Whole-process case management effects on mental state and selfcare ability in patients with liver cancer
2024-05-07ManDiJuQinQinMengLi
Man-Di Ju,Qin Qin,Meng Li
Abstract BACKGROUND Regarding the incidence of malignant tumors in China,the incidence of liver cancer ranks fourth,second only to lung,gastric,and esophageal cancers.The case fatality rate ranks third after lung and cervical cancer.In a previous study,the whole-process management model was applied to patients with breast cancer,which effectively reduced their negative emotions and improved treatment adherence and nursing satisfaction.AIM To explore Mental state and self-care ability in patients with liver cancer: effects of whole-process case management.METHODS In this single-center,randomized,controlled study,60 randomly selected patients with liver cancer who had been admitted to our hospital from January 2021 to January 2022 were randomly divided into an observation group (n=30),who received whole-process case management on the basis of routine nursing measures,and a control group (n=30),who were given routine nursing measures.We compared differences between the two groups in terms of anxiety,depression,the level of hope,self-care ability,symptom distress,sleep quality,and quality of life.RESULTS Post-intervention,Hamilton anxiety scale,Hamilton depression scale,memory symptom assessment scale,and Pittsburgh sleep quality index scores in both groups were lower than those pre-intervention,and the observation group had lower scores than the control group (P < 0.05).Herth hope index,self-care ability assessment scale-revision in Chinese,and quality of life measurement scale for patients with liver cancer scores in both groups were higher than those pre-intervention,with higher scores in the observation group compared with the control group (P < 0.05).CONCLUSION Whole-process case management can effectively reduce anxiety and depression in patients with liver cancer,alleviate symptoms and problems,and improve the level of hope,self-care ability,sleep quality,and quality of life,as well as provide feasible nursing alternatives for patients with liver cancer.
Key Words: Liver cancer;Mental state;Self-care ability;Whole-process case management;Life quality;Nursing
lNTRODUCTlON
In terms of global cancer rankings,liver cancer ranks sixth in incidence and second in terms of case fatality rate.In males,the incidence of liver cancer ranks fifth and the case fatality rate ranks second,while the incidence of liver cancer in women ranks ninth and the case fatality rate ranks sixth[1].Regarding the incidence of malignant tumors in China,the incidence of liver cancer ranks fourth,second only to lung,gastric,and esophageal cancers.The case fatality rate ranks third after lung and cervical cancer.The incidence and mortality rates for liver cancer in males with malignant tumors are both ranked third.The incidence rate in females with malignant tumors is ranked sixth,and the case fatality rate is ranked fourth[2].The incidence and mortality rates for liver cancer in China is higher than those of other countries,accounting for > 50% of the total number of patients with liver cancer globally[3,4].
Patients with liver cancer are likely to face different dilemmas and have differing psychological states at various stages of the disease.A definitive diagnosis of liver cancer can be a significant trauma for patients,with patients and their families often unable to cope for a certain period of time.Patients with liver cancer are prone to negative psychological emotions such as anxiety,depression,and fear.During treatment,patients are known to experience complex and diverse psychological dilemmas[5].Moreover,physical pain,a long treatment process,medical treatment dilemmas,complications,and the threat of death may result in patients already physical and mental stress being unable to cope[6].Furthermore,the cost of treatment is high,repeated hospitalizations are often required,and work and social life are affected.A patient’s financial income is likely to be reduced,resulting in increased financial pressure on a family,and patients often have feelings of guilt.The incidence of liver cancer has been reported to peak between the ages of 40 and 60 years[7] and patients in this age group are frequently providing fundamental financial and emotional support within their families.Following the onset of liver cancer,the resulting stress may trigger psychological issues that are challenging to overcome,especially for male patients in China.Historically,clinical treatment for liver cancer has involved medical staff paying attention more often to surgery or drug treatment for patients with cancer,while overlooking or underestimating changes in the mental status of patients with cancer.It is important to investigate nursing intervention programs that are suitable for improving the mental status of patients with liver cancer.
The whole-process management model is a type of high-quality nursing service that continues throughout the entire diagnosis and treatment process of patients,that is,patients can enjoy continuous professional nursing services from admission to discharge and from discharge to review,as well as receive rehabilitation[8].The United States and other Western countries have taken the lead in proposing whole-process nursing management and applying it to clinical nursing practice.Following promotion and development,whole-process case nursing has been found not to increase patients’ medical costs,but rather to improve nursing efficiency and reduce medical costs[9].In a previous study,the whole-process management model was applied to patients with breast cancer,which effectively reduced their negative emotions and improved treatment adherence and nursing satisfaction[8].However,the application of this model to patients with liver cancer has rarely been reported.Therefore,this study aimed to explore the effects of the application of whole-process case management on the mental state and self-care ability of patients with liver cancer.
MATERlALS AND METHODS
Study patients
In this single-center,randomized controlled study,60 patients with liver cancer who had been admitted to our hospital from January 2021 to January 2022 were randomly selected.The patients were randomly divided into an observation group (n=30) and a control group (n=30).Inclusion criteria comprised patients: Aged ≥ 18 years,who met the clinical diagnostic criteria for liver cancer[10],and who were fully conscious,with good cognitive function,and fully able to communicate.Exclusion criteria comprised patients: With a prior history of mental illness,with other serious systemic diseases,with major negative events having occurred in recent life,who were unable to perform independent self-care,and with other malignant tumors.Included study patients or their family members signed a written informed consent form to participate in the study.All processes and procedures undertaken during this study were in accordance with the Declaration of Helsinki.
Nursing programs
The control group was supported with routine nursing measures,including routine examination during hospitalization,vital signs testing,timely medical intervention,perioperative care,relevant medication information,routine health education,and bi-weekly telephone follow-up post-discharge.
The observation group received whole-process case management interventions in addition to routine nursing measures.Specifically,the interventions included full-time nurses organizing a seminar to broaden discussions concerning liver-cancer related information.The intervention steps were as follows:
A case management file was established for each patient to provide a continuous and dynamic medical record.
Patient-related issues were analyzed through communicating with patients in the observation group to become better informed concerning their physical and psychological issues,doubts,and confusions in relation to their daily care,and their health behaviors were analyzed to identify practical challenges for discussion.
A nursing plan was proposed.A consensus was reached following discussion and a standardized nursing plan was designed,and health education was conducted once a patient had been admitted.The nursing staff listened and replied to each patient’s consultation content in a timely manner and provided evidence-based guidance.Intensive education was delivered concerning the ward environment,physical and psychological nursing was provided to reinforce the information provided by medical staff,and the care of patients with liver cancer was standardized during hospitalization,especially during the perioperative period,with a view to preventing common complications.
During hospitalization,a psychologist regularly evaluated each patient’s mental status and adjusted psychological interventions in real time according to the assessment results.
Medical staff guided and educated patients while implementing nursing to strengthen patient self-management ability.Pathology-related information specific to liver cancer and perioperative self-intervention methods for patients were introduced.Adverse symptoms that a patient might encounter such as pain,hematemesis,and ascites were explained,and patients were informed of the corresponding countermeasures.Nursing staff positively confirmed patient selfmanagement behaviors in relation to pain,discomfort,or complications.
At discharge,in accordance with the needs of each patient,the nursing staff formulated and implemented work plans for discharge preparation,including home self-care,referral to other hospitals,remote health management,and home follow-up.Personalized electronic files were established for patients throughout the course of the disease.A health management manual was issued to patients to facilitate recording their medication and psychological status outside the hospital.This manual also contained relevant patient information concerning liver cancer and frequently asked questions and responses.Patients were required to bring the manual to follow-up consultations to facilitate more accurate understanding of the current status of each patient by the medical team.
Post-discharge: Follow-up visits were conducted through telephone or Internet platforms such as WeChat,and personal nursing education after discharge was continued,as necessary.A specific WeChat forum was set up with a continuous service team and training was provided for team members.Through the establishment of a WeChat forum,timely team communication,discussion,and a timely response to patient-related questions could be realized.Through continuous and regular assessment of a patient’s mental stateviatelephone or online platforms,and according to the assessment results,professional psychologists provided targeted psychological guidance to patients.Patients were regularly informed of new information concerning liver cancerviathe WeChat platform.Each patient’s weekly feedback information was collated and analyzed,and new content was re-introduced.The intervention was provided continuously for three months post-discharge.
Evaluation indicators
Anxiety and depression:Anxiety was measured using the Hamilton anxiety scale (HAMA)[11] and depressive mood was measured using the Hamilton depression scale (HAMD)[12].The HAMA has a total of 14 questions,involving a fivelevel scoring method ranging from 0 to 4 points,with a total score between 0 and 56 points.The higher the score,the more serious the anxiety.The HAHD has a total of 17 questions,involving a five-level scoring method ranging from 0 to 4 points,with a total score between 0 and 68 points.The higher the score,the more serious the depression.
Level of hope:The Herth hope index (HHI)[13] was used to assess a patient’s level of hope.In total,12 items involving three aspects,namely,attitude,action,and social relationships were assessed with each item ranged from 1 to 4 points,with a total possible score of 48 points.The higher the score,the higher the level of hope.
Self-care ability:Self-care ability was assessed using the self-care ability assessment scale-revision in Chinese (ASAS-RC).The self-care ability assessment scale,first designed in 2014,was used to form the ASAS-R-C scale with a stable structure and clear dimensions[14].The ASAS-R-C scale has three dimensions,namely,general self-care ability,developmental self-care ability,and self-care ability when personal health is poor.Using a Likert five-point scale scoring method,it includes 15 items (items 4,11,14,and 15 are reverse scored),with scores ranging from 15 to 75 points.The higher the score,the stronger the self-care ability.
Symptom distress:We used the memory symptom assessment scale (MSAS)[15],developed at the Memorial Sloan-Kettering Cancer Center in the United States,which is a multi-dimensional symptom self-rating scale consisting of three dimensions,namely,physiological symptoms,psychological symptoms and total distress index.It includes 32 items,of which the first 24 symptom-related items evaluate the symptoms experienced by patients with malignant tumors in terms of incidence,frequency,severity,and distress.Eight further symptom items are used to evaluate the frequency and severity of each symptom item,with scores represented in terms of points ranging from 1 to 4 (low to high),and the degree of distress represented in terms of points ranging from 0 to 4 (low to high).Frequency,severity,and lifedistressing scores for each symptom item are added and divided by 3 to calculate the average score of the symptom.This scale had a Cronbach’s α coefficient of 0.79-0.87 and a content validity of 0.94,and the Chinese version of this scale had good reliability and validity.
Sleep quality:Patient sleep quality was scored using the Pittsburgh sleep quality index (PSQI)[16].The scale has 24 questions divided into seven categories.The scores of each category range from 0 to 3 points,with 0 point indicating there are no problems and 3 points indicating major difficulties.The total score is obtained by adding the scores of each category and can range between 0 and 21 points.The higher the score,the poorer the sleep quality.
Quality of life:Quality of life was assessed using the quality of life measurement scale for patients with liver cancer (QLICP-LI)[17].This scale,consisting of a general module (version 2.0) and a liver cancer-specific model,includes 32 items covering four areas,namely,physical function,psychological function,social function,and common symptoms and side-effects.It also includes eight items covering basic physiological function and mobility and activity ability;nine items covering cognition,emotion and will;and eight items covering interpersonal communication,social support and security,and social role.Common symptoms and side-effects are assessed using seven items.The liver cancer-specific module uses 12 items to assess liver-related signs,systemic manifestations,and specific psychological effects.In total,this scale comprises 13 aspects and 44 items across five areas,with each item ranging from 1 to 5 points and the total score ranging from 44 to 220 points.The higher the score,the better the quality of life.
Statistical methods
SPSS22.0 statistical software was used to analyze the data.Following a normality test,the measurement data approximately followed a normal distribution (expressed as mean ± SD).Counting data are represented as percentages.We conducted at-test,a Pearson’s chi-square test,a Fisher’s exact test or a Mann-Whitney test,as required.Pvalues < 0.05 were considered statistically significant.
RESULTS
Patient baseline data
In total,60 patients with liver cancer (average age,50.16 ± 9.37 years;males,66.67%;females,33.33%;Child-Pugh grades: Grade A,65%;grade B,35.00%) were included in our study.In terms of education levels,45% of the patients had at least completed junior high school,36.67% had completed senior high school,and 18.33% had completed university.In terms of tumor-node-metastasis (TNM) stages,8.33% of the patients had stage I liver cancer,70.00% had stage II,and 21.67% had stage III.In addition,15% of the patients had hepatocellular carcinoma,68.33% had adenocarcinoma,11.67% had squamous cell carcinoma,and 5.00% had liver cancer of other pathological types.
Compared with the control group,no statistically significant differences were observed in baseline data concerning age,sex,Child-Pugh grade,education level,pathological type,TNM stage,and other general data in the observation group (P> 0.05;Table 1).
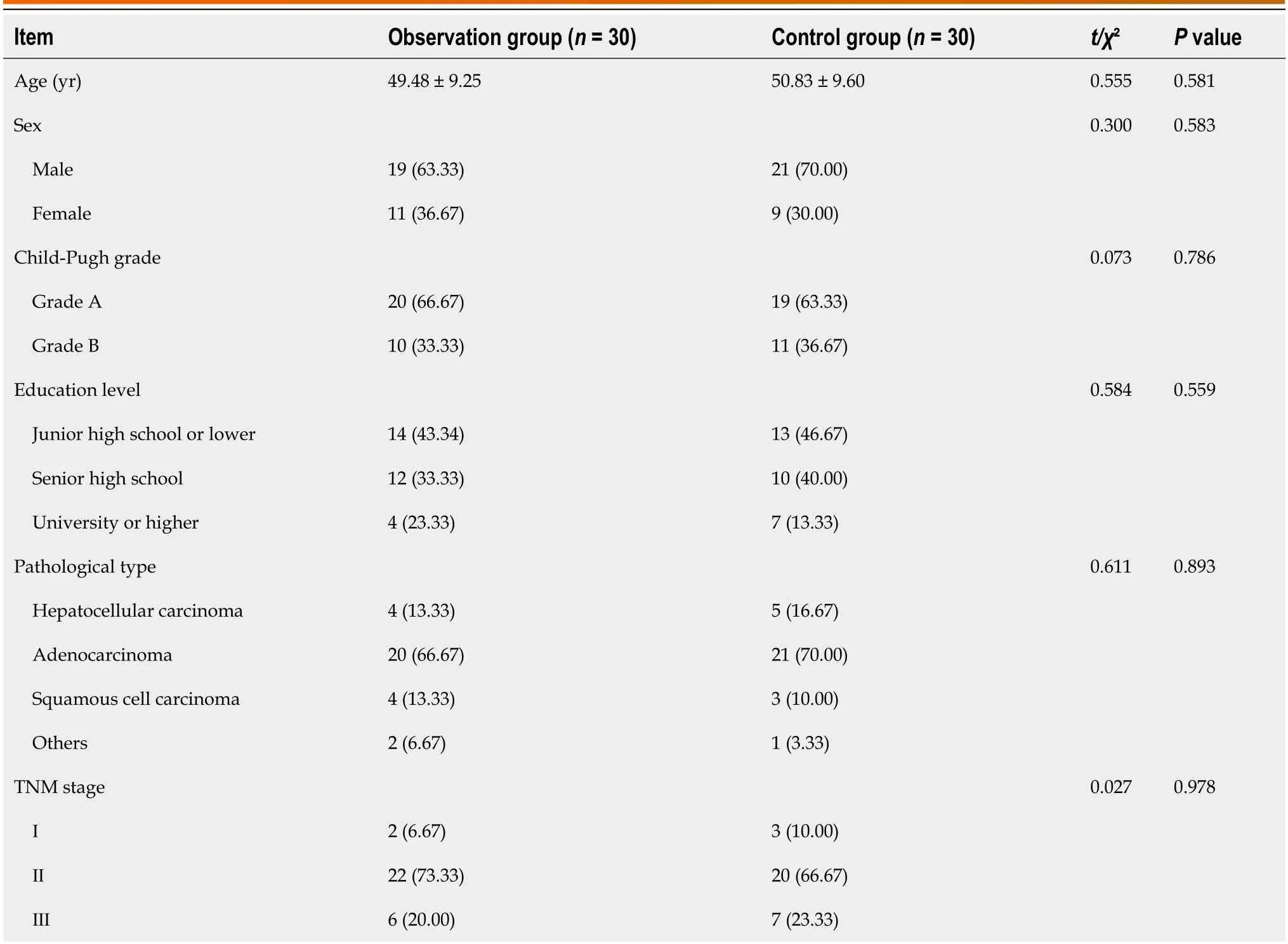
Table 1 Comparison of baseline data between the two groups [n (%),mean ± SD]
Comparisons between anxiety, depression, and level of hope
Pre-intervention,compared with the control group,no statistically significant differences were observed in the observation group concerning the HAMA,HAMD,and HHI scores (P> 0.05).Post-intervention,the HAMA and HAHD scores in both groups were significantly lower than those pre-intervention,and observation group scores were significantly lower than those in the control group (P< 0.05).Compared with pre-intervention scores,the HHI score in both groups was significantly higher,and observation group scores were significantly higher than those in the control group (P< 0.05;Table 2).
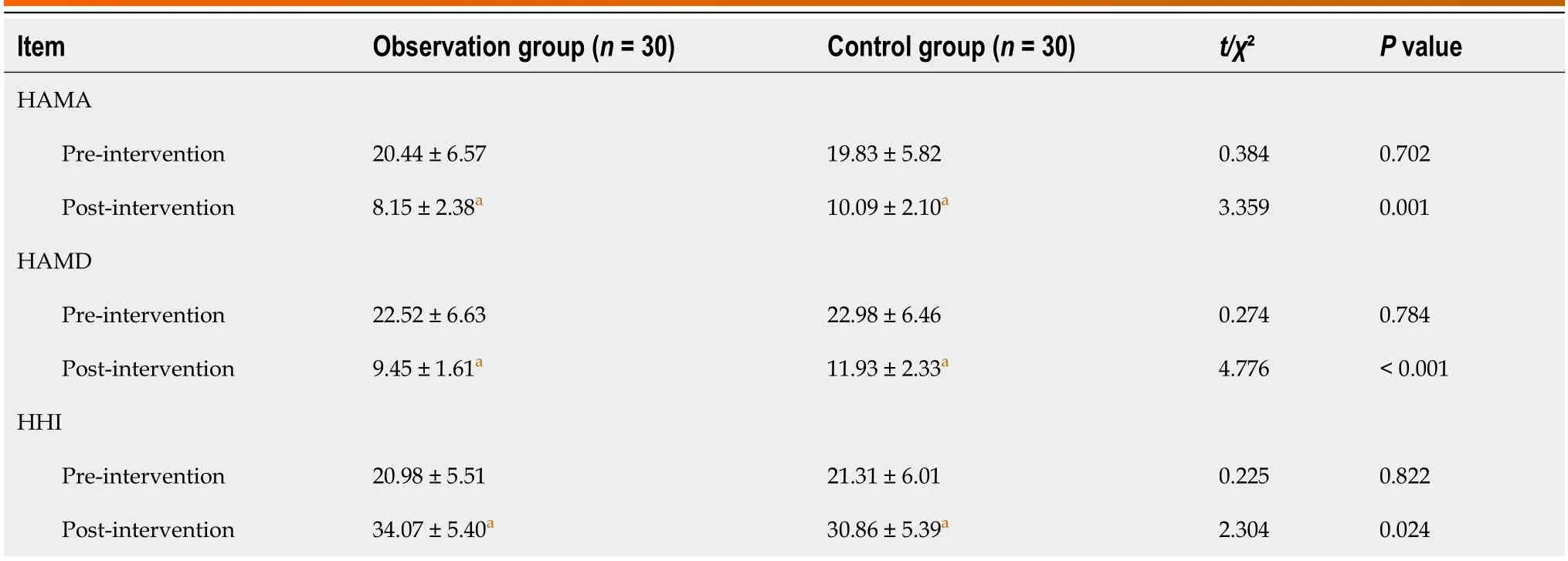
Table 2 Comparison of anxiety and depression plus hope level between two groups (mean ± SD)
Comparison of self-care ability
Pre-intervention,compared with the control group,no statistically significant difference was observed in the ASAS-R-C scores in the observation group (P> 0.05).Post-intervention,the ASAS-R-C score was significantly higher in both groups compared with pre-intervention scores,and observation group scores were significantly higher than those in the control group (P< 0.05;Table 3).

Table 3 Comparison of self-care abilities assessment scale-revision in Chinese between two groups (mean ± SD)
Comparison of symptom distress
Pre-intervention,compared with the control group,no statistically significant difference was observed in each dimension of the MSAS scores in the observation group (P> 0.05).Post-intervention,the MSAS scores in each dimension in the two groups were significantly lower than those in each group pre-intervention,and observation group scores were significantly lower than those in the control group (P< 0.05;Table 4).
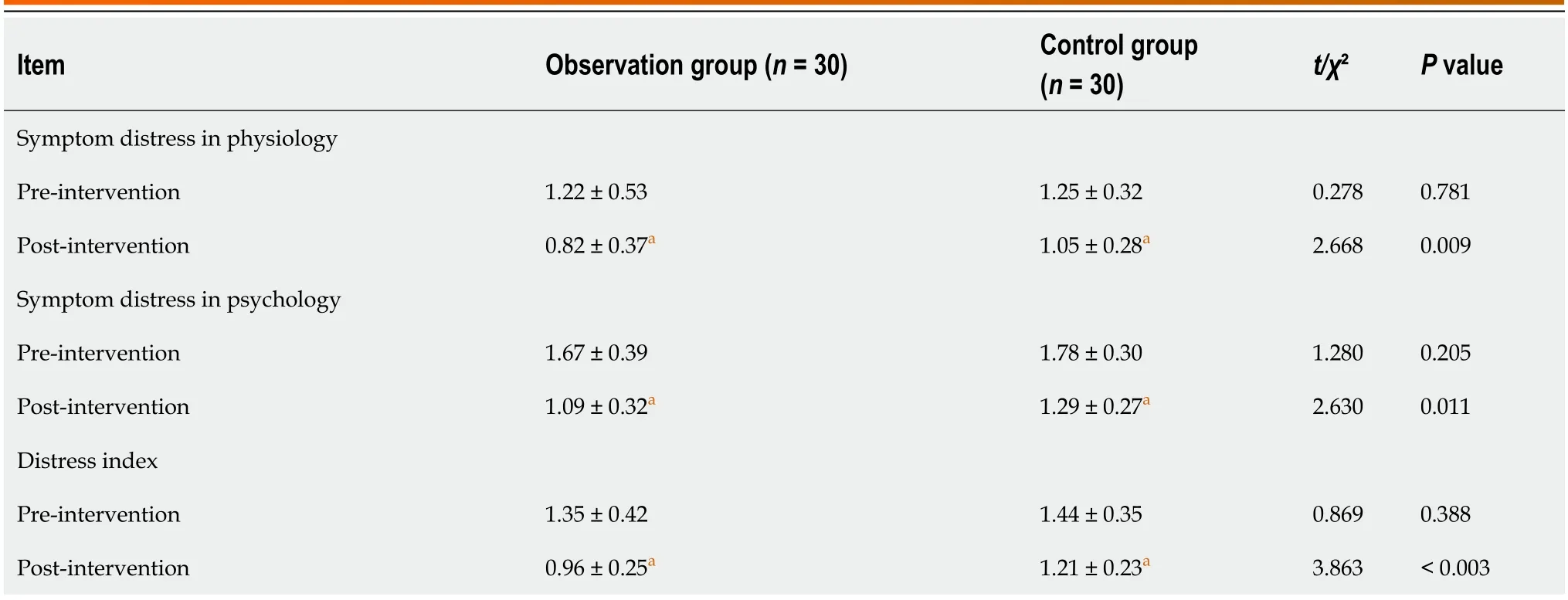
Table 4 Comparison of symptom distress between the two groups (mean ± SD)
Comparison of sleep quality and quality of life
Pre-intervention,no statistically significant difference in PSQI scores was observed in the observation group compared with the control group (P> 0.05).Post-intervention,the PSQI scores of both groups were significantly lower than those in each group pre-intervention,and observation group scores were significantly lower than those in the control group (P< 0.05).Compared with each group pre-intervention,the QLICP-LI scores in both groups were significantly higher postintervention,with observation group scores significantly higher post-intervention than those in the control group (P< 0.05;Table 5).
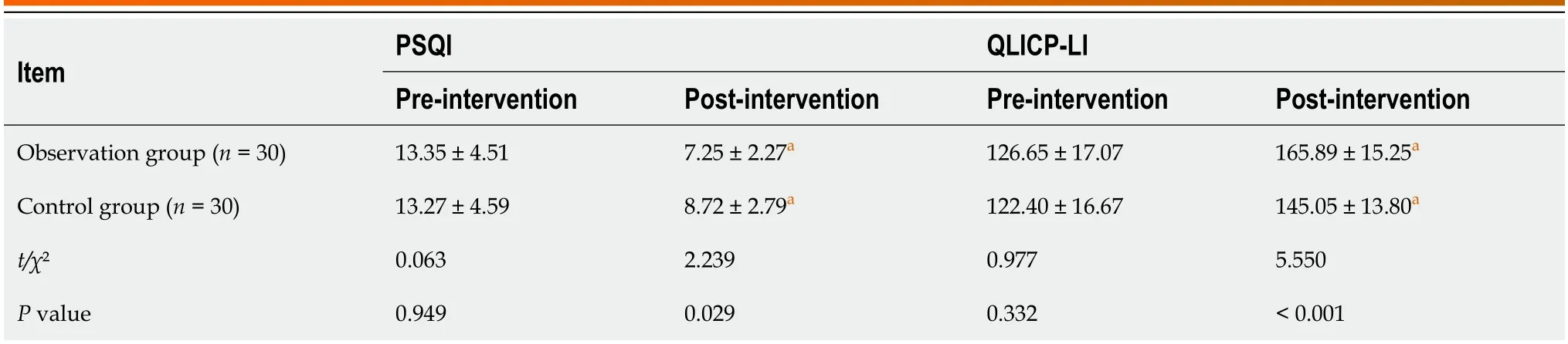
Table 5 Comparison of sleep quality and life quality (mean ± SD)
DlSCUSSlON
The onset age of liver cancer reaches a peak at 45 years,with males having a higher risk of developing liver cancer than females[18,19].The clinical treatment for liver cancer currently mainly involves interventional treatment such as radiotherapy,chemotherapy,surgical resection,or Transcatheter arterial chemoembolization.While the above treatment methods have shown good efficacy,patients with liver cancer are under considerable physical and mental pressure during the treatment process.Some patients have severe depression,anxiety,and other negative emotions,and a poor mental state.Furthermore,the self-management ability of patients with cancer in China is of a medium level,and issues such as insufficient self-management awareness,lack of knowledge and information,and poor disease management ability have been reported[20-22].These issues have an important effect on quality of life,treatment decisions,and a desire to survive.
The whole-process case management model provides a more comprehensive medical service compared with the general hospitalization mode.The main highlight of the whole-process case management model is managed participation in the entire treatment course,which can also be regarded as an extension of the hospitalization routine treatment outside the hospital[23,24].
In this study,the HAMA,HAMD,MSAS,and PSQI scores of both groups post-intervention were lower than preintervention scores,with the observation group having lower scores than the control group (P< 0.05).The HHI,ASAS-RC,and QLICP-LI scores were higher in both groups compared to their respective baseline values.However,the observation group had significantly higher scores than the control group (P< 0.05).Our findings indicate that the wholeprocess case management model could effectively reduce the anxiety and depression in patients with liver cancer,reduce symptom distress,and improve the level of hope,self-care ability,sleep quality and life quality.
The whole-process case management model established a relationship of mutual trust with patients in the early stage of treatment,with regular communication undertaken through various channels such as telephone and the WeChat platform,which provided patients with continuous confidence in treatment,encouragement when encountering difficulties,and facilitated responses to their questions.Patients could receive advice when they were facing life pressures,which helped them to overcome negative thoughts.The patients were asked to regularly record their information concerning their physical and psychological status,identify issues that were mostly causing them anxiety,and to set out recently completed treatment goals.These recordings allowed them to gain confidence in the treatment process and to improve their level of hope[25].
In addition,in the observation group,the whole-process case management service was implementedviathe WeChat platform,which was convenient for medical staff to fully and dynamically learn about the self-care situation of patients outside of the hospital,and to provide timely adjustments to strengthen the content and direction of continuous care.For patients who could not use WeChat,nurses could guide family members to enter the WeChat platform and join the whole-process case management.In the process of home treatment,patients could complete remote health consultationsviathe network,doctors and nursing staff could communicate with patients in real time,and nursing staff could provide relevant knowledge in relation to liver cancer,precautions when taking medication,and preliminary treatment when discomfort or complications occurred to patientsviathe network platform.Patients carried out self-health management under professional supervision and guidance.This method has been shown to effectively reduce the effect of varioussymptoms during hospitalization and following discharge in relation to the physical and mental health of patients,ensuring patient safety post-discharge[26].
This study had some limitations.First,this single-center clinical study involved only a small number of patients from the same hospital and within the same region,which may have led to selection bias.Second,this study only followed the patients for three months and long-term effects of the intervention were not observed.Third,nurses collaborate,coordinate,and execute whole nursing,which is key to ensuring the safety of nursing and improving the quality of nursing.While the nurses involved in the whole-process case management in this study were specialist nurses,there can be deficiencies in managing all aspects of the nursing process and implementing nursing intervention strategies,and the theoretical knowledge and operation technology may not be able to quickly meet the requirements of the whole-process case management model.The next step is to continue to expand the sample size,improve the study design,and encourage nursing staff to continuously improve their nursing skills to ensure effective implementation of the wholeprocess case management model in future studies.
CONCLUSlON
In summary,the whole-process case management was shown to effectively reduce the anxiety and depression in patients with liver cancer,reduce symptom distress and improve the level of hope,self-care ability,sleep quality and life quality,as well as provide feasible nursing alternatives for patients with liver cancer.
ARTlCLE HlGHLlGHTS
Research background
In China,liver cancer incidence is fourth,following lung,gastric,and esophageal cancers.Case fatality rate is third after lung and cervical cancer.A previous study applied whole-process management model to breast cancer patients,effectively reducing negative emotions,improving treatment adherence,and nursing satisfaction.
Research motivation
Improve the hope level,self-care ability,sleep quality and quality of life,and provide feasible care plan for liver cancer patients.
Research objectives
To study the psychological state and self-care ability of liver cancer patients: the effect of the whole process of case management
Research methods
We compared anxiety,depression,hope level,self-care ability,symptom distress,sleep quality,and quality of life between the two groups.
Research results
Whole-course case management can effectively reduce anxiety and depression,relieve symptoms and problems.
Research conclusions
Improve patient self-care ability and provide feasible nursing plan for liver cancer patients.
Research perspectives
This is a research perspective of the whole-process case management.
FOOTNOTES
Co-first authors:Man-Di Ju and Qin Qin.
Author contributions:Ju MD and Qin Q designed the research;Li M,Ju MD and Qin Q performed the research;Li M,Ju MD and Qin Q contributed new reagents/analytic tools;Li M,Ju MD and Qin Q analyzed the data;Ju MD and Qin Q wrote the paper;All authors were involved in the critical review of the results and have contributed to,read,and approved the final manuscript.Ju MD and Qin Q contributed equally to this work as co-first authors equally to this work.Ju MD and Qin Q contributed efforts of equal substance throughout the research process.The choice of these researchers as co-first authors acknowledges and respects this equal contribution,while recognizing the spirit of teamwork and collaboration of this study.In summary,we believe that designating Ju MD and Qin Q as co-first authors of are fitting for our manuscript as it accurately reflects our team’s collaborative spirit,equal contributions,and diversity.
lnstitutional review board statement:This study protocol was approved by the General Hospital of the Yangtze River Shipping,and all the families have voluntarily participated in the study and have signed informed consent forms.
Clinical trial registration statement:We have not registered URL number.We have the ethical certificate approved by the unit.
lnformed consent statement:All the families have voluntarily participated in the study and have signed informed consent forms.
Conflict-of-interest statement:All the authors report no relevant conflicts of interest for this article.
Data sharing statement:Data generated from this investigation are available upon reasonable request from the corresponding author at limeng333321@163.com.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BY-NC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is non-commercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORClD number:Meng Li 0009-0005-1170-6134.
S-Editor:Li L
L-Editor:A
P-Editor:Yuan YY
杂志排行

World Journal of Gastrointestinal Surgery的其它文章
- Alcohol associated liver disease and bariatric surgery: Current perspectives and future directions
- Applications of gastric peroral endoscopic myotomy in the treatment of upper gastrointestinal tract disease
- Ex vivo liver resection and auto-transplantation and special systemic therapy in perihilar cholangiocarcinoma treatment
- Evaluation of bacterial contamination and medium-term oncological outcomes of intracorporeal anastomosis for colon cancer: A propensity score matching analysis
- Rescue from complications after pancreaticoduodenectomies at a low-volume Caribbean center: Value of tailored peri-pancreatectomy protocols
- Comparison of prognosis and postoperative morbidities between standard pancreaticoduodenectomy and the TRlANGLE technique for resectable pancreatic ductal adenocarcinoma