Previous studies have shown that the severity of cognitive impairment affects the functional status and the degree of supervision required[1,6]. For this reason, patients cannot achieve full independence in activities of daily living even though they have achieved recovery of motor skills[1,6].
In conclusion, the results of the current study demonstrate that level of consciousness, functional status, mobility and independence in activities of daily living improved after early physiotherapy in patients with cerebral aneurysms who underwent surgical clipping or endovascular embolization. Patients with a worse clinical status at onset tended to have a poorer functional status at discharge. The choice of surgical clipping or endovascular embolization did not affect outcomes.
SUBJECTS AND METHODS
Design
A retrospective review of medical records.
Time and setting
This study was performed at Hacettepe University Hospital, Turkey from January 2007 to November 2009.
Subjects
Patients with ruptured or unruptured cerebral aneurysms who underwent surgical clipping or endovascular embolization were given early physiotherapy at the Department of Neurosurgery, Hacettepe University Hospital. The diagnosis of cerebral aneurysm was confirmed by CT, MRI or angiography.
Methods
Patients were clinically assessed by a neurosurgeon at admission using the Hunt and Hess grading system[10]. This system is widely used to predict prognosis, with a higher score correlating with a lower survival rate. Patients were divided into two groups according to a Hunt and Hess grade of ≤ II or ≥ III. Patients in each group were then divided into two subgroups according to whether they underwent surgical clipping or endovascular embolization: Group 1, Hunt and Hess grade ≤ II and surgical clipping; Group 2, Hunt and Hess grade ≤ II and endovascular embolization; Group 3, Hunt and Hess grade ≥ III and surgical clipping; Group 4, Hunt and Hess grade ≥ III and endovascular embolization. Medical reports, endovascular and surgical reports, discharge summaries, age, gender, aneurysm location, length of hospital stay, and length of inpatient physiotherapy were retrospectively reviewed.
Early physiotherapy program
The aims of the physiotherapy program were to avoid complications of bed rest, improve postural control and functional activity, and provide post-discharge education for patients and their families. Physiotherapy was based on the Bobath concept and included individualized therapy sessions. Patient-centered goals were developed at the start of therapy. Physiotherapy focused on muscle control, quality of movement, weight bearing and trunk stability. Unilateral or bilateral activities were undertaken in the lying, sitting or standing positions depending on the condition of the patient. Activities were active or passive, again depending on the condition of the patient. Throughout the session, patients were given stimuli to develop a normal sense of movement. Caregivers were trained in correct patient positioning at all times, and were taught exercises that patients could perform during weekends. Physiotherapy was given 5 days a week until hospital discharge.
Outcome measures
All patients were evaluated in the intensive care unit by a physiotherapist before and after early physiotherapy. Level of consciousness, functional status, mobility and independence in activities of daily living were assessed. The GCS was used to evaluate the level of consciousness and degree of brain injury[11]. This score evaluates visual, motor and verbal responses to stimuli. GCS scores range from 3 to 15, with a lower score indicating more severe damage and a poorer prognosis. A score of 15 indicates normal, 13-14 indicates mild disability, 9-12 indicates moderate disability, and 3-8 indicates severe disability.
The functional status of patients was assessed using the GOS. This is a global score of functional outcome that classifies patients into five categories: 5, excellent (return to the original functional level and employment with no deficits); 4, good (minor neurological deficit that does not interfere with daily functioning or employment); 3, fair (significant neurological deficit that interferes with daily activities or prevents return to employment); 2, poor (coma or severe deficit rendering the patient totally dependent); and 1, death[12].
Mobility was evaluated using the MSAS.This score is based on the amount of assistance needed for six mobility tasks: bridging, sitting from supine, sitting balance, standing from a chair, and standing balance and gait. Performance is scored from 1 (patient makes no contribution to the activity) to 6 (patient performs the activity unassisted) with a maximum total score of 36[13]. Functional performance and independence in activities of daily living were evaluated using the BI, which has a maximum score of 100. A higher score indicates better functional performance and more independence. The ten activities of daily living assessed are feeding, moving from a wheelchair to a bed and returning, grooming, transferring to and from a toilet, bathing, walking on a level surface, going up and down stairs, dressing, and bowel and bladder continence[14].
Statistical analysis
All data were analyzed using SPSS 11.5 for Windows (SPSS, Chicago, IL, USA). The normality of data was tested using the Kolmogorov-Smirnov test. Normally distributed data (age) were compared using analysis of variance and expressed as mean ± SD unless otherwise stated. The chi-square test was used to compare categorical variables. For non-normally distributed data (Hunt and Hess grade, length of hospital stay, length of inpatient physiotherapy, GCS, GOS, MSAS and BI), comparisons of values before and after early physiotherapy were performed using the Wilcoxon signed-rank test and data were expressed as median and interquartile range. Statistical significance was set atP< 0.05. The four groups were compared using Kruskal-Wallis analysis of variance, followed by paired Mann-WhitneyUtests with statistical significance set atP< 0.008.
Author contributions: All authors participated in the study design, conduct, and evaluation. All authors contributed to preparation of the manuscript.
Conflicts of interest: None declared.
Ethical approval: The study protocol was approved by the Ethics Committee of Hacettepe University, Turkey.
[1] Vega C, Kwoon JV, Lavine SD. Intracranial aneurysms:current evidence and clinical practice. Am Fam Physician. 2002;66:601-608.
[2] Chung RY, Carter BS, Norbash A, et al. Management outcomes for ruptured and nonruptured aneurysms in the elderly. Neurosurgery. 2000;47:827-832.
[3] Wiebers DO, Whisnant JP, Huston J 3rd, et al. International Study of Unruptured Intracranial Aneurysms Investigators. Unruptured intracranial aneurysms: natural history, clinical outcome, and risks of surgical and endovascular treatment. Lancet. 2003;362:103-110.
[4] Yamashiro S, Nishi T, Koga K, et al. Postoperative quality of life of patients treated for asymptomatic unruptured intracranial aneurysms. J Neurosurg. 2007;107:1086-1091.
[5] King JT Jr, Tsevat J, Roberts MS. Preference-based quality of life in patients with cerebral aneurysms. Stroke. 2005;36:303-309.
[6] Saciri BM, Kos N. Aneurysmal subarachnoid hemorrhage:outcomes of early rehabilitation after surgical repair of ruptured intracranial aneurysms. J Neurol Neurosurg Psychiatry. 2002;72:334-337.
[7] Clinchot DM, Bogner JA, Kaplan PE. Cerebral aneurysms:analysis of rehabilitation outcomes. Am J Phys Med Rehabil. 1997;78:346-349.
[8] Dombovy ML, Drew-Cates J, Serdans R. Recovery and rehabilitation following subarachnoid hemorrhage. Part I:Outcome after inpatient rehabilitation. Brain Inj. 1998;12:443-454.
[9] Kara B, Yozbatiran N, Arda MN. Functional results of physiotherapy programme on patients with aneurysmal subarachnoid hemorrhage. Turk Neurosurg. 2007;17:83-90.
[10] Hunt WE, Hess RM. Surgical risk as related to time of intervention in the repair of intracranial aneurysms. J Neurosurg. 1968;28:14-20.
[11] Teasdale GM, Pettigrew LE, Wilson JT, et al. Analyzing outcome of treatment of severe head injury: a review and update on advancing the use of the Glasgow Outcome Scale. J Neurotrauma. 1998;15:587-597.
[12] Jennett B, Bond M. Assessment of outcome after severe brain damage. Lancet. 1975;1:480-481.
[13] Simondson JA, Goldie P, Greenwood KM. The mobility scale for acute stroke patients: concurrent validity. Clin Rehabil. 2003;17:558-564.
[14] Mahoney FI, Barthel D. Functional evaluation: the Barthel Index. Md State Med J. 1965;14:56-61.
Cite this article as:Neural Regen Res. 2012;7(24):1900-1905.
Arzu Guclu-Gunduz☆, Ph.D., P.T., Department of Physiotherapy and Rehabilitation, Faculty of Health Sciences, Gazi University, Ankara, Turkey
Arzu Guclu-Gunduz, Department of Physiotherapy and Rehabilitation, Faculty of Health Sciences, Gazi University, Emniyet Mahallesi, Muammer Yasar Bostanci Cad. No.16
Besevler/Ankara, 06500 Turkey
arzuguclu@hotmail.com
2012-04-19
2012-07-03
(NY20120413003/H)
Guclu-Gunduz A, Bilgin S, Köse N, Oruckaptan H. Outcomes of early physiotherapy in patients with cerebral aneurysms treated by surgical clipping or endovascular embolization. Neural Regen Res.
2012;7(24):1900-1905.
www.crter.cn
www.nrronline.org
10.3969/j.issn.1673-5374. 2012.24.009
We would like to thank Celik Bulent from the Department of Biostatistics, Faculty of Health Sciences, Gazi University, Turkey for help with statistical analysis.
(Edited by Li S, de Oliveira MF/Song LP)
猜你喜欢
杂志排行
中国神经再生研究(英文版)的其它文章
- Effects of wind-dispelling drugs and deficiency-nourishing drugs of Houshiheisan compound prescription on astrocyte activation and inflammatory factor expression in the corpus striatum of cerebral ischemia rats****☆
- Acupuncture and moxibustion for visceral pain
- Therapeutic effect of nerve growth factor on cerebral infarction in dogs using the hemisphere anomalous volume ratio of diffusion-weighted magnetic resonance imaging*★
- Pre-ischemia electro-acupuncture potentiates the expression of Bcl-2 and transforming growth factor-beta 1 in rat brains*☆△◇
- Yizhijiannao Granule and a combination of its effective monomers, icariin and Panax notoginseng saponins, inhibit early PC12 cell apoptosis induced by beta-amyloid (25-35)☆
- Acupuncture activates signal transduction pathways related to brain-tissue restoration after ischemic injury**☆