Clinical study of enhanced recovery after surgery in laparoscopic appendectomy for acute appendicitis
2024-05-07ZhuLinLiHuaChongMaYongYangJianJunChenZhenJunWang
Zhu-Lin Li,Hua-Chong Ma,Yong Yang,Jian-Jun Chen,Zhen-Jun Wang
Abstract BACKGROUND Enhanced recovery after surgery (ERAS) protocol is a comprehensive management modality that promotes patient recovery,especially in the patients undergoing digestive tumor surgeries.However,it is less commonly used in the appendectomy.AIM To study the application value of ERAS in laparoscopic surgery for acute appendicitis.METHODS A total of 120 patients who underwent laparoscopic appendectomy due to acute appendicitis were divided into experimental group and control group by random number table method,including 63 patients in the experimental group and 57 patients in the control group.Patients in the experimental group were managed with the ERAS protocol,and those in the control group were received the traditional treatment.The exhaust time,the hospitalization duration,the hospitalization expense and the pain score between the two groups were compared.RESULTS There was no significant difference in age,gender,body mass index and Sunshine Appendicitis Grading System score between the experimental group and the control group (P > 0.05).Compared to the control group,the patients in the experimental group had earlier exhaust time,shorter hospitalization time,less hospitalization cost and lower degree of pain sensation.The differences were statistically significant (P < 0.01).CONCLUSION ERAS could significantly accelerate the recovery of patients who underwent laparoscopic appendectomy for acute appendicitis,shorten the hospitalization time and reduce hospitalization costs.It is a safe and effective approach.
Key Words: Enhanced recovery after surgery;Appendicectomy;Laparoscopy;Acute appendicitis;Treatment
lNTRODUCTlON
Enhanced recovery after surgery (ERAS) was a therapeutic concept.It optimizes clinical pathways through multidisciplinary collaboration such as surgery,anesthesia,and nursing,reducing the physiological and psychological stress reactions of surgical patients,and ultimately promoting patient recovery[1,2].This concept was first proposed by a Danish doctor Kehlet in 2001,and was introduced to China by Academician Li Jie-Shou in 2006.ERAS protocols were initially developed for colorectal surgery and was widely applied in various fields of the medical process at present but with few applications and reports in appendix surgery[3,4].
Appendicitis was the most common acute abdomen in the world,with an incidence rate of approximately one in a thousand in adults[5].Surgery remained the main treatment for acute appendicitis.Patients often experienced varying degrees of pain and indigestion after surgery,which could prolong hospital stay and increase the risk of postoperative complications.The role of ERAS in the field of elective surgery is evident,but there is currently limited research on its role in emergency surgery.This study aims to explore the feasibility and clinical effects of ERAS in laparoscopic appendectomy.
MATERlALS AND METHODS
Patient data
Inclusion criteria were as follows: (1) Aged 18-70 years;(2) American society of Anesthesiologists score I-II;(3) Nongestational appendicitis;and (4) No history of abdominal surgery.
This study is a prospective randomized controlled study.A total of 120 patients who met the inclusion criteria and were diagnosed with acute appendicitis before surgery between March 2018 and March 2020 were randomly divided into an experimental group and a control group using a random number table method.The experimental group consisted of 63 patients (34 males and 29 females) and the control group consisted of 57 patients (26 males and 31 females).The severity of acute appendicitis was evaluated on the Sunshine Appendicitis Grading System (SAGS) score published in 2017[6].SAGS 1-SAGS 4 represented simple appendicitis,purulent appendicitis,purulent appendicitis with four quadrant contamination and perforated appendix respectively.Informed consent was obtained from all patients and their families,and the study was approved by the hospital's Ethics and Medical Committee.
Treatment methods
The experimental group adopted the ERAS protocol for perioperative management,while the control group adopted traditional methods for perioperative management.The specific methods used were shown in Table 1.All patients underwent laparoscopic appendectomy,with detailed postoperative records of patient exhaust time,pain scores,and other indicators.The differences in gastrointestinal function recovery time,hospitalization time,hospitalization costs,and pain scores between the two groups were compared and analyzed.
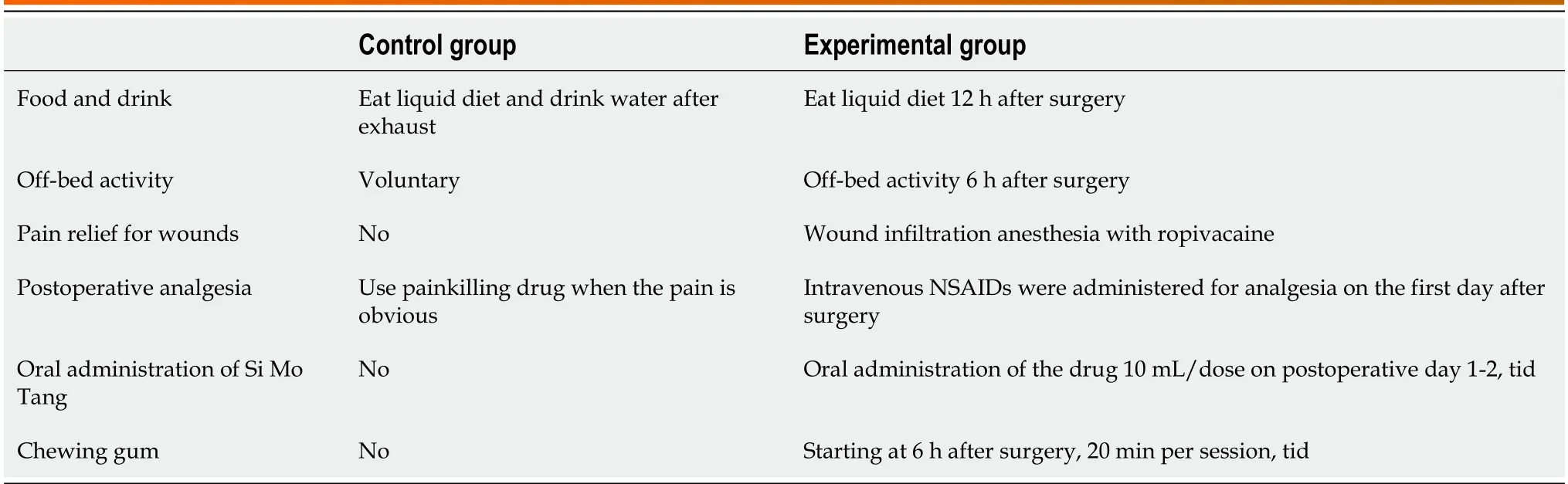
Table 1 Two sets of perioperative management protocols
Observation indicators
Observation indicators included postoperative recovery time of gastrointestinal function,hospitalization stay,hospitalization expenses,and pain score (Table 2).The pain score was evaluated using the numerical rating scale,which was evaluated six hours after surgery by chief surgeon.

Table 2 Comparison of observed indexes between two groups of patients (mean ± SD)
Statistical analysis
SPSS22.0 statistical software was used to analyze the data.Quantitative data of normal distribution were expressed as mean ± SD.Thet-test of two independent samples was used for inter-group comparison,and the Chi-square test was used to analyze the differences in the clinicopathological features between the experimental and control groups.The difference was statistically significant withP< 0.05.
RESULTS
Comparison of clinicopathological features between the two groups
In the experimental group,the patients included 34 males and 29 females and ranged from 16-years-old to 69-years-old (38.5 ± 13.7 years).There were 11 patients whose body mass index (BMI) exceed 25 kg/m2and 52 patients whose BMI did not exceed 25 kg/m2.There were 30 cases in SAGS score 2 group and 15 cases in SAGS score 3 group.In the control group,the patients included 26 males and 31 females and ranged from 15-years-old to 70-years-old (39.7 ± 14.6 years).There were 14 patients whose BMI exceed 25 kg/m2and 43 patients whose BMI did not exceed 25 kg/m2.There were no statistically significant differences in age,gender,BMI and SAGS score between the experimental group and the control group (P> 0.05;Table 3).
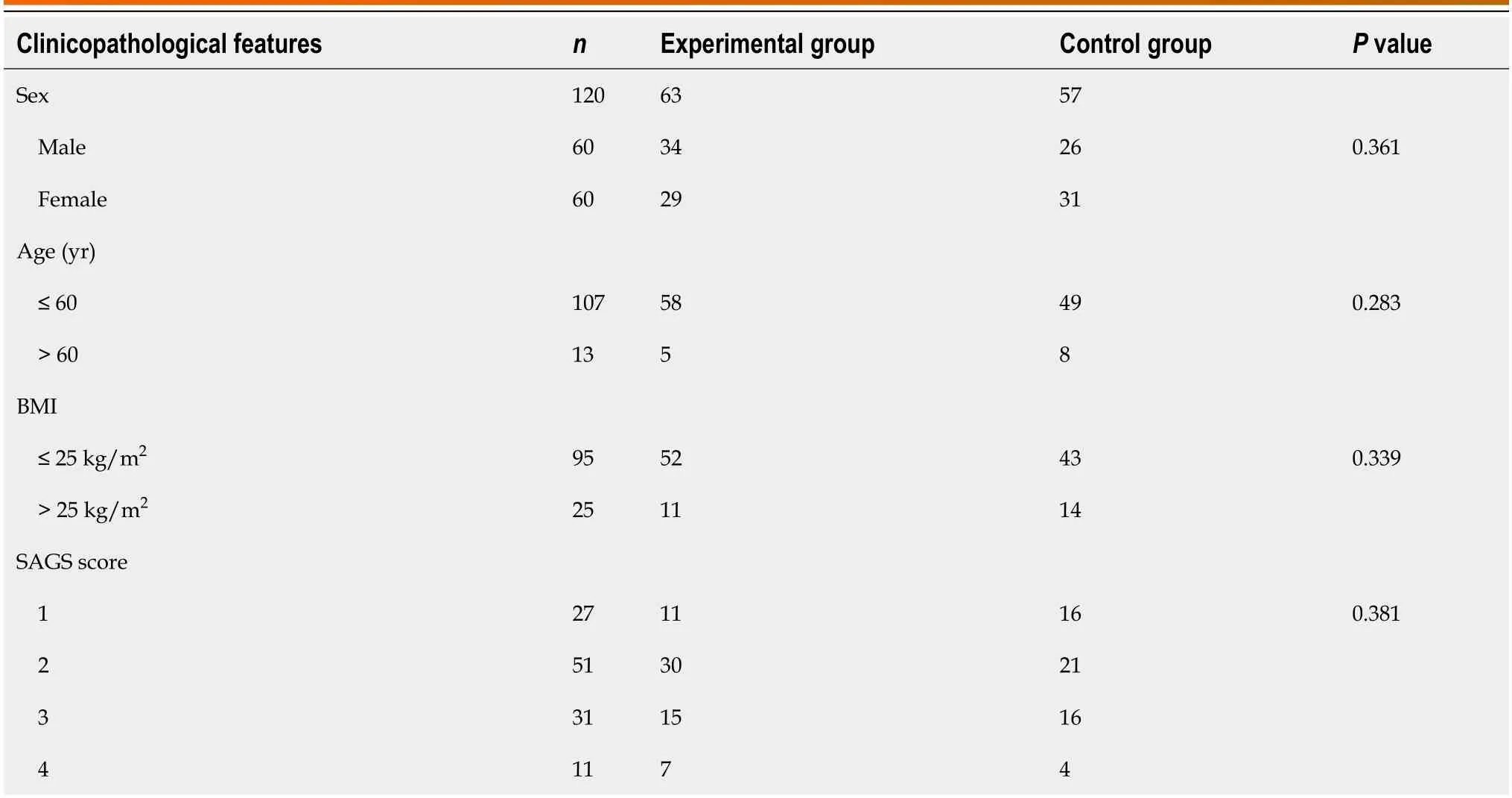
Table 3 Analysis of clinicopathological features of 120 patients
Comparison of observed indexes between the two groups
Both groups of surgeries were successful and there was no conversion to open surgery.Compared with the control group,patients in experimental group had earlier postoperative exhaust time,shorter hospital stay,lower hospitalization costs,and lower pain scores.The differences between the two groups were statistically significant (P< 0.05;Table 2).
Complications and patient outcomes
One patient in the control group had wound infection and one patient in the experimental group had urinary retention.The other patients did not have complications such as lung infection,abdominal abscess,urinary tract infection,etc.All patients recovered well and were discharged.
DlSCUSSlON
With the transformation of medical models,solving psychological and social factors reflected a comprehensive care for improvement of health at a higher level.Therefore,reducing patients' pain and accelerating their recovery had become practical and urgent.The concept of ERAS was proposed by optimizing the perioperative management process,reducing stress reactions and postoperative complications,thereby shortening hospitalization duration and accelerating patient recovery.This concept was introduced into China in 2006 and gradually applied in surgical treatment in multiple disciplines such as gastrointestinal surgery,thoracic surgery,and urology,achieving positive clinical outcome[7-9].
In this study,administration of sufficient postoperative analgesia and the promotion of gastrointestinal function recovery were the focus of our attention.Research had shown that active and effective pain relief could alleviate patients' fear of pain,facilitate early off-bed activity,and accelerate the recovery of patient organ function[10].The current mode of postoperative analgesia had shifted from single mode analgesia to multi-mode analgesia[11].Compared to single mode analgesia dominated by opioids,multimodal analgesia was a type of analgesic mode that combined analgesic drugs or methods with different mechanisms of action.The aim of this model was to increase the analgesic effect and reduce adverse reactions through the complementarity of different drug mechanisms[12].Regarding the pain after abdominal surgery,which mainly includes visceral pain,incision pain,and inflammatory pain,we used ropivacaine to locally infil-trate and anesthetize the incision at the end of the surgery to reduce the incision pain.At the same time,we administered non-steroidal anti-inflammatory drugs on the first day after surgery to alleviate the patient's postoperative inflammatory pain.Compared with the control group,patients in the experimental group had lower pain scores,and the difference was statistically significant.Ropivacaine was an amide-based local anesthetic agent with advantages such as good anesthetic effect and minimal toxic side effects,and was commonly used for wound infiltration anesthesia[13].Non-steroidal antiinflammatory drugs could selectively inhibit cyclooxygenase-2,reduce prostaglandin synthesis,and achieve the effect of inhibiting postoperative inflammatory pain.Currently,they had become the basic medication for multimodal analgesia.
Postoperative gastrointestinal dysfunction may occur to varying degrees,with clinical manifestations including postoperative nausea,vomiting,abdominal pain,and cessation of exhaust and bowel movements.The mechanism of its occurrence was still not fully understood.Current research suggested that it was caused by multiple factors,including surgical trauma stress,inflammatory factors,anesthetic drugs,and BMI[14,15].Therefore,restoring gastrointestinal function required a multi-pronged approach.In the experimental group in our study,patients were fed liquid food 12 h after surgery,while taking oral Si Mo Tang (a traditional Chinese medicine,TCM),chewing gum to accelerate the recovery of gastrointestinal function.The results showed that the first exhaust time of this group of patients was 5.9 h earlier than that of the control group.Early postoperative eating was not only to provide energy and supplement nutrition,but more importantly,it could stimulate nerve reflexes and the release of neurotransmitters,increase intestinal peristalsis,and facilitate the recovery of gastrointestinal motility.Si Mo Tang was a Qi regulating agent in TCM,which had the effects of regulating Qi,reducing adverse reactions,reducing accumulation and relieving pain,and could promote the recovery of gastrointestinal function after abdominal surgery[16].Chewing gum had the same effect as sham feeding,which could stimulate the vagus nerve and activate the cholinergic anti-inflammatory pathway,thereby facilitating the recovery of gastrointestinal function[17,18].In summary,the combination of multiple treatment methods could accelerate the recovery of gastrointestinal function.
A limitation of this study was the use of a small number of patients in a single center,in the future,a multicenter study with a larger sample size is needed to further confirm our findings.
CONCLUSlON
In summary,this study applied the concept of ERAS during the perioperative period of laparoscopic surgery for acute appendicitis.Compared with the control group,the experimental group showed a significant improvement in recovery,characterized by earlier exhaust time,shorter hospitalization time,lower hospitalization costs,and lower patient pain scores.Therefore,applying the concept of ERAS to laparoscopic appendectomy was safe,economical and effective,and was worth further promotion and implementation.
ARTlCLE HlGHLlGHTS
Research background
Enhanced recovery after surgery (ERAS) protocol has shown to be beneficial to patients undergoing various abdominal surgeries,especially in the digestive tumor surgery.However,few studies have explored the application of ERAS in laparoscopic surgery for acute appendicitis.
Research motivation
To determine if ERAS is beneficial to patients undergoing laparoscopic surgery for acute appendicitis.
Research objectives
This study aimed to evaluate the value of ERAS in laparoscopic surgery for acute appendicitis.
Research methods
A prospective randomized controlled study was performed in Beijing Chao-Yang Hospital.A total of 120 patients who met the inclusion criteria and were diagnosed with acute appendicitis before surgery between March 2018 and March 2020 were randomly divided into an experimental group and a control group using a random number table method.The clinicopathological features of the two groups were analyzed.In addition,variables including gastrointestinal function recovery time,hospitalization duration,hospitalization costs,and pain scores were also analyzed.
Research results
One hundred and twenty patients were included.There were 63 patients in the experimental group and 57 patients in the control group.There was no significant difference in age,gender,body mass index and Sunshine Appendicitis Grading System score between the two groups (P> 0.05).The application of ERAS resulted in accelerated recovery of acute appendicitis patients,shorter hospitalization stay,less hospitalization costs,earlier postoperative exhaust time,and milder pain.
Research conclusions
The application of ERAS is associated with shorter hospitalization stay,less hospitalization costs,earlier postoperative exhaust time,and milder pain in the patients who underwent laparoscopic appendectomy due to acute appendicitis.It is safe,economical and effective.
Research perspectives
The findings in this study can encourage surgeons to pay more attention to postoperative management measures for patients with acute appendicitis,and to apply the concept of ERAS to their postoperative recovery,thereby reducing the burden on patients and saving medical resources.
FOOTNOTES
Author contributions:Li ZL,Wang ZJ and Ma HC designed the study;Li ZL and Chen JJ collected and analyzed the data;Li ZL wrote the manuscript;Yang Y and Ma HC revised the manuscript;Yang Y participated in collection of the data;All authors approved the final version of the manuscript.
lnstitutional review board statement:The study was reviewed and approved by the Beijing Chao-Yang Hospital’s Ethics and Medical Committee (approval No.2018-Ke-340).
Clinical trial registration statement:This study is registered at https://www.chictr.org.cn/searchproj.html;The registration identification number is ChiCTR2400081069.
lnformed consent statement:Informed consent was obtained from all patients and their families.
Conflict-of-interest statement:All the authors report no relevant conflicts of interest for this article.
Data sharing statement:No additional data are available.
CONSORT 2010 statement:The authors have read the CONSORT 2010 statement,and the manuscript was prepared and revised according to the CONSORT 2010 statement.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BY-NC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is non-commercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORClD number:Zhu-Lin Li 0000-0001-7935-3981;Yong Yang 0000-0001-8824-156X;Zhen-Jun Wang 0000-0003-0176-6588.
S-Editor:Li L
L-Editor:A
P-Editor:Xu ZH
杂志排行

World Journal of Gastrointestinal Surgery的其它文章
- Alcohol associated liver disease and bariatric surgery: Current perspectives and future directions
- Applications of gastric peroral endoscopic myotomy in the treatment of upper gastrointestinal tract disease
- Ex vivo liver resection and auto-transplantation and special systemic therapy in perihilar cholangiocarcinoma treatment
- Evaluation of bacterial contamination and medium-term oncological outcomes of intracorporeal anastomosis for colon cancer: A propensity score matching analysis
- Rescue from complications after pancreaticoduodenectomies at a low-volume Caribbean center: Value of tailored peri-pancreatectomy protocols
- Comparison of prognosis and postoperative morbidities between standard pancreaticoduodenectomy and the TRlANGLE technique for resectable pancreatic ductal adenocarcinoma