抗阻训练对老年人肌肉力量影响的元分析
2011-01-02王光平张开发
王光平,张开发
(1.绵阳师范学院 体育与健康教育学院运动医学教研室,四川 绵阳 621000;2.绵阳师范学院 校医院,四川 绵阳 621000)
抗阻训练对老年人肌肉力量影响的元分析
王光平1,张开发230
(1.绵阳师范学院 体育与健康教育学院运动医学教研室,四川 绵阳 621000;2.绵阳师范学院 校医院,四川 绵阳 621000)
评价抗阻训练对改善老年人肌肉力量的效果,为抗阻训练处方的制定提供依据,以MEDLINE和PUBMED为文献主要来源,搜索1990~2010年间公开发表的抗阻训练对老年人肌肉力量影响的相关文献,根据纳入标准和排除标准选择合适的文献,对其进行质量评估和相关数据提取。结果对30篇文献进行元分析后发现,抗阻训练后,老年人腿部伸肌群最大力量加权均数差为6.78 kg,95%可信区间为5.92~7.64 kg,平均最大力量增加了24.2%;腿部屈肌群最大力量加权均数差为1.03 kg,95%可信区间为0.93~1.14 kg,平均最大力量增加了20.3%。卧推最大力量加权均数差为11.52 kg,95%可信区间为10.74~12.29 kg,平均增加了26.9%。说明抗阻训练是能有效改善老年人增龄性肌肉力量减退的干预手段;大强度的抗阻训练较中等强度或小强度的抗阻训练更能有效增强老年人肌肉力量。
运动医学;抗阻训练;肌肉力量;老年人;元分析
肌肉力量增龄性的减退是导致老年人机能障碍的重要原因,骨骼肌的最大力量在40岁后逐年递减,并在65岁左右表现最为突出。尽管有关肌肉力量衰减的纵向研究较少,但现有的资料表明,在受试者寿命的最后10年,其肌肉力量发生显著性的下降,并同时伴随骨骼肌肌纤维的质量减少、肌肉耐力及代谢能力减退、神经支配失调、结缔组织和脂肪增多等退行性改变[1]。研究表明,在老年人肌肉力量衰减早期,抗阻训练是一种安全有效的可直接改善老年人肌肉力量衰减的身体活动方式,可有效增加蛋白合成效率,提高神经肌肉适应性[2]。但如何进行抗阻训练,以何种方式、何种强度可以更好地改善肌肉力量,其相关结果却因研究设计、训练强度、训练方式、样本量等多种因素的不同而不一致。
元(Meta)分析作为循证医学中的主要研究方法,可针对某一个干预措施全面收集所有相关资料,并进行严格评价和分析,将不同的研究进行定量的统计学处理,可对干预效果做出更好的评价。本研究采用Meta分析的方法,检索抗阻训练对老年人肌肉力量影响的相关研究文献,评价其影响作用和最有效的训练强度和训练方案,为抗阻训练运动处方的制定提供依据。
1 研究方法
1.1 文献检索
检索方法:检索 MEDLINE和 PUBMED中(1990~2009年)所有与抗阻训练对老年人肌肉力量影响的文献。检索词为:aging and resistance training(老化和抗阻力量训练)、resistance training and muscle strength(抗阻力量训练和肌肉力量)、aging and muscle strength(老化和肌肉力量)。根据检索到的文献中所列出的相关参考文献,对其进行追溯查找。手工检索本校图书馆的电子期刊、参考文献目录及其它信息来源。初步检索得到了513篇相关文摘及引文,全文112篇。
1.2 文献筛选
为最大程度排除异质性的存在,设置文献纳入标准和排除标准。
文献纳入标准:(1)受试者为未参加其它锻炼方式的普通健康人群,年龄大于50岁。(2)锻炼时间大于6周,须设立对照组;测定肌肉力量的基础值及干预后数值。(3)至少有一组采用抗阻训练方法作为干预手段。(4)同一研究者针对相同人群所做的多篇研究文献,采用最近发表的一篇。
文献排除标准:(1)存在其它干预手段者,因难以判断锻炼效果而排除;(2)排除间歇训练和混合运动组。
1.3 文献评估
采用Jadad等[3]制定的文献评分量表对研究质量,如试验设计是否明确、试验对象是否随机分组,各组病人的年龄、性别、职业等是否相似,治疗作用评价是否准确,是否描述了所有重要的治疗结果等方面进行评分,总分为5分,1~3分属于低质量,4~5分属于高质量。
1.4 资料合成及分析
本研究由两名研究人员独立按照纳入和排除标准筛选文献,进行评价和提取数据信息,提取的数据内容包括个体特征、运动强度、肌肉力量改变情况。经文献检索,共得到513篇关于抗阻训练对老年人肌肉力量影响的研究文献。经阅读摘要和(或)全文,按照纳入和排除标准,共得到有效文献30篇。所有文献评估的平均分为 2.1分。由于抗阻训练的干预方法无法设置双盲对照,因此所有文献均未采用双盲对照。其中18篇文献对训练条件和对照组进行了随机分配,12篇文献只设立了对照组,未对治疗条件进行随机分配。在这30项文献中,包括2项中青年男性与老年男性的比较;1项中青年女性与老年女性的比较研究。将这30篇有效文献进行Meta分析,共计868名受试者,年龄51~82岁((67.4±6.3)岁);16篇文献为男女混合组,8篇文献受试者为男性,6篇文献受试者为女性。训练持续时间为12~52周((20.6±8.6)周),训练频率为每周1~3次((2.7±0.5)d/周),训练强度为40%~80% 1RM((70 ±12.7)% 1RM)。每次锻炼包括1~6组((2.5±1.0)组)。其相关情况见表1。
为了判断Meta分析中是否有发表偏倚的存在,我们将使用漏斗图(即以单个研究估计得来的治疗效果(x轴)与每项研究的样本大小(y轴)所做出的散点图形)的不对称程度来判断其是否存在偏倚。如出现图形不对称,表明存在一定的发表偏倚。
采用Review Manage 4.2软件进行统计分析。若研究间存在临床异质性,则分别进行描述。采用χ2检验进行异质性检验。若各试验间无统计学异质性,选用固定效应模型,否则选择随机效应模型。对二分类变量资料计算比值率及其95%可信区间,对连续性变量资料计算加权均数差值(加权均数差的计算原理是以锻炼干预效应方差的倒数为权重,将每个研究的干预效应量进行加权合并,最后得出合并效应量)及其95%可信区间。
2 结果
2.1 发表偏倚的评价
抗阻训练对老年人肌肉力量影响的 Meta分析的漏斗图见图1。
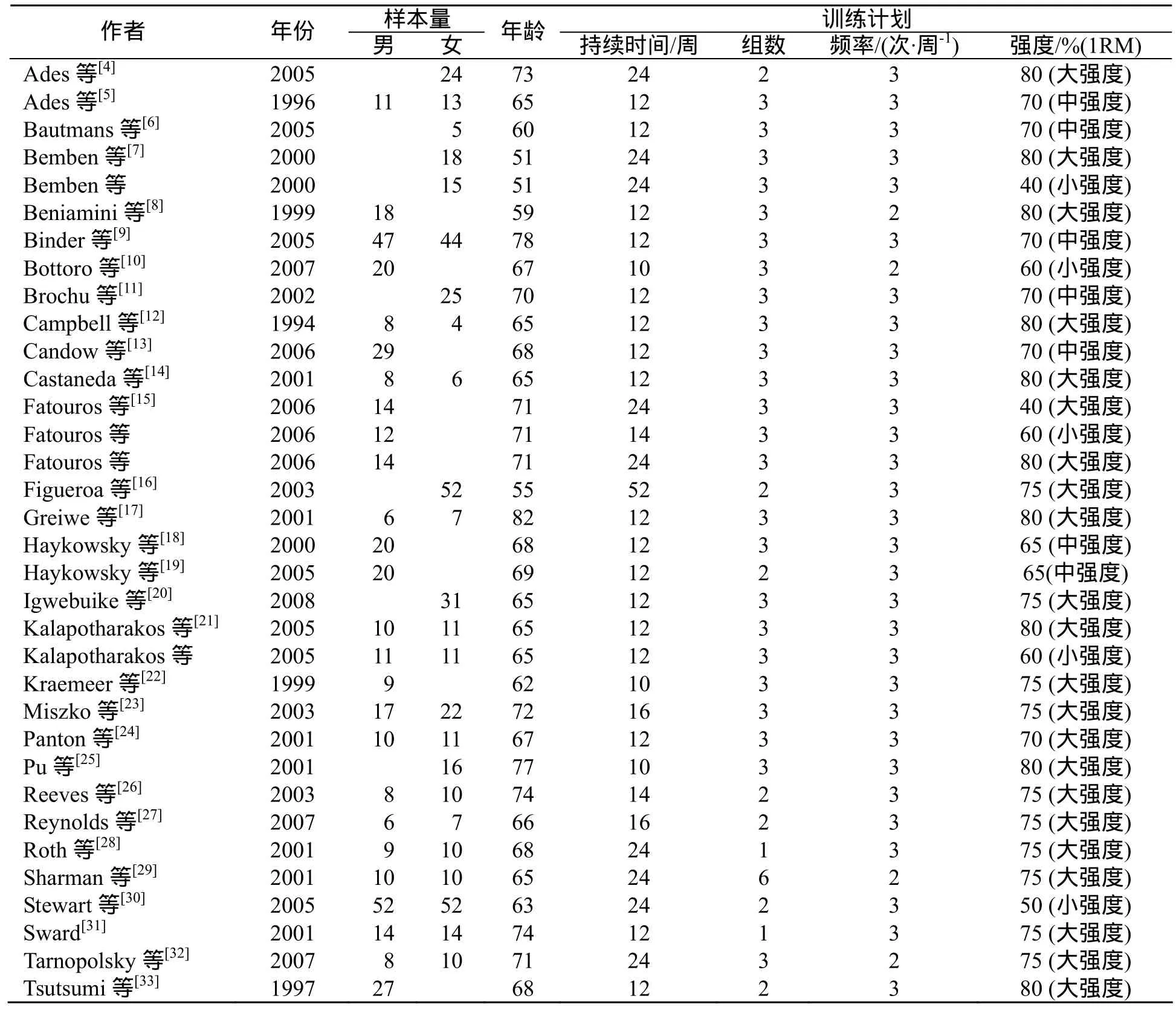
表1 纳入文献中受试者情况及训练计划
如图1所示,漏斗图出现图形不对称,表明存在一定的发表偏倚,也有可能为以下原因所致:阴性结果的研究未能发表、纳入研究的质量较低、纳入研究的样本较小、研究结果的异质性明显等。
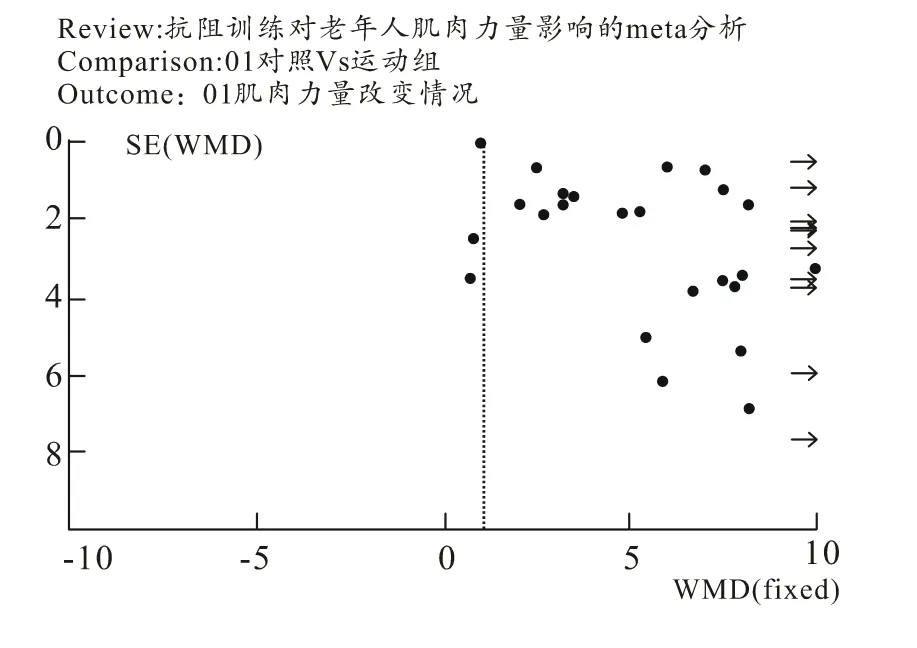
图1 发表偏倚评估漏斗图
2.2 抗阻训练对老年人腿部伸肌群力量的影响
在抗阻训练对老年人腿部伸肌群力量加权均数差的影响森林图中(图2),右边一列均数差中横线代表每个研究结果的可信区间,是真值可能存在的范围,反映结果的准确性,横线中间的点为每个研究干预效应值。最下方的菱形代表多个研究的合并效应量。垂直线将图分为左右两半,用于判断抗阻训练对老年人腿部伸肌群力量的作用有无统计学意义:横线或菱形与垂直线相交表明该研究中锻炼组与对照组相比,腿部伸肌群力量的改变无统计学意义;横线和菱形均在垂直线的右侧,表明锻炼组腿部伸肌群力量的改变具有显著性差异。
如图2所示,对纳入文献的各个研究之间的异质性进行检验,结果为df=21(P=0.001),I2=54.6%,说明存在统计学异质性,故采用随机效应模型计算合并效应值:总效应Z=15.48(P<0.000 01),腿部伸肌群最大力量加权均数差为6.78 kg,95%可信区间为5.92~7.64 kg,具有统计学意义。与受试者锻炼前腿部伸肌群平均最大力量36.02 kg相比,通过抗阻训练使最大力量增加了24.2%。
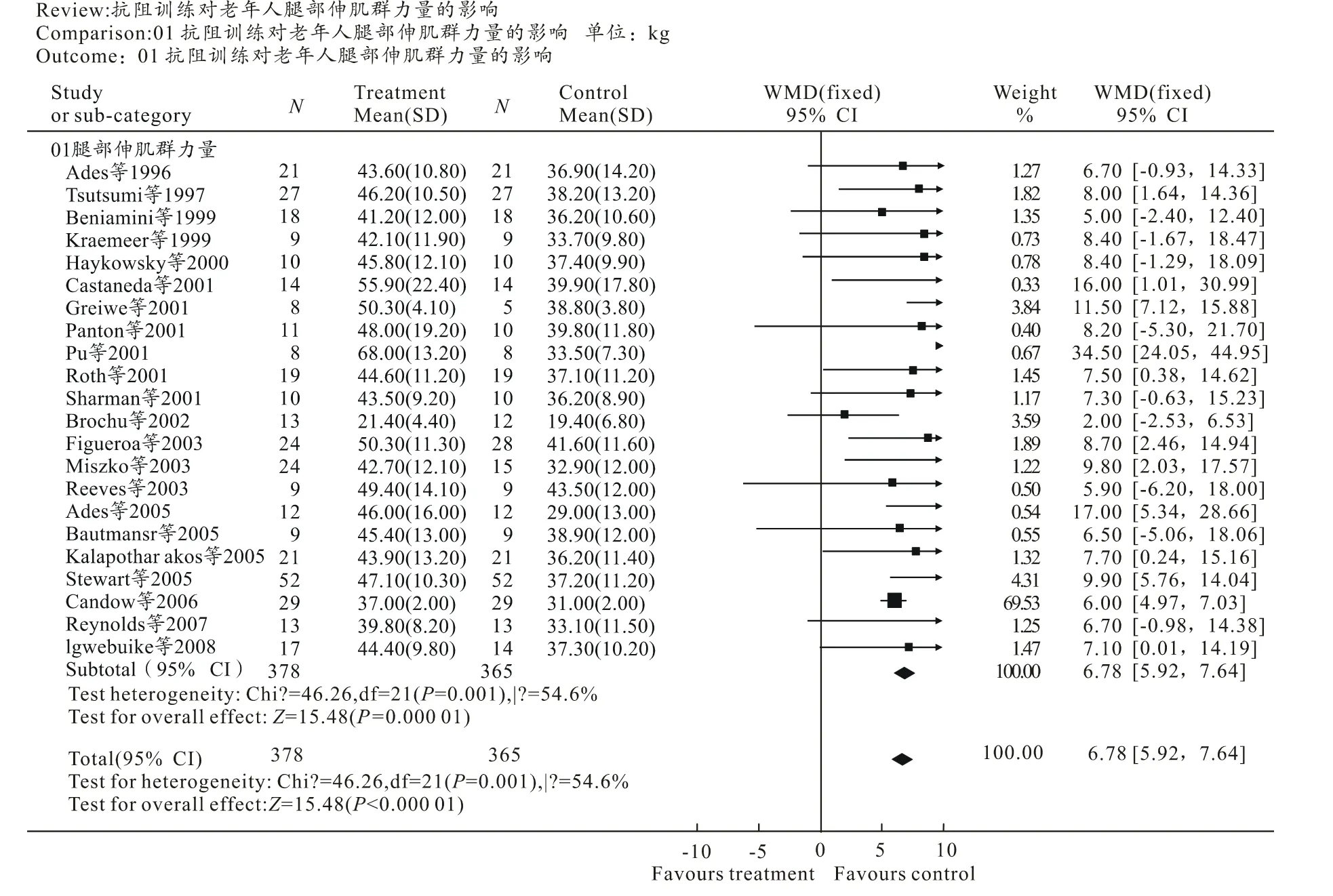
图2 抗阻训练对老年人腿部伸肌群力量加权均数差影响的森林图
2.3 抗阻训练对老年人腿部屈肌群力量的影响
如图3所示,对纳入文献的各个研究之间的异质性进行检验,结果为df=16(P<0.000 01),I2=71.8%,说明存在统计学异质性,故采用随机效应模型计算合并效应值:总效应Z=119.78(P<0.000 01),腿部屈肌群最大力量加权均数差为 1.03 kg,95%可信区间为0.93~1.14 kg,具有统计学意义。与受试者锻炼前腿部屈肌群平均最大力量25.95 kg相比,通过抗阻训练使最大力量增加了20.3%。
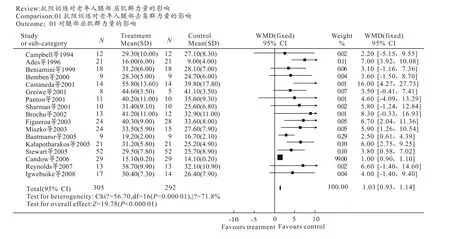
图3 抗阻训练对老年人腿部屈肌群力量加权均数差影响的森林图
2.4 抗阻训练对老年人卧推力量的影响
如图4所示,对纳入文献的各个研究之间的异质性进行检验,结果为df=16(P<0.000 01),I2=82.8%,说明存在统计学异质性,故采用随机效应模型计算合并效应值:总效应Z=29(P<0.000 01),卧推最大力量加权均数差为11.52 kg,95%可信区间为10.74~12.29 kg,具有统计学意义。与受试者锻炼前卧推平均最大力量31.39 kg相比,通过抗阻训练使最大力量增加了26.9%。
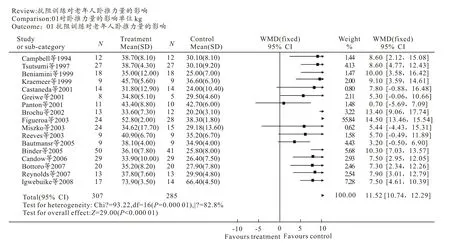
图4 抗阻训练对老年人卧推力量加权均数差影响的森林图
3 讨论
本研究通过Meta分析发现,抗阻训练能有效增加老年人上肢和下肢肌肉力量,表明老年人参与抗阻训练能有效改善增龄性的全身肌肉力量衰减,成为一种新型有效的活动方式。通过本研究发现,所纳入的30篇文献具有异质性,需采用随机效应模型计算合并效应值。本研究共纳入的研究文献中,训练持续时间为10~52周((20.6±8.6)周),训练频率为每周1~3次((2.7 ±0.5) d/周),训练强度为40%~80% 1RM((70±12.7)% 1RM)。每次锻炼包括1~6组((2.5±1.0)组)。将30篇文献按训练强度分为40%~60%、60%~70%、75%~80% 3个亚组,进行亚组Meta分析,结果显示:锻炼强度为75%~80% 1RM,每周3次,每次3组时,老年人肌肉力量增加可达到最大效果,卧推力量可以增加29.5%,腿部伸肌群力量增加 28.6%,腿部屈肌群力量可增加21.4%,这和以往的综述研究结果类似[34]。由图2、图3和图4可知,使用力量训练强度为40%~60% 1RM时,横线或菱形基本与垂直线相交,表明此时锻炼组与对照组相比,肌肉力量的改变无统计学意义;而当力量训练强度为75%~80% 1RM时,横线和菱形均远离垂直线的右侧,表明此时锻炼组与对照组相比,肌肉力量的改变具有显著性差异。由于所纳入的文献中不同强度的力量训练所对应的受试者和肌群部位不同,所以我们无法定量比较不同强度的抗阻训练对老年人肌群力量的效果差异,但仍可以定性判断出大强度的抗阻训练较小强度的抗阻训练更能有效增强老年人肌肉力量。由于所纳入的文献中,训练持续时间绝大部分均超过12周,亚组Meta分析未显示训练持续时间的不同与力量增加具有显著相关,但结合前人研究结果,我们认为抗阻训练应至少持续12周以上。
现有的文献表明,抗阻训练作为康复手段在中青年和老年人群中具有不同的功效[35-36]。但渐进抗阻训练已成为一种有效改善老年人因肌肉力量下降而产生的相关疾病的干预手段。抗阻训练能增加瘦体重使体内瘦体重的百分比增加,降低体脂率,改善身体成分,间接改善整个身体健康状态;抗阻训练也可预防骨质稀少和骨质疏松症,降低骨折的危险,并可有效延缓或阻止增龄性的骨密度下降,Kerr[37]的研究表明,耐力训练组对骨密度作用不明显,而力量训练组骨密度显著增加,且大强度的负荷对增加骨密质的效果最为显著;抗阻训练还可以降低血脂,改善肥胖程度。因此我们认为,对于老年人来说,在保证安全的基础上,应积极参与全身性的抗阻训练,训练持续时间应超过12周,每周至少3次,运动强度应在75% 1RM以上。
所有Meta分析都会存在一些不可避免的局限性,如没有纳入全部的相关研究,不能提取全部相关数据,发表具有偏倚性,资料真实性、文献质量不可控等。本研究的局限在于:(1)本研究仅收录了MEDLINE和PUBMED中所收录的文献,未纳入相关的中文文献,由于阴性结果的论文往往不能发表,所以收集的资料存在偏倚性;(2)所纳入资料中,受试者的性别无法进行有效控制,很多文献未将性别作为独立因素加以区别;(3)纳入文献时间跨度为 20年,测试方法和技术的不断更新,也会对结果产生一定影响;(4)大多数纳入的文献并没有对卧推、伸肌群和屈肌群力量全部进行测定,进行统计时,文献数量较少也会对结果造成一定影响。
4 结论
抗阻训练能有效增加老年人上肢和下肢肌肉力量,是有效改善增龄性的全身肌肉力量衰减的重要手段;大强度的抗阻训练较小强度的抗阻训练更能有效增强老年人肌肉力量,训练持续时间应超过12周,每周至少3次,运动强度应在75% 1RM以上。
[1] Janssen I,Baumgartner R N,Ross R,et al. Skeletal muscle cutpoints associated with elevated disability risk in older men and women[J]. Am J Epidemiol,2004,159:413-421.
[2] Hubal M J,Gordish-Dressman H,Thompson P D,et al. Variability in muscle size and strength gain after unilateral resistance training[J]. Med Sci Sports Exerc,2005,37:964-972.
[3] Jadad A R,Moore R A,Carroll D,et al. Assessing the quality of reports of randomized clinical trials:is blinding necessary?[J]. Control Clin Trials,1996,17(1):1-12.
[4] Ades P A,Savage P D,Brochu M,et al. Resistance training increases total daily energy expenditure in disabled older women with coronary heart disease[J]. J Appl Physiol,2005,98(4):1280-1285.
[5] Ades P A,Ballor D L,Ashikaga T,et al. Weight training improves walking endurance in healthy elderly persons[J]. Ann Intern Med,1996,124(6):568-572.
[6] Bautmans I,Njemini R,Vasseur S,et al. Biochemical changes in response to intensive resistance exercise training in the elderly[J]. Gerontology,2005,51(4):253-265.
[7] Bemben D A,Fetters N L,Bemben M G,et al. Musculoskeletal responses to high-and low-intensity resistance training in early postmenopausal women[J]. Med Sci Sports Exerc,2000,32(11):1949-1957.
[8] Beniamini Y,Rubenstein J J,Faigenbaum A D,et al. High-intensity strength training of patients enrolled in an outpatient cardiac rehabilitation program[J]. J Cardiopulm Rehabil,1999,19(1):8-17.
[9] Binder E F,Yarasheski K E,Steger-May K,et al. Effects of progressive resistance training on body composition in frail older adults:results of a randomized,controlled trial[J]. J Gerontol A Biol Sci Med Sci,2005,60(11):1425-1431.
[10] Bottaro M,Machado S N,Nogueira W,et al. Effect of high versus low-velocity resistance training on muscular fitness and functional performance in older men[J]. Eur J Appl Physiol,2007,99(3):257-264.
[11] Brochu M,Savage P,Lee M,et al. Effects of resistance training on physical function in older disabled women with coronary heart disease[J]. J Appl Physiol,2002,92(2):672-678.
[12] Campbell W W,Crim M C,Young V R,et al. Increased energy requirements and changes in body composition with resistance training in older adults[J]. Am J Clin Nutr,1994,60(2):167-175.
[13] Candow D G,Chilibeck P D,Facci M,et al. Protein supplementation before and after resistance training in older men [J]. Eur J Appl Physiol,2006,97(5):548-556.
[14] Castaneda C,Gordon P L,Uhlin K L,et al. Resistance training to counteract the catabolism of a low-protein diet in patients with chronic renal insufficiency. A randomized,controlled trial[J]. Ann Intern Med,2001,4,135(11):965-976.
[15] Fatouros I G,Kambas A,Katrabasas I,et al. Resistance training and detraining effects on flexibility performance in the elderly are intensity-dependent[J]. J Strength Cond Res,2006,20(3):634-642.
[16] Figueroa A,Going S B,Milliken L A,et al. Effects of exercise training and hormone replacement therapy on lean and fat mass in postmenopausal women[J]. J Gerontol A Biol Sci Med Sci,2003,58(3):266-270.
[17] Greiwe J S,Cheng B,Rubin D C,et al. Resistance exercise decreases skeletal muscle tumor necrosis factor alpha in frail elderly humans[J]. FASEB J,2001,15(2):475-482.
[18] Haykowsky M,Humen D,Teo K,et al. Effects of 16 weeks of resistance training on left ventricular morphology and systolic function in healthy men>60 years of age[J]. Am J Cardiol,2000,85(8):1002-1006.
[19] Haykowsky M,McGavock J,Vonder Muhll I,et al. Effect of exercise training on peak aerobic power,left ventricular morphology,and muscle strength in healthy older women[J]. J Gerontol A Biol Sci Med Sci,2005,60(3):307-311.
[20] Igwebuike A,Irving B A,Bigelow M L,et al. Lack of dehydroepiandrosterone effect on a combined endurance and resistance exercise program in postmenopausal women[J]. J Clin Endocrinol Metab,2008,93(2):534-538.
[21] Kalapotharakos V I,Michalopoulos M,Tokmakidis S P,et al. Effects of a heavy and a moderate resistance training on functional performance in older adults[J]. J Strength Cond Res,2005,19(3):652-657.
[22] Kraemer W J,Häkkinen K,Newton R U,et al. Effects of heavy-resistance training on hormonal response patterns in younger vs. older men[J]. J Appl Physiol,1999,87(3):982-992.
[23] Miszko T A,Cress M E,Slade J M,et al. Effect of strength and power training on physical function in community-dwelling older adults[J]. J Gerontol A Biol Sci Med Sci,2003,58(2):171-175.
[24] Panton L B,Franke W D,Bleil D A,et al. Effects of resistance training on cardiovascular responses to lower body negative pressure in the elderly[J]. Clin Physiol,2001,21(5):605-611.
[25] Pu C T,Johnson M T,Forman D E,et al. Randomized trial of progressive resistance training to counteract the myopathy of chronic heart failure[J]. J Appl Physiol,2001,90(6):2341-2350.
[26] Reeves N D,Maganaris C N,Narici M V,et al. Effect of strength training on human patella tendon mechanical properties of older individuals[J]. J Physiol,2003,548(Pt 3):971-981.
[27] Reynolds T H 4th,Supiano M A,Dengel D R. Regional differences in glucose clearance:effects of insulin and resistance training on arm and leg glucose clearance in older hypertensive individuals[J]. J Appl Physiol,2007,102(3):985-991.
[28] Roth S M,Ivey F M,Martel G F,et al. Muscle size responses to strength training in young and older men and women[J]. J Am Geriatr Soc,2001,49(11):1428-1433.
[29] Sharman M J,Newton R U,Triplett-McBride T,et al. Changes in myosin heavy chain composition with heavy resistance training in 60-to 75-year-old men and women[J]. Eur J Appl Physiol,2001,84(1-2):127-132.
[30] Stewart K J,Bacher A C,Turner K L,et al. Effect of exercise on blood pressure in older persons:a randomized controlled trial[J]. Arch Intern Med,2005,165(7):756-762.
[31] Sward K. Effect of resistance exercise training on muscular strength, functional fitness, physical self-perception,and quality of life in the elderly[D]. University of Pittsburgh,PA,2001:186.
[32] Tarnopolsky M,Zimmer A,Paikin J,et al. Creatine monohydrate and conjugated linoleic acid improve strength and body composition following resistance exercise in older adults[J]. PLoS One,2007,2(10):e991.
[33] Tsutsumi T. The effects of strength training on mood,self-efficacy,cardiovascular reactivity and quality of life in older adults[D]. Boston University,Boston,MA,1997:171.
[34] Latham N K,Bennett D A,Stretton C M. et al. Systematic review of progressive resistance strength training in older adults[J]. J Gerontol A Biol Sci Med Sci,2004,59:48-61.
[35] American College of Sports Medicine Position Stand. Progression modelsin resistance training for healthy adults[J]. Med Sci Sports Exerc,2009,41:687-708.
[36] Chodzko-Zajko W J,Proctor D N. Exercise and physical activity for older adults[J]. Med Sci Sports Exerc,2009,41:1510-1530.
[37] Kerr D,Morton A,Dick I,et al. Exercise effects on bone mass in postmenopausal women are site-specific and load-dependent[J]. J Bone Miner Res,1996,11(2):218-225.
Meta analysis of the effects of resistance training on the muscle strength of the elderly
WANG Guang-ping1,ZHANG Kai-fa2
(1.Teaching and Research Division for Sport Medicine in the Physical Education and Health Education College,Mianyang Nornal University,Miangang 621000,China;2.The Campus Clinic,Mianyang Nornal University,Miangang 621000,China)
In order to evaluate the effects of resistance training on improving the muscle strength of the elderly, and to provide a criterion for establishing resistance training prescriptions, by basing their important literature sources on MEDLINE and PUBMED, searching literatures in relation to the effects of resistance training on the muscle strength of the elderly, published between 1990 and 2010, and selecting suitable literatures according to inclusion and exclusion standards, the authors evaluated their quality and extracted related data, and revealed the following findings after having performed a meta analysis on 30 literatures: after resistance training, the weighted mean difference of the maximum strength of the leg extensor group of the elderly was 6.78kg, the 95% credibility interval was 5.92~7.64 kg, the mean maximum strength increased by 24.2%; the weighted mean difference of the maximum strength of the leg flexor group was 1.03kg, the 95% credibility interval was 0.93~1.14 kg, the mean maximum strength increased by 20.3%; the weighted mean difference of the maximum strength of supine pushup was 11.52 kg, the 95% credibility interval was 10.74~12.29 kg, the mean maximum strength increased by 26.9%. The said findings indicated that resistance training is a means of intervention which can effectively improve the age-growth specific deterioration of the muscle strength of the elderly, and that high intensity resistance training can more effectively enhance the muscle strength of the elderly as compared with medium or low intensity resistance training.
sports medicine;resistance training;muscle strength;the elderly;meta analysis
王光平(1960-),女,副教授,研究方向:运动医学。
G804.5
A
1006-7116(2011)05-0132-07
2011-05-13
·竞赛与训练·
