Neutrophils in the tumor microenvironment: role in tumor progression and potential targeted therapeutic strategy
2024-05-18HongshuangShiSiqiYuWenshiLiXuejianLiXinWuXiujuanQuYiMaChunleiZhengXiaofangChe
Hongshuang Shi, Siqi Yu, Wenshi Li, Xuejian Li, Xin Wu, Xiujuan Qu, Yi Ma, Chunlei Zheng,Xiaofang Che
1Department of gynecology, The First Affiliated Hospital, China Medical University, Shenyang 110001, Liaoning, China.
2Department of Medical Oncology, Provincial Key Laboratory of Anticancer Drugs and Biotherapy of Liaoning Province, Clinical Cancer Research Center of Shenyang, The First Hospital of China Medical University, Shenyang 110001, Liaoning, China.
3Department of Hepatobiliary surgery, The First Affiliated Hospital, China Medical University, Shenyang 110001, Liaoning, China.
4Department of Otolaryngology, The First Affiliated Hospital of China Medical University, Shenyang 110001, Liaoning, China.
5Department of Oncology, Shanghai Electric Power Hospital, Shanghai 200050, China.
Abstract Neutrophils are known as the body's first line of defense against invading pathogens, which are the most abundant bone-marrow-derived innate immune cells accounting for 50%-70% of all white blood cells in human peripheral blood.With in-depth research in recent years, neutrophils have also been recognized as one of the main immune cells in the tumor microenvironment (TME), playing an important role in tumor development.Neutrophils can promote tumor metastasis through secretion of chemokines and cytokines and formation of neutrophil extracellular traps (NETs).Also, neutrophil targeting treatment has shown a promising anticancer effect.In this article, we summarized the recent research progress related to the significant role of neutrophils in tumor metastasis, as well as the current progression and limitations of targeting neutrophils in tumor therapeutics.This review can provide a comprehensive understanding of the role of neutrophils in the TME and the development of a new anticancer strategy.
Keywords: Neutrophils, metastasis, tumor microenvironment, targeting neutrophil
INTRODUCTION
Metastasis is the major cause of death in cancer patients.The “seed-soil” theory proposed by Steven Paget in 1889 described the basic mechanism of tumor metastasis that tumor cells as “seeds” can only colonize on the suitable microenvironment of the “soil” and grow to form foci of metastasis, but not randomly spread around[1].In fact, in both primary and metastatic sites, tumor cells, as well as immune cells, cancerassociated fibroblasts (CAFs), extracellular matrix (ECM), endothelial cells, and cytokines, constitute the complex tumor microenvironment (TME), which plays a significant role in tumor progression[2].
Among the immune cells in the TME, there are not only T cells, B cells, NK cells, and M1 macrophages that play antitumor roles, but also M2 macrophages, Treg cells, Th2 cells, and myeloid suppressor cells (MDSCs)that play immunosuppressive roles.In addition, there are a large number of neutrophils in the TME.However, the functional studies of neutrophils in the TME lagged far behind other immune cells, because neutrophils with short half-life have long been regarded as a single, terminally differentiated cell population that only acts as “bystanders” in the TME[3]; until recent years, with the deepening of TME research, more attention has been paid to the crucial role of neutrophils in the TME.Current studies have shown that,similar to macrophages, neutrophils can be polarized into different states under the stimulation of different microenvironments, which can play a dual role in promoting or inhibiting tumors.With tumor progression, neutrophils mainly play roles in promoting tumor growth, angiogenesis, extracellular matrix remodeling, and immunosuppression.Therefore, its high infiltration in tumor tissue is often closely related to poor prognosis[4].Recently, there has been a surge in studies focusing on neutrophil targeting therapy,which have shown promising anticancer effects, implying its potential as a new anticancer strategy[5-7].In this article, focusing on the role of neutrophils in tumor progression, especially in tumor metastasis, we reviewed the heterogeneity and plasticity of neutrophils, the related mechanisms that promote tumor metastasis, the role in tumor prognosis, and tumor therapy targeting neutrophils.
HETEROGENEITY AND PLASTICITY OF NEUTROPHILS
The neutrophils recruited to TME are called tumor-associated neutrophils (TANs).TANs were first identified as N1 and N2 by Fridlender in 2009, similar to tumor-associated macrophages (TAM) with heterogeneity and plasticity[3].The N1 TANs are characterized by cytotoxic and pro-inflammatory properties due to their production of intercellular adhesion molecule-1 (ICAM-1), factor-related apoptosis(FAS), reactive oxygen species (ROS), and tumor necrosis factor-α (TNF-α), whereas N2 TANs have strong immunosuppressive properties induced by secreting cytokines, chemokines, chemokine ligands, and matrix metalloproteinase (MMPs), promoting angiogenesis to contribute to tumor metastasis[3,8].Studies in mouse models of breast cancer have shown that the antitumor immunity in the metastatic niche (MN) is positively correlated with the proportion of N1/N2 TANs.Furthermore, a high N1/N2 TAN chemoattractant ratio,such as CXCL1/S100A8 ratio, was positively associated with a survival advantage in breast cancer[9].Increasing N1 TANs and their chemoattractants could enhance antitumor immunity and prevent lung metastasis of breast cancer.TANs can be polarized into antitumor or pro-tumor populations under the stimulation of different TMEs, that is, the phenotype and function of TANs change with tumor progression[10].Some factors, such as melanoma cell-neutrophil interactions, the stimulation of granulocyte colony-stimulating factor (G-CSF) and transforming growth factor (TGF-β), as well as colorectal cancerderived exosomal circular RNA (circRNA) circPACRGL, can trigger the transformation of TANs into a pro-tumor N2 phenotype[3,11-13], whereas Interferon-β (IFN-β), ACE inhibitor (ACEI), or angiotensinogen receptor 1 (AGTR1) antagonists can induce the polarization of TANs to the N1 phenotype[14,15].
Neutrophils can also be classified into low-density neutrophils (LDNs) and high-density neutrophils(HDNs), depending on their density[16].LDNs include immature and mature neutrophils, while HDNs are mature neutrophils.In the mouse models, LDNs can promote tumor growth when co-injected with tumor cells, showing functions of pro-tumor and immunosuppression, while HDNs play an antagonistic role against LDNs in cancer development and progression[10].Studies discovered that HDNs can transform into LDNs and acquire immunosuppressive activities by the stimulation of TGF-β[3].Interestingly, immature LDNs are specifically derived from bone marrow, while mature LDNs are considered to be converted from HDNs, suggesting two distinct sources of LDNs[10].However, the specific mechanism of these cells in cancer progression remains unclear.
In addition, a subtype of MDSCs has been found to express the markers of neutrophils, called polymorphonuclear myeloid-derived suppressor cells [PMN-MDSCs, also known as granulocyte-MDSCs(G-MDSCs)], acting as immunosuppressive neutrophils in tumor development[10].PMN-MDSCs highly express immunosuppressive factors such as inducible nitric oxide synthase (iNOS), arginase-1 (Arg-1), and indoleamine 2,3-dioxygenase (IDO) to inhibit T cell activation and effector function, ultimately promoting tumor progression[17].Additionally, G-MDSCs can highly express MMP-9, which can promote angiogenesis and ultimately promote tumor growth and metastasis[18].However, whether PMN-MDSCs are a separate lineage of immune cells, or merely immature neutrophils with an immunosuppressive phenotype, is currently unclear.
Thus, neutrophils are classified into different phenotypes according to polarization states, density, or markers.Although different phenotypes of neutrophils play dual functions, neutrophils are more likely to be polarized into tumor-promoting phenotype in tumor development, especially in the process of tumor metastasis [Table 1].The role of neutrophils in tumor metastasis is described in detail below.
THE DIRECT EFFECTS OF NEUTROPHILS ON TUMOR CELLS
Metastasis is a cascade process by which the tumor cells disseminate from the primary locations, enter the blood and/or lymphatic system (intravasation), exit from circulation (extravasation), and finally colonize distant organs.Neutrophils can promote tumor metastasis at each of the aforementioned stages [Figure 1].
Neutrophils in tumor cell dissemination
Epithelial-mesenchymal transformation (EMT) is a process by which epithelial cells acquire mesenchymal fibroblast-like morphology and lose their intercellular adhesion property and show enhanced motility, and is the most studied mechanism related to tumor cell dissemination.Neutrophils have been proved to be able to induce EMT of tumor cells in various cancers, including lung cancer, breast cancer, gastric cancer, oral squamous cell carcinoma, colorectal cancer, ovarian cancer, and other cancers[19-23].For example,neutrophils could induce EMT of lung cancer cells through TGF-β/Smad and JNK-ZEB1/Snail signaling pathways, trigger EMT of gastric cancer cells by activating JAK2/STAT3 signaling pathway by secreting IL-17a, and induce EMT of breast cancer cells by secreting tissue inhibitors of matrix metalloproteinase 1(TIMP-1)[24-26].
Neutrophils in tumor cell intravasation
Tumor cells need to infiltrate blood vessels to reach distal organs to form metastasis, and neutrophils can promote tumor cell intravasation by weakening the endothelial cell barrier.The increased level ofcomplement activation product C5a near tumor blood vessels promotes the recruitment of neutrophils;then, upon contact with vascular endothelium, neutrophils are further activated by the complement membrane attack complex (MAC); finally, the activated neutrophils secrete ROS to enhance vascular permeability and promote the infiltration of melanoma cells into the circulatory system[27].However, related research remains sparse and the molecular mechanisms warrant further exploration.
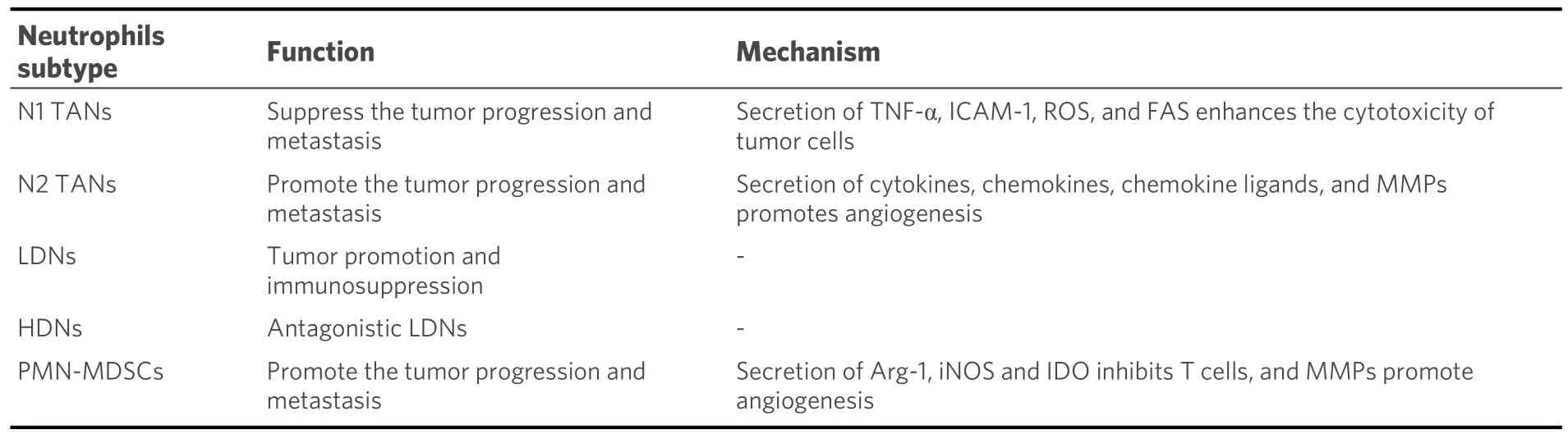
Table 1.Main function and mechanism of TANs, LDNs, HDNs and PMN-MDSCs
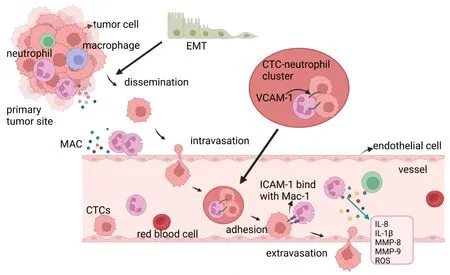
Figure 1.Neutrophils induce EMT of tumor cells, leading to the dissemination from the primary tumor site; Mac-activated neutrophils increase vascular permeability and promote intravasation of tumor cells.Neutrophils and CTCs form CTC-neutrophil clusters mediated by VCAM-1, which escort CTCs.Neutrophil-secreted cytokines such as IL-8, IL-1β, MMP-8, MMP-9, and ROS weaken the endothelial barrier and promote extravasation.The Mac-1 expression on the surface of neutrophils interacts with the ICAM-1 expression of CTCs to enhance adhesion and extravasation of tumor cells.EMT: Epithelial-mesenchymal transformation; CTCs: circulating tumor cells; MAC:membrane attack complex; VCAM-1: vascular cell adhesion molecule-1; ICAM-1: intercellular adhesion molecule-1.Created in BioRender.com.
Neutrophils promote the survival of CTCs
The tumor cells shedding into the blood from the primary site, known as circulating tumor cells (CTCs), are the seeds for metastasis, and their survival is a prerequisite for successful metastasis.However, CTCs continuously suffer from the continuous impact of fluid shear force, oxidative stress, and immune cellkilling, so only a few CTCs can eventually reach the distal organs for colonization[28].Neutrophils can interact with CTCs to form CTC-neutrophil clusters mediated by vascular cell adhesion molecule-1(VCAM-1), aiding in CTC survival and even and even stimulating proliferation by promoting cell cycle progression in the blood vessels[8].By analyzing blood samples from 70 patients and 5 mouse models of breast cancer, Szczerbaet al.found that the majority of leukocytes escorting circulating breast cancer cells were neutrophils (85.5%-91.7%), and depleting the neutrophils with neutralizing antibodies leads to a delayed metastasis.They also found that the mouse injected with CTCs from CTC-neutrophil clusters developed metastasis much more quickly than those injected with CTCs alone, mirrored by a shorter overall survival (OS)[8].
Neutrophils in extravasation of tumor cells
After homing to the vicinity of metastatic sites, the ability of CTCs in terms of extravasation from blood vessels and rapid penetration of surrounding tissues determines their metastatic potential.Although the exact mechanism of extravasation remains unclear, several studies have shown that changes in endothelial cell morphology and increased permeability can promote the extravasation of CTCs.The cytokines secreted by neutrophils such as IL-8, IL-1β, MMP-8, MMP-9, and ROS can disrupt extracellular matrix components,resulting in the weakness of endothelial barrier function and the following increase in transendothelial migration, ultimately accelerating the extravasation of tumor cells[29-31].
In addition, neutrophils can also promote the extravasation of tumor cells by enhancing their adhesion ability.Mac-1 is highly expressed on the surface of neutrophils, which mainly binds to intercellular adhesion molecule-1 (ICAM-1) expressed on cancer cells.Spiceret al.found that the interaction between Mac-1 of neutrophils and ICAM-1 expressed on CTCs enhanced the adhesion of tumor cells in hepatic sinuses and promoted liver metastasis[32].Neutrophils secrete IL-8 to acquire the capacity to recruit and infiltrate tumor sites; the infiltrated neutrophils further induce tumor cell extravasation and metastasis under the action of ICAM-1.In vivozebrafish models show similar patterns of migration and extravasation behaviors as observed after neutrophil-tumor cells were co-injected into the embryonic vasculature[29].
NEUTROPHILS INDIRECTLY PROMOTE METASTASIS
The interaction between neutrophils and other immune cells
The interaction between neutrophils and other immune cells in the TME promotes tumor metastasis by establishing an immunosuppressive microenvironment.Previous studies show that neutrophils cause immune escape by inhibiting the function of T cells, and lead to tumor progression by regulating the activities and recruitment of both NK cells and macrophages [Figure 2][33].
Germannet al.found that among different types of bone marrow cells in mouse models with colon cancer,neutrophils were the most potent inhibitor of T-cell activity in the TME[34].The secretion of MMPs by neutrophils can inhibit the functions of T cells by activating TGF-β in the TME[34].The ROS, Arg-1, and iNOS produced by neutrophils can directly suppress CD8+cytotoxic T lymphocytes (CTLs)[35-37].Moreover,the crosstalk between the programmed death ligand-1 (PD-L1) overexpressed on neutrophils and programmed cell death protein 1 (PD-1) expressed on T cells exhibits a greater suppressive role in T cell immunity, which could be reversed by PD-L1 blocking[38].NK cells play an important role in antitumor metastasis, but the increase in neutrophils at the metastasis site can inhibit the activation of NK cells to remove their tumor-cell-killing ability[30].The ROS released from neutrophils kills NK cells, and targeting the ROS pathway in neutrophils eliminates the pro-metastatic role of neutrophils[39,40].Neutrophils can also recruit macrophages and Treg cells into the TME to promote the development of hepatocellular cancer[41].Conversely, the depletion of neutrophils could attenuate macrophage recruitment and T cell suppression[42].
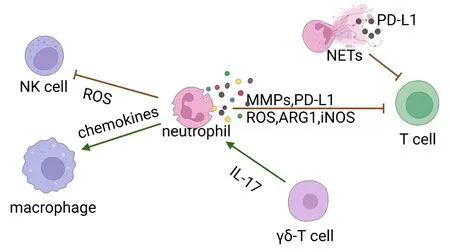
Figure 2.Neutrophils secreted ROS to inhibit NK cell function; TANs recruit phagocytes by secreting chemokines; Neutrophils suppress the T cell immunity by secreting MMPs, ROS, ARG1, and iNOS.IL-17 secreted by γδ-T cells promotes neutrophil recruitment.Neutrophils inhibit T cell function by expressing PD-L1, and some PD-L1 can be embedded in NETs.ROS: reactive oxygen species;MMPs: matrix metalloproteinase; Arg-1: arginase-1; iNOS: inducible nitric oxide synthase; NETs:neutrophil extracellular traps; PD-L1:programmed death ligand-1; TANs: tumor-associated neutrophils.Created in BioRender.com.
The formation of the premetastatic niche
In 2005, Kaplanet al.first proposed that the primary tumor is able to affect distant sites by promoting the formation of supportive metastatic environments, which was termed the premetastatic niche (PMN)[43].The accumulation of neutrophils and neutrophil-derived molecules is thought to contribute to immunosuppression, angiogenesis, and extracellular matrix remodeling in the distal organs, thereby promoting the formation of PMN [Figure 3].In the mouse models of breast cancer metastasis, Wculeket al.found that neutrophils increase in lung before cancer cells infiltration[44].Moreover, neutrophils in PMN have been shown to secrete leukotrienes that enrich metastasis-initiating cells which retain high tumorigenic potential[44].Primary tumor-derived elements are the main “culprits” in PMN formation.In mouse models of melanoma metastasis, primary tumor-derived exosomes are enriched in small nuclear RNAs, which are potential ligands for toll-like receptor 3 (TLR3), and activate TLR3 in alveolar type II epithelial cells, causing secretion of chemokine (CXCL1, CXCL2, CXCL5, and CXCL12) and initiating neutrophils recruitment in the lung[45].Additionally, Zhenget al.found that under the influence of Th2 cytokines (such as IL-4 and IL-13), lung interstitial stromal cells are activated to express high levels of C3,thus promoting neutrophils recruitment and subsequent lung metastasis.However, how the primary tumor induces Th2 cytokine secretion remains to be explored[46].In the PMN, neutrophils can secrete other metastasis-promoting factors, including MMP-9, chemokines S100A8 and S100A9, NE, cathepsin G, proinflammatory cytokines IL-1β, TNF-α, IL-12, and leukotriene B4 (LTB4)[47].In addition, neutrophils can also induce angiogenesis in PMN by secreting VEGF and Bv8[48,49].
NEUTROPHIL EXTRACELLULAR TRAPS, NETS
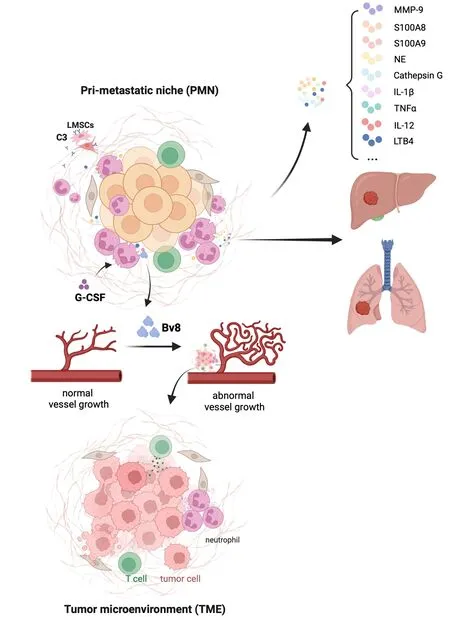
Figure 3.Neutrophils secrete MMP-9, S100A8, S100A9, NE, Cathepsin G, IL-1β, TNF-α, IL-12, and leukotriene B4(LTB4) in PMNs to promote metastasis.Neutrophils secrete vascular endothelial growth factor (VEGF) and Bv8 to promote angiogenesis in PMN.TNF-α:tumor necrosis factor-α; PMN: premetastatic niche; EMT: Epithelial-mesenchymal transformation; CTLs: cytotoxic T lymphocytes;LMSCs: lung interstitial stromal cells; G-CSF: granulocyte colony-stimulating factor; Bv8: bombina variagata peptide 8.Created in BioRender.com.
In addition to secreting cytokines and chemokines, the formation of neutrophil extracellular traps (NETs)also promotes metastasis.In 2004, Brinkmann first described NETs as the extracellular networks released by neutrophils, which consisted of nuclear DNA, specifically modified citrullinated histones and cytoplasmic degradative enzymes (including elastases, MMPs, and myeloperoxidase)[50].Numerous studies in recent years have found that NETs are also vital in facilitating metastasis and establishing an immunosuppressive microenvironment[51][Figure 4].
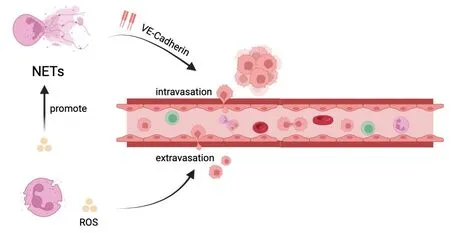
Figure 4.NETs participate in the cascade process of tumor metastasis.NETs induce EMT of tumor cells and enhance the migration ability.NETs trap tumor cells and protect them from CTLs and NK cells.NETs: neutrophil extracellular traps; ROS: reactive oxygen species; EMT: epithelial-mesenchymal transformation; CTLs: cytotoxic T lymphocytes; NK cells: natural killer cells; TGF-β: transforming growth factor.Created in BioRender.com.
Firstly, NETs can participate in the tumor metastasis cascade.NETs may induce the intravasation of tumor cells by the downregulation of VE-cadherin on endothelial cells, which can destroy the integrity of tumor vasculature[52].NETs can capture CTCs, preventing them with physical and immune barriers from the attack of CTLs and NK cells.Teijeiraet al.discovered that when tumor spheroids were co-cultured with NK cells or CD8+T cells, NET-coated tumor spheroids grew much larger than those without NET coating[53].Notably, NETs not only entrap CTCs but also interact with CTCs via receptors on the membrane to improve the abilities of adhesion to distant organ sites and motility of CTCs, such as integrin β1, a coiledcoil domain-containing 25 (CCDC25)[54,55].In obese tumor-bearing mice, ROS production by neutrophils promotes the formation of NETs, which can weaken endothelial junctions and promote extravasation of CTCs[31].
Secondly, NETs can also stimulate EMT, which leads to increased migration and invasion of cancer cells to distant organs[56].Stehret al.found that NETs could induce the formation of filopodia and promote the cell motility of colorectal cancer cells, which was associated with the increased expression of mesenchymal markers mRNA [vimentin (Vim), fibronectin (FN1)] and EMT-promoting transcription factors [ZEB1, Slug(SNAI2)] and decreased expression of epithelial markers E-cadherin and epithelial cell adhesion molecules[56].NETs transformed the typical epithelial morphology of breast cancer cells into mesenchymal morphology characterized by increased expression of N-cadherin and FN and decreased expression of Ecadherin, which ultimately led to enhanced migratory capacity[57].Furthermore, it has been established that NETs could induce EMT of tumor cells in gastric cancer and pancreatic cancer[58,59].
NETs are also involved in the formation of PMN.Previous studies found that the presence of NETs in the peritoneum and omentum contributes to PMN formation[60,61].At present, this mechanism has been proposed to explain the colonization of target organs by different types of cancers, such as omentum colonization by ovarian cancer and liver colonization by colorectal cancer[60,62].
NETs modulate tumor immune escape.NETs wrap and coat tumor cells, blocking their contact with other immune cells and surrounding target cells[53].In addition to providing a physical barrier, NETs can also impair the antitumor function of immune cells.For example, NETs can induce the exhaustion and dysfunction of CD8+T cells[63].The PD-L1 can be embedded in NETs, thereby inhibiting T cell function by binding to PD-1 on the surface of the T cells[63].NETs can also impair the tumorilytic function of NK cells by increasing the secretion of TGF-β.
CLINICAL VALUE OF NEUTROPHILS
Due to the ease of obtainment and calculation, the peripheral blood NLR has long been considered a potential biomarker for tumors.The neutrophil to lymphocyte ratio (NLR) is known to increase in many types of tumors including sarcoma, and is closely related to a shorter OS, disease-free survival, or progression-free survival[64-68].The high NLR has been considered a biomarker of poor clinical outcomes in gastric, triple-negative breast, colorectal, pancreatic, thyroid, and ovarian cancers and soft tissue sarcoma[69-76].Moreover, the results of a recent study about sarcomas indicate that high NLR may be associated with chemoresistance[77].Notably, several studies have found that high NLR is also an independent predictor of metastasis.For example, high NLR is associated with brain metastasis of nonsmall-cell lung cancer[78].Colorectal cancer patients with high NLR before operation are more likely to develop liver metastasis than those with low NLR[79].The peritoneal cancer index (PCI) is used to assess peritoneal metastasis of gastric cancer, with higher PCI indicating either more extensive or larger tumors(or both) in the peritoneal cavity.Recent studies showed that the NLR was an independent predictor of a higher PCI in gastric cancer patients with peritoneal metastasis[80].Moreover, the elevated NLR can also predict inguinal lymph node metastasis of penile squamous cell carcinoma[81].
In clinical practice, the key role of peripheral blood NLR in screening patients suitable for immunotherapy and evaluating its efficacy is also attracting increasing attention.The prognostic value of NLR has been demonstrated in immune checkpoint inhibitor (ICI) therapy and NLR has also been identified as a biomarker associated with ICI treatment outcome, which has been reported in various cancers, such as lung cancer, kidney cancer, and melanoma[82,83].Linet al.proposed that patients might be more amenable to treatment with ICI if they have a lower NLR level in peripheral blood, because of more infiltrating CD8+T cells in their tumors[84].Liet al.showed that NLR < 5 at baseline and on-treatment was significantly associated with improved OS in advanced cancers treated with ICI[85].
The high NLR ratio is usually manifested by the presence of a large number of circulating neutrophils in the blood and often leads to elevated TAN levels of infiltration in the TME.However, at present, many studies evaluating the correlation of neutrophils with cancer prognosis mainly focus on peripheral blood neutrophils rather than TANs, which is mainly due to the challenges in assessing the number and subsets of TAN infiltrates.In hepatocellular carcinoma, Heet al.revealed that the expression of PD-L1 in both intra and peri-tumor neutrophils is elevated beyond the levels observed in circulating neutrophils, suggesting that TAN infiltration may have a stronger ability to predict the therapeutic effect of ICI[86].In the pancreatic ductal adenocarcinoma, Liet al.found that higher densities of TAN following nivolumab portend a poorer OS[87].However, there was no significant difference in intratumoral neutrophil counts in melanoma patients treated with nivolumab compared with non-users[88].
NEUTROPHIL TARGETING FOR TUMOR IMMUNOTHERAPY
At present, a large number of preclinical studies and clinical trials have evaluated the efficacy and safety of neutrophil targeting in tumor treatment.The relevant mechanisms mainly include the inhibition of neutrophil activities, recruitment, induction of polarization, targeting NETs, and combining the aforementioned tactics with other antitumor medications [Table 2].
Directly targeting neutrophils
Inhibition of neutrophil survival and recruitment
CXCR1 and CXCR2 are the major chemokine receptors expressed on the surface of neutrophils, and neutrophils can mainly be recruited into TME by chemokines, especially CXCL8.Therefore, targeting CXCLs/CXCR1/2 signaling axis has been identified as a powerful strategy for tumor therapy[95].Using the CXCR2-specific antagonists or blocking of CXCR2 by gene knockdown can significantly suppress the growth and metastasis of breast and ovarian cancer; similarly, a CXCR2-specific inhibitor (SB225002) could inhibit the metastasis of gliomain vitro[96-98].SX-682, an oral CXCR1/2 small molecule antagonist, had been shown to inhibit the recruitment of PMN-MDSCs in mouse oral, lung and prostate cancer models[99,100].A Phase I clinical trial of melanoma is exploring whether SX-682 can inhibit MDSC recruitment in tumors,which is ongoing at the time of writing (NCT03161431).In fact, there are still many clinical trials of SX-682 in non-small cell lung cancer, pancreatic cancer, and lung cancer underway at the time of writing.A Phase II clinical trial of CXCL8 specific inhibitor Reparixin in HER-2 negative metastatic breast cancer exerted a positive effect with the combination of paclitaxel[89].DS-8273A is an agonistic antibody against TRAIL receptor 2 (TRAIL-R2), which can induce apoptosis of tumor cells[101].Targeting TRAIL-R has been shown to cause the exhaustion of MDSCs in mice[102].The results of a Phase I clinical trial that evaluated the antitumor effect of DS-8273A showed that DS-8273A could eliminate PMN-MDSCs and extend progression-free survival.However, the inhibitory effect of DS-8273A on PMN-MDSCs could not be sustained in the long term, and returned to the pre-treatment level on the 42nd day after treatment[101].At present, the clinical development of DS-8273A is almost at a standstill.
Besides, colchicine compounds and Del-1 were also reported to be able to inhibit the recruitment of neutrophils.Chenet al.found that low-toxicity colchicine derivatives (BCS) modified with sialic acid and cholesterol derivatives (SA-CH) can be absorbed by neutrophils, reducing neutrophilic infiltration, resulting in suppression of cell migration and imparting an effective antitumor effect[103].In mouse colon cancer models, Tianet al.used the engineered Salmonella delivering Del-1 (a potent inhibitor of neutrophil recruitment) to enhance the anticancer activity by decreasing tumor-infiltrating neutrophils[104].
Reprogramming neutrophils into an antitumor phenotype
Reprogramming pre-tumor neutrophils into antitumoral phenotypes is considered another strategy for neutrophil targeting.In mouse models, a new nano-vaccine can polarize N2 neutrophils in the TME to the N1, which causes 83% of the tumors to regress completely and extends survival[105].Furthermore, STAT3 has been proved to be involved in the polarization of neutrophils in N2 populations[106].Tyagiet al.found that nicotine induced neutrophil polarization through a STAT3-dependent pathway, thereby promoting brain metastasis in lung cancer.However, the small molecule STAT3 inhibitors (STAT3i, SH-4-54) could suppress the polarization of nicotine-induced STAT3-mediated neutrophils, thereby eliminating brain metastasis[107].
Since the pro-tumor activity of neutrophils can be reversed to an antitumor role with TGF-β blockade,enhancing the tumor-killing activity of neutrophils by inhibiting TGF-β is considered a potential tumor therapeutic strategy[108].Anti-TGF-β (1D11) treatment increased the cytotoxicity of neutrophils and reduced the secretion of metastatic chemokines, suppressing tumor cell migration[109].Galunisertib (LY2157299), a small molecule inhibitor of TGF-β receptor 1 kinase, has significant antitumor activities in mouse glioblastoma models.A Phase II clinical trial in pancreatic cancer with the combination of Galunisertib and ICI has demonstrated increased infiltration of CD8+T cells in the tumor, with a 25.0% disease control rate.In addition, Galunisertib also achieved clinical effects in a series of clinical trials including glioblastoma,hepatocellular carcinoma, non-small cell lung cancer, and rectal cancer[93,94,110].At present, Galunisertib is considered a promising potent drug at the stage of clinical development.Moreover, based on the regulatory effects on immunosuppressive microenvironment, ICI resistance and sensitivity, more than 10 types of TGF-β inhibitors have been tested in clinical trials for cancer treatment, which have broad prospects in the treatment of tumors.Certainly, whether their effects really depend on neutrophils remains to be explored.
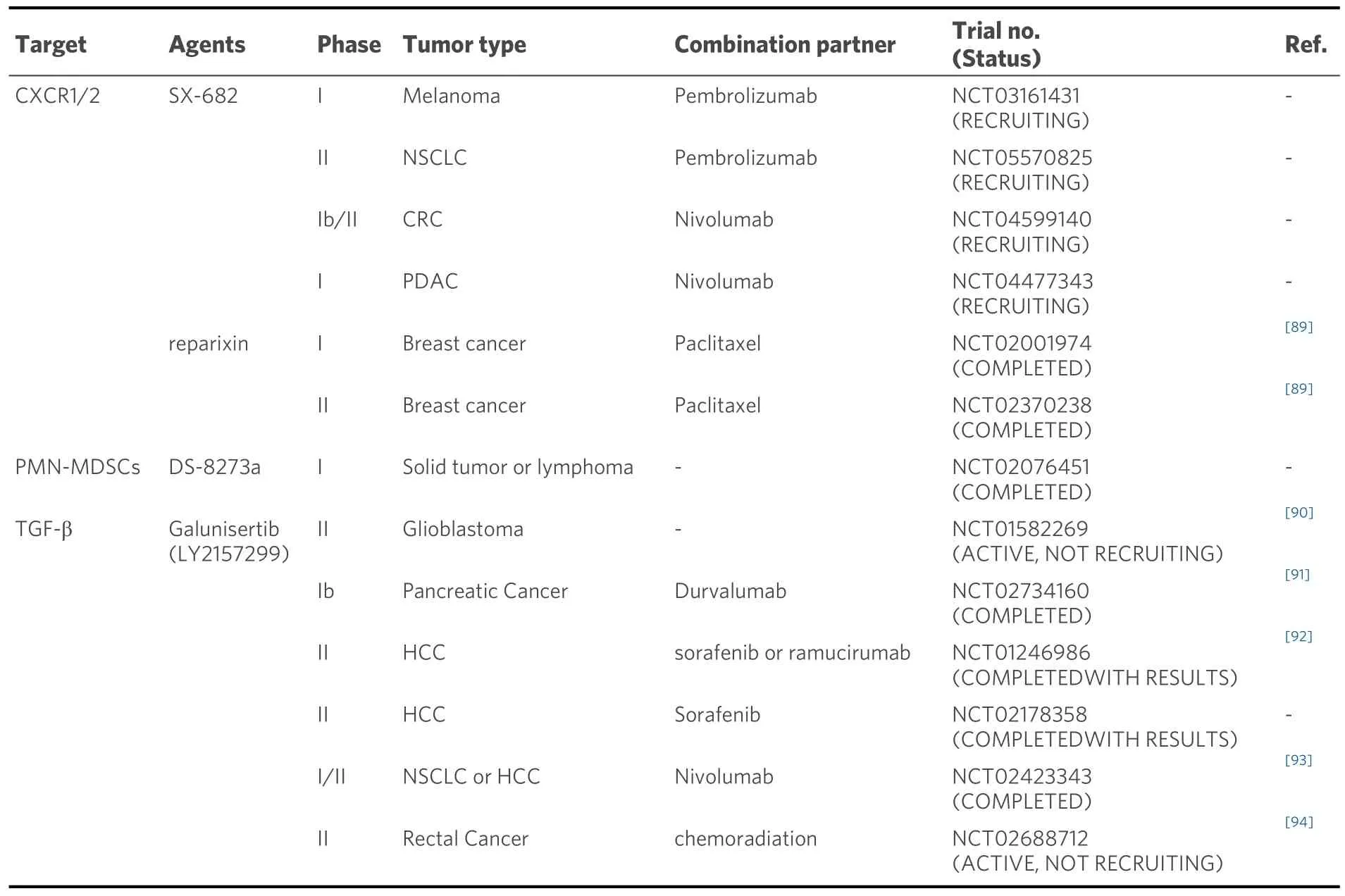
Table 2.Clinical trials of agents targeting neutrophils
In addition, knockout or knockdown of IFN-β can stimulate the production of pro-tumor neutrophils with elevated expression levels of VEGF, MMP-9, and CXCR4, whereas a low dose of IFN-β treatment can restore the expression of pro-angiogenic factors to control levels[14,111].Similarly, low-dose IFN-β treatment of tumor-bearing mice resulted in neutrophil polarization into antitumor N1 phenotype, characterized by increased FAS and TNF-α expression and elevated antitumor cytotoxicity[14].However, there are currently no related clinical trials of IFN-β for cancer treatment.
In general, studies directly targeting the inhibition of neutrophil activity and recruitment and functional reprogramming remain sparse.In the future, more preclinical studies and clinical trials are needed.
Targeting NETs
Targeting NETs, mainly including directly destroying the structure of NETs or interfering with the formation of NETs, is also considered a promising approach to tumor treatment.The deoxyribonuclease enzyme (DNase), which can break down the structure of NETs by degrading free DNA, has shown therapeutic benefits in multiple tumor models[112].DNaseI treatment significantly decreased the metastasis ability of breast cancer cells; treatment with DNaseI also significantly inhibited liver and lung metastases in mice[51,113,114].Peptidyl arginine deaminase 4 (PAD4) is a key enzyme involved in the release of NETs into extracellular domains.In vitro, Zhuet al.confirmed that DNaseI and PAD4 inhibitors could effectively suppress the formation of NETs, thereby inhibiting EMT of tumor cells and ultimately inhibiting migration[58].However, there are no clinical trials involving the targeting of NETs.
Moreover, clinically available drugs may also be used for anti-NET therapy.Autophagy is the key means of NET formation.When treated with autophagy inhibitors, the formation of NETs in circulation and TME was suppressed in pancreatic cancer.Those such as chloroquine can reverse the tendency to form NETsin vitro[115].Another autophagy inhibitor, hydroxychloroquine, may also exhibit the same activity[116].These drugs are expected to be further validated for their ability to suppress the formation of NETs.
Combination therapy
At present, the combination of drugs with different mechanisms of action is a key method by which to improve the therapeutic effect of cancer, such as the combination of immunotherapy with chemotherapy or radiotherapy, and the combination of multiple immunotherapy strategies, which can not only enhance drug sensitivity, but also overcome resistance.The combination of targeting neutrophils with ICI and conventional chemotherapy has demonstrated efficacy in several cancer studies [Table 2].
Combination of neutrophil inhibitors and immune checkpoint inhibitors
The use of ICIs may have brought new hope for cancer treatment in recent years, but not all patients respond to ICI clinically.ICI is usually effective in hot tumors (highly T-lymphocyte infiltrating), while neutrophils play an immunosuppressive role in T-cell immunity.Therefore, the efficacy of ICI is markedly reduced in tumors rich in neutrophils in the TME[117].Studies have confirmed that targeting neutrophils can improve the efficacy of ICI.For example, CXCR1/2 inhibitors can significantly improve the efficacy of anti-PD-1 immunotherapy[118].In xenograft tumor models, the combination of CXCR2 inhibitors and anti-PD-1 significantly extended the survival[119].Highfillet al.have also found that immunotherapy efficacy was restored by suppressing CXCR2 in mouse models of soft tissue sarcoma resistant to anti-PD-1 therapy[120].Lorlatinib is an oral tyrosine kinase inhibitor that can inhibit neutrophil recruitment.When lorlatinib was combined with anti-PD-1, there was a significant decrease in neutrophils and an increase in CD8+T cells in mouse tumors, suggesting that lorlatinib may improve tumor responsiveness to ICI by inhibiting neutrophils[121].Cabozantinib is also a tyrosine kinase inhibitor that can inhibit the function of neutrophils.The preliminary results of Cabozantinib in combination with PD-1/PD-L1 or CTLA-4 antibodies are also effective in the treatment of cancer[122].
Combination of neutrophil inhibitors and chemotherapy
The combination of neutrophil targeting with chemotherapy may be another effective synergistic treatment strategy.A preclinical study demonstrated that CXCR2 inhibitor combined with cisplatin significantly reduced neutrophil infiltration and enhanced antitumor activity of CD8+T cells, showing a significant therapeutic effect in mouse lung cancer models[123].Similarly, CXCR2 inhibitors combined with gemcitabine significantly can also improve the OS of mouse pancreatic ductal adenocarcinoma models[119].
CONCLUSION AND PERSPECTIVES
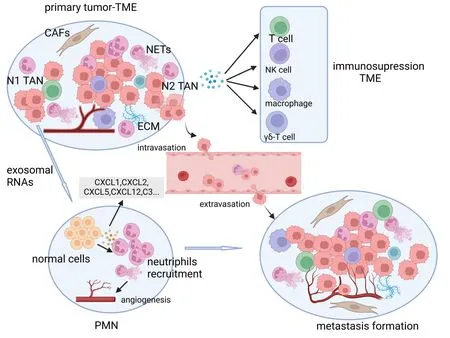
Figure 5.Neutrophils and the NETs released thereby provide a protective microenvironment for tumor growth and metastasis.They participate in the cascade process of metastasis and the formation of PMN.NETs: neutrophil extracellular traps; PMN: premetastatic niche; TME: tumor microenvironment; ECM: extracellularmatrix; CSFs: colony stimulating factors; CAFs: cancer-associated fibroblasts;N1 TAN: tumor-associated neutrophil; exosomes RNAs: exosomes ribonucleic acid.Created in BioRender.com.
As an important part of the TME, neutrophils are a new agent active in tumor development, which provide a protective microenvironment for tumor growth and metastasis [Figure 5].The high plasticity and diversity of neutrophils offer a new idea for tumor treatment.During the process of tumor metastasis,neutrophils and the NETs released thereby can induce EMT of tumor cells and help tumor cells escape from the primary sites to complete the first step of tumor metastasis.In blood vessels, neutrophils and tumor cells form the clusters or NETs wrap them directly, providing a powerful “protective shield” for tumor cells to cope with attack from the surrounding environment.In addition, both neutrophils and NETs are involved in the formation of PMN, and their complex interactions with lymphocytes, macrophages, and NK cells constitute an immunosuppressive microenvironment, which is closely related to the formation of metastasis.
Although most experimental work showed that targeting neutrophils has a clear inhibitory effect on tumors,most research is limited to basic studies.In the course of research, there are still many problems that need to be addressed; for example, how to target N2 neutrophils without affecting N1 neutrophils or specifically induce neutrophils to antitumor phenotypes? Theoretically, inhibition of TGF-β can induce neutrophils into the antitumor N1 phenotype; however, Fanget al.found that non-small cell lung carcinoma mice with TGF-β1 knockout had larger tumors than wild-type mice, while 1D11 (a TGF-β inhibitor) can suppress the growth of tumor.They hypothesized that knockout of TGF-β1 might impart an overall immunosuppressive effect and promote tumor development, possibly contributing to the multifunction of TGF-β1[124].Therefore,does suppression of TGF-β actually impart an antitumor effect in clinical practice? Although specific reduction of neutrophils in peripheral blood and TME can suppress tumor progression, it may expose patients to opportunistic infection and give rise to the question of how to reduce the occurrence of infections during treatment.NETs, as described above, trap cancer cells isolated from the primary tumor,acting as a “physical barrier” to protect them during metastasis.Does this “physical barrier” limit the proliferation of tumor cells to some extent? How do CTCs break this barrier when they exude blood vessels?Although most of the current experiments found that targeting NETs can inhibit the metastasis of tumor cells, a small number of studies have shown that NETs can inhibit the growth and migration of cancer cells and induce cell apoptosis[125,126].The mechanism of interaction between NETs and tumor cells remains to be explored.Currently, high NLR is associated with poor clinical outcomes in a variety of tumors, especially as recent studies have found that it can be used to assess the efficacy of ICIs therapy.Is the TAN infiltration density in the TME a more accurate predictor of ICI efficacy? Moreover, does the increase of neutrophils in peripheral blood necessarily lead to the increase of TAN in the TME, and can the evaluation effect of the two be consistent? Which fraction of neutrophils in the peripheral blood is recruited to the TME to play a pro-tumor role? How are these neutrophils detected? In addition, is the predictive effect of TANs still accurate under different inflammatory states of tumor tissues? Does the time (from biopsy/surgery to medication) to detect the TAN infiltration density affect the predicted outcome? Like ICIs, targeting neutrophils may also disrupt the body’s immune tolerance balance and cause systemic immune injury, such as drug-induced liver injury (DILI), but these issues also warrant investigation.
In conclusion, the mechanism of neutrophil-induced tumor metastasis and possible targeted therapies was reviewed.With the deepening of the study of the interaction mechanism between neutrophils and tumors,targeting neutrophils will undoubtedly usher in a new era of tumor therapy, but there are still many problems yet to be explored.This review is expected to provide ideas for further research.
DECLARATIONS
Authors’ contributions
Literature search and writing original draft: Shi H
Conceptualization, manuscript review and editing: Che X, Zheng C, Ma Y
Literature search, figures, and tables: Yu S, Li W
Literature search, language modification: Li X, Wu X, Qu X
Availability of data and materials
Not applicable.
Financial support and sponsorship
This review was supported by National Natural Science Found ation of China (No.32170791); the highquality development of science and technology funding projects at China Medical University (2022JH2/20200039); “China Medical University-Chinese Academy of Sciences Shenyang Branch Scientist Partner”project (HZHB2022002); and Guozhong Health Group Science and Technology Project (GZKJ-KJXXQTHT-20230425).
Conflicts of interest
Xiaofang Che is an Editorial Board member of the journal Journal of Cancer Metastasis and Treatment.The other authors declare that there are no conflicts of interest.
Ethical approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Copyright
© The Author(s) 2024.
杂志排行
Journal of Cancer Metastasis and Treatment的其它文章
- ImmuneScore as a novel RNA-based prognostic signature superior to PD-L1 in advanced nonsquamous NSCLC patients receiving chemotherapy combined with immune checkpoint inhibitor therapy
- Research progress of intestinal microbiota in targeted therapy and immunotherapy of colorectal cancer
- Research advances in immunotherapy combined with DNA damage response inhibitors for liver cancer therapy