Changes in the level of micro RNA-206 gene exPression in Patients with tyPe I biPolar disorder before and after treatment and comParison with a control PoPulation
2011-07-18ZuoweiWANGZezhiLILingxiaoWANGZhiguoWUChengmeiYUANWuHONGShunyingYUYiruFANG
Zuowei WANG,Zezhi LI,Lingxiao WANG,Zhiguo WU,Chengmei YUAN,Wu HONG,Shunying YU,Yiru FANG*
·Research Article·
Changes in the level of micro RNA-206 gene exPression in Patients with tyPe I biPolar disorder before and after treatment and comParison with a control PoPulation
Zuowei WANG1,2,Zezhi LI1,Lingxiao WANG1,Zhiguo WU1,Chengmei YUAN1,Wu HONG1,Shunying YU1,Yiru FANG1*
Background:Micro RNA-206(miRNA-206)is a potential biomarker of bipolar disorder that has not yet been fully investigated.
Obiective:Assess the relationship between the level of miRNA-206 in peripheral blood and the clinical state of patients in the manic phase of bipolar disorder.
Methods:Thirty-six newly admitted patients in the manic phase of type I bipolar disorder(diagnosed using the Structured Clinical Interview for DSM IV Axis I disorders)and 30 age and gender matched healthy controls were enrolled.miRNA-206 levels in peripheral blood lymphocytes were assessed at the time of enrollment in control subjects and at baseline and at the end of the second,fourth and eighth week of treatment in the patient group.The severity of manic symptoms in the patient group was evaluated at the same time as the miRNA-206 assessments using the Young Mania Rating Scale.
Results:There were no statistically significant differences in baseline miRNA-206 levels between patients and controls(Z=-0.02,P=0.988)or,in the patient group,between baseline levels and those at the end of the second (Z=-0.17,P=0.864),fourth(Z=-0.86,P=0.392)and eighth(Z=-1.29,P=0.197)weeks after initiating treatment.There were also no statistically significant correlations between the miRNA-206 level and the severity of manic symptoms at any of the four time points(rs=0.13,P=0.518;rs=0.12,P=0.532;rs=-0.18,P=0.361; and rs=0.02,P=0.912;respectively).
Conclusion:The activity of miRNA-206 in peripherally blood lymphocytes does not appear to be a biomarker of type I bipolar disorder or a biomarker for treatment efficacy during the treatment of a manic episode.But the power to detect differences between patients and controls in the study was only 22%so further research with larger samples(possibly using different techniques to assess miRNA-206 activity)are needed to confirm these findings.
Bipolar disorder;Manic episode;MicroRNA-206;Lymphocytes;Gene expression
1 Introduction
The pathogenesis of bipolar affective disorder (BAD)involves the complex interaction of multiple genetic and environmental factors.The diverse clinical phenotypes of the disorder include core emotional symptoms combined with abnormalities in cognition,autonomic functioning,endocrine systems and sleep[1].In recent years genetic studies have shown that BAD is a polygenetic condition[2]. Increased attention to abnormalities in the regulation and plasticity of neural circuits has led to a growing consensus that the pathogenesis of BAD—like that for other psychiatric disorders—is far more complicated than a simple deficiency or excess of neurotransmitters[1].This consensus is further supported by psychopharmacological studies of mental disorders which typically find relatively long delays between the initiation of treatment and clinical effectiveness—suggesting that latent downstream effects of medication on gene and protein expression mediate clinical efficacy[1].
Micro RNAs(miRNAs)are a newly discovered type of nonprotein coding RNA composed of 22 nucleotides primarily situated in introns(i.e.,gene spacer regions)that may regulate up to onethird of all genes in the human genome[3].miRNAs regulate a wide range of processes including the development,differentiation,proliferation andapoptosis of neurons;immunological responses; neuronal plasticity;and,possibly,the post-transcriptional processing of mRNA during signaling transduction[4,5].There is increasing evidence that miRNAs may be significant contributors to the pathogenesis of a variety of psychiatric diseases including schizophrenia,bipolar disorder and autism[6,7]. Some researchers hypothesize that miRNA-206,which is involved in the regulation of brain-derived neurotrophic factor(BDNF)[8],may be a factor in the causal pathway for multiple psychiatric diseases,particularly bipolar disorder[9].
Most previous studies about the role of miRNAs in the pathogenesis of bipolar disorder have been based on animal models used in psychopharmacological trials.One previous clinical study from China reported lower plasma miRNA-134 levels in patients with bipolar disorder than in control subjects and a negative correlation between the severity of mania and the miRNA-131 level[10].Many signaling pathways related to the hypothesized pathogenesis of bipolar disorder—including BDNF,p53,Notch3,estrogen and others—are closely related to miRNA-206[11-13]so this is another candidate biomarker for bipolar disorder that merits investigation.To help determine whether or not miRNA-206 could be a biological marker for bipolar disorder and/or for the severity of mania in persons with bipolar disorder,the current study compares peripheral blood lymphocyte levels of miRNA-206 between bipolar patients with untreated acute mania and normal control subjects and compares the levels of miRNA-206 in manic patients over the course of treatment of their acute mania.
2 Methods
2.1 Subiects
Figure 1 provides a flowchart of the enrollment of study subjects.Patients with a clinical diagnosis of type-I bipolar disorder hospitalized at the Shanghai Mental Health Center of the Shanghai Jiao Tong University School of Medicine or at the Hongkou District Mental Health Center(in Shanghai)from November 2009 to December 2010 were eligible for the study.Inclusion criteria were as follows:1) satisfies the diagnostic criteria for bipolar disorder as assessed by the Clinical Interview for DSM-IV Axis I Disorders,Patient Version(SCID-P)[14](administered by a clinical psychiatrist);2)currently experiencing a manic episode according to DSM-IV criteria;3)Han ethnicity;4)18-65 years of age;5)at admission the Young Mania Rating Scale (YMRS)score was≥20;6)The Clinical Global Impressions Scale bipolar disorder severity score of the(CGI-BP-S)was≥4;and 7)patients were either drug naïve or had discontinued any previous psychiatric medications for at least four weeks prior to enrollment.Exclusion criteria included 1)known intolerance to lithium or quetiapine;2)serious suicidal ideation;3)co-morbid substance dependence or any Axis II disorder diagnosis;4)pregnant or lactating;and 5)presence of cardiac disease,significant organic brain disease,diabetes,or other serious medical condition.Based on these criteria 36 patients(16 males and 20 females)were enrolled in the study:they had a mean(SD)age of 37.5 (1.6)years;the range in the duration of illness was 1-456 months(median=88.5 months,interquartile range=48-156 months);the mean number of manic episodes(including the index episode)was 3.9(1.7)episodes;and at admission their mean (SD)YMRS score was 31.2(5.0)and their mean CGI-BP-S score was 5.36(0.68).

Figure 1.Flowchart of subiect enrollment
The control group consisted of staff members and medical students at the two mental health centers who responded to a request for volunteers and met the following inclusion and exclusion criteria:1)did not meet any current DSM-IV diagnosis as assessed by administering the SCID-P;2)Han ethnicity;3)18-65 years of age;4)no family history of mental disorders;5)no significant medical history; and 6)not currently using any type of medications. Thirty-one control subjects were enrolled including 13 males and 18 females;their mean(SD)age was 36.9(6.3)years.There were no significant differences between patients and controls by gender (χ2=0.04,P=0.836)or by age(t=0.22,P= 0.825).
The Institutional Review Board of the Shanghai Mental Health Center reviewed and approved the study protocol.Written informed consent was obtained from each subject before any study-related procedure was performed.
2.2 Pharmacological treatment of manic Patients
Lithium salt and quetiapine were used in combination to treat patients’manic episodes.Lithium blood levels reached the therapeutic effective concentration(≥0.6 mmol/L)within the first two weeks of treatment.Quetiapine was gradually increased to the recommended dosage range of 600-750 mg/d.Both medications were then continued for the remainder of the 8-week trial.The mean dose of lithium during the trial was 1330(193) mg/d,the mean blood lithium concentration was 0.80(0.14)mmol/L,and the mean dose of quetiapine was 657(73)mg/d.Other psychotropic medications were not used except for short-acting benzodiazepines for sleep or to treat severe anxiety or agitation.
2.3 RNA extraction
Five ml of fasting venous blood was collected from the subject’s brachial vein in the morning with 2%ethylenediaminetetraacetic acid(EDTA)as the anticoagulation.These samples were collected at enrollment and,for the patient group,at the end of the second,fourth and eighth week of treatment.Ficoll lymphocyte separation medium(Ficoll-Plaque Plus,GE Healthcare Bio.Sciences AB,Sweden) was utilized to isolate lymphocytes,then the total RNA mirVanaTM miRNA isolation Kit(Applied Biosystems,CA,USA)was used to extract the total RNA in the peripheral blood.Finally the TaqMan MicroRNA Reverse Transcription Kit(Applied Biosystems,CA,USA)was used to synthesize the cDNA.TaqMan fluorescent RT-qPCR was then carried out using the 384-well ABI Prism 7900 Sequence Detection System(Applied Biosystems,CA,USA)for the fluorescent real-time quantitative PCR amplification.During this process the TaqMan MGB probe method was utilized to assess the level of expression of miRNA-206.The housekeeping gene U6 snRNA was used as the internal reference gene to normalize the expression level of the target gene(miRNA-206).
The RNA data were analyzed using the 2.1 version of the Sequence Detector Software(SDS) (Applied Biosystems,CA,USA)for the real-time collection of fluorescent signals,followed by using the Comparative Ct Values(ΔCt)process to calculate the relative expression level of the target gene compared to that of the internal reference gene[10,15].This value is computed and provided by the Sequence Detector Software(SDS)version 2.1 in the ABI Prism 7900 sequencer.The target gene and the internal reference gene for each sample was repeated three times and the reported result was the mean value of the three assessments.
2.4 Assessment of clinical status
The Young Mania Rating Scale(YMRS)was administered to all patients by a single trained clinical psychiatrist at baseline and,in the patient group,at the end of the second,fourth and eighth week of treatment.The reliability and validity of the Chinese version of the YMRS has not been fully assessed.
2.5 Statistical Analysis
We used the SPSS 13.0 software package for the analysis.Mann-Whitney rank sum tests were used to compare differences in the expression levels of miRNA-206 between the patient group and the control group;Friedman tests were used tocompare miRNA-206 levels in the patient group over the four time periods(baseline,and 2,4,and 8 weeks after starting treatment).In the patient group Spearman rank correlation analysis was carried out to assess the correlation between the expression level of miRNA-206 and the severity of manic symptoms at each of the four time periods. Repeated measures analysis of variance was used to compare changes in YMRS score before and after the treatments.The last observation carried forward method(LOCF)was utilized to handle cases where treatment had been discontinued prior to the end of the study.All of the statistical tests used twotail tests with α=0.05 as the level for statistical significance.
3 Results
3.1 miRNA-206 levels in BAD Patients and healthy controls at different time Points
As shown in Table 1,there were no statistically significant differences between the median miRNA-206 level in the control group at enrollment and the median values in the patient group at any of the four time periods(i.e.,pre-treatment and 2,4 and 8 weeks after starting treatment).In the patient group the miRNA-206 levels over the four time periods did not change significantly(Friedman test,χ2=4.23,P=0.238).
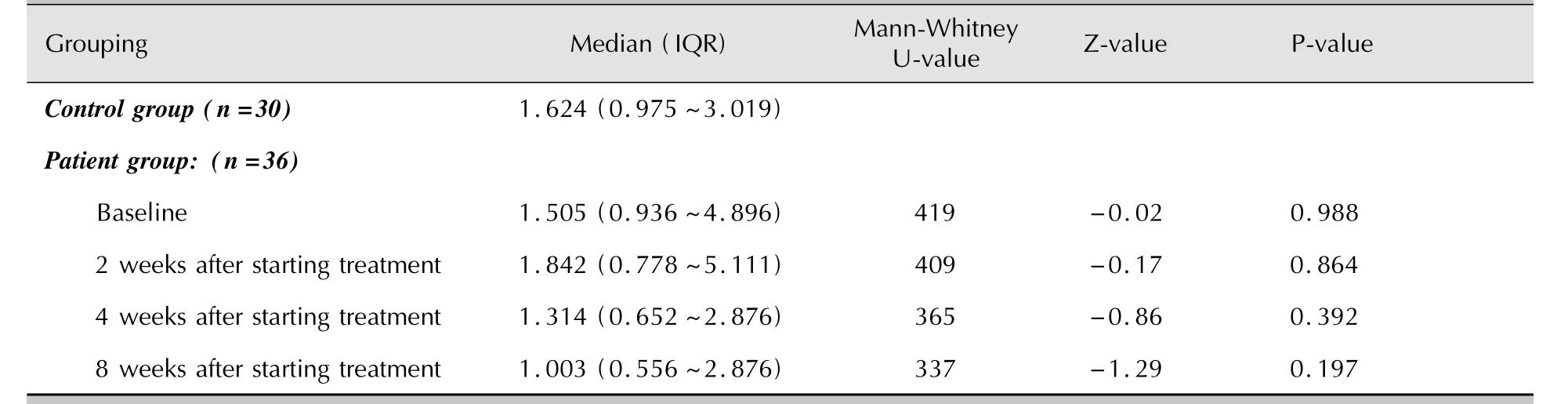
Table 1.ComParison of median micoRNA-206 levels in Patients in the manic Phase of biPolar affective disorder with those in healthy controls subiects
3.2 Correlations between miRNA-206 and YMRS scores
In the patient group,the mean YMRS scores at the end of the second(19.96,SD=5.55),fourth (12.21,SD=5.50)and eighth(5.21,SD=0.38) week after initiating treatment were all significantly lower that the mean pre-treatment YMRS score (31.18,SD=5.00)(F=140.78,df=33,P<0.001). But the ranked correlations of the miRNA level and the YMRS total score were all relatively weak and statistically non-significant:at baseline rs=0.13 (P=0.518),after two weeks of treatment rs=0.12 (P=0.530),after four weeks of treatment rs= -0.18(P=0.361),and after eight weeks of treatment rs=0.02(P=0.912).Moreover,the correlation of the pre-treatment versus post-treatment(i.e.,8-week)change in the miRNA-206 levels and change in YMRS scores was not statistically significant(rs=0.01,P=0.964).
4 Discussion
4.1 Maior Findings
This is the first study to assess the relationship of miRNA-206 to the occurrence and symptom severity of mania in bipolar I disorder patients.A previous study with another miRNA found a relationship between miRNA-134 levels and mania[10],but this study found no significant relationship between peripheral lymphocyte levels of miRNA-206 and the occurrence of manic episodes in bipolar I disorder or with the severity of manic symptoms in those who are experiencing a manic episode.These results suggest that miRNA-206 is not a biomarker of type I bipolar disorder or a biomarker for treatment efficacy during the treatment of a manic episode.However,the power of this study to detect differences between the patient group and control group was relatively low(22%)so these negative results must be considered preliminary;larger samples would be needed to confirm these results.
4.2 Limitations
The relatively small sample size and the nonnormal distribution of the miRNA values decreased the power of the study to detect differences(power= 22%)so it is possible that this negative finding obscures real differences(that is,a type II error).[Based on the identified difference between patients and controls,at least 157 subjects in each arm of the study would be needed to detect a significant difference at α=0.05 with a power of 80%.]Small sample size also made it impossible to adjust the results for potential confoundingvariables including duration of illness,family history,prior medication history,and so forth.It is,moreover,unclear how representative these inpatients are of the larger pool of bipolar I patients;it is certainly possible that the results could be different in a different subpopulation of bipolar patients.The use of combined treatment with lithium and quetiapine may have obscured the relationship between miRNA levels and bipolar disorder;previous studies use monotherapy lithium in animal models of bipolar disorder[1].And the use of serum levels of miRNA cannot help identify differential miRNA levels in different regions of the brain—the relationship of miRNA to bipolar disorder may only be relevant for specific brain regions.
4.3 ImPlications
Despite this study’s negative results,several lines of theory and research suggest a significant relationship between miRNA-206 activity and the pathogenesis of mental disorders so further research with larger samples that uses alternative methods of assessing this relationship should be conducted.We found that peripheral blood lymphocyte activity levels of miRNA-206 was not related to bipolar disorder or to the severity of mania,but this approach only considers one possible method of assessing this relation ship.The expression levels of miRNA-206 in central and peripheral tissues may differ,the effect of miRNA-206 activity may be tissue specific,and miRNA-206’s functional mechanisms of action may be different for different target genes. These alternatives need to be assessed in future research with samples that are large enough to control for potential confounders before rejecting this promising candidate biomarker.
Conflict of interest
The authors report no conflict of interest regarding this paper.
Funding
Funding was provided by the National Natural Science Foundation of China(grant No.30971047) and the project was supported by the Department of Public Health of the Hongkou District of Shanghai(project No.91 for 2010).
1. Zhou R,Yuan P,Wang Y,Hunsberger JG,Elkahloun A,Wei Y,et al.Evidence for selective microRNAs and their effectors as common long-term targets for the actions of mood stabilizers.Neuropsychopharmacology,2009,34(6):1395-1405.
2. Schloesser RJ,Huang J,Klein PS,Manji HK.Cellular plasticity cascades in the pathophysiology and treatment of bipolar disorder.Neuropsychopharmacology,2008,33(1):110-133.
3. Wang ZW,Yu SY,Fang YR.MicroRNAs and its application in the study of mental illness.Chinese Journal of Nervous and Mental Diseases,2010,36(8):508-510.(in Chinese)
4. WU YY,Li L.MicroRNAs and cancer-associated signal transduction pathways.Hereditas,2007,29(12):1419-1428.(in Chinese)
5. Xia W,Cao GJ,Shao NS.The research progress of searching and identification of MicroRNA target genes.Science in China series C:Life Science,2009,39(1):121-128.(in Chinese)
6. Dinan TG.MicroRNAs as a target for novel antipsychotics:a systematic review of an emerging field.Int J Neuropsychopharmacol,2010,13(3):395-404.
7. Miller BH,Wahlestedt C.MicroRNA dysregulation in psychiatric disease.Brain Res,2010,1338:89-99.
8. Hansen T,Olsen L,Lindow M,Jakobsen KD,Ullum H,Jonsson E,et al.Brain expressed microRNAs implicated in schizophrenia etiology.PLoS One,2007,2(9):e873.
9. Barbosa IG,Huguet RB,Mendonça VA,Neves FS,Reis HJ,Bauer ME,et al.Increased plasma levels of brain-derived neurotrophic factor in patients with long-term bipolar disorder. Neurosci Lett,2010,475(2):95-98.
10. Rong H,Liu TB,Yang KJ,Yang HC,Wu DH,Liao CP,et al. MicroRNA-134 plasma levels before and after treatment for bipolar mania.J Psychiatr Res,2011,45(1):92-95.
11. Lin PY.State-dependent decrease in levels of brain-derived neurotrophic factor in bipolar disorder:a meta-analytic study. Neurosci Lett,2009,466(3):139-143.
12. Suzuki HI,Yamagata K,Sugimoto K,Iwaoto T,Kato S,Miyazono K.Modulation of microRNA processing by p53.Nature,2009,460(7254):529-533.
13. Miyachi M,Tsuchiya K,Yoshida H,Yagyu S,Kikuchi K,Misawa A,et al.Circulating muscle-specific microRNA,miR-206,as a potential diagnostic marker for rhabdomyosarcoma.Biochem Biophys Res Commun,2010,400(1):89-93.
14. Li T,Zhou RY,Hu JM,Ma XH,Wang Q.Structured Clinical Interview for DSM-IV-TR Axis I Disorders-Patient Edition.Chengdu:Institute of Psychology,Sichuan University West China Medical School,2004.(in Chinese)
15. Yuan JH.Experimental Research on Real-Time Fluorescent Quantitative PCR.Modern Agricultural Wciences and Technology,2010,13:20-22.(in Chinese)
双相障碍I型患者治疗前后微小RNA206基因表达水平变化及与对照的比较
汪作为1,2李则挚1王凌霄1吴志国1苑成梅1洪 武1禹顺英1方贻儒1
国家自然科学基金(30971047);虹口区医学重点专科建设项目[虹卫(2010)91号];虹口区重大医学科研课题[虹卫1101-02]
1上海交通大学医学院附属精神卫生中心心境障碍科200030;2上海市虹口区精神卫生中心200083
方贻儒,电子信箱yirufang@yahoo.com.cn
背景微小RNA206(MicroRNA-206,miRNA-206)可能是双相障碍的生物学标志之一,有待深入探究。
目的评估双相障碍躁狂发作期外周血miRNA-206水平与患者临床状态的关系。
方法采用美国精神障碍诊断与统计手册第4版轴I障碍定式临床检查,符合双相障碍I型躁狂发作期的新入院患者36例和年龄、性别匹配的健康对照者30名纳入研究。健康对照者入组时,双相障碍患者在基线、治疗后第2、4、8周末外周血淋巴细胞miRNA-206水平被检测。在检测miRNA-206水平相同时间点,采用杨氏躁狂量表(Young Mania Rating Scale,YMRS)评估双相障碍患者躁狂症状严重程度。
结果在基线(Z=-0.02,P=0.988)和治疗后第2周末(Z=-0.17,P=0.864)、第4周末(Z=-0.86,P=0.392)、第8周末(Z=-1.29,P=0.197),双相障碍患者与健康对照者之间外周血miRNA-206水平差异无统计学意义。对于双相障碍患者,在4个时间点miRNA-206水平与躁狂症状严重程度之间也无统计学明显相关(统计值依次为:rs= 0.13,P=0.518;rs=0.12,P=0.532;rs=-0.18,P=0.361;rs=0.02,P=0.912)。
结论外周血淋巴细胞miRNA-206水平可能不是双相障碍I型或躁狂发作期治疗效果的生物学标志。由于本研究检测患者与对照者之间差异的统计效能仅22%,今后需要大样本研究(可能应用不同技术检测miRNA-206水平)进一步验证。
双相障碍 躁狂发作 微小RNA-206 淋巴细胞 基因表达
date:2011-03-23;accepted date:2011-09-07)
10.3969/j.issn.1002-0829.2011.05.003
1Division of Mood Disorders,Shanghai Mental Health Center,Shanghai Jiao Tong University School of Medicine,Shanghai,200030 China;2Hongkou District Mental Health Center,Shanghai,200083 China
*Correspondence:yirufang@yahoo.com.cn
·论著·
猜你喜欢
杂志排行
上海精神医学的其它文章
- Binary outcome variables and logistic regression models
- Differences in the levels of suPeroxide dismutase and brain-derived neurotroPhic factor in first-ePisode schizoPhrenia,chronic schizoPhrenia and normal control subiects
- Case-control study of changes in bone mineral density in drug-naïve Patients in the first-ePisode of schizoPhrenia during the first year of treatment with risPeridone
- Randomized controlled trial comParing quetiaPine with lithium and clozaPine with lithium in the treatment of female Patients with mania
- ComParison of the neuroPsychological characteristics of two subtyPes of mild cognitive imPairment
- 精神分裂症的全基因组关联分析研究