Prevalence and risk factors associated with long COVID symptoms in children and adolescents in a southern province of Vietnam
2024-04-07HuynhNgocLinhNguyenTheTanLeThiMinhThuNguyenTuLoanNguyenThiToUyenLeThanhThaoTrangTruongThanhNamDoanHoangPhu
Huynh Ngoc Linh ,Nguyen The Tan ,Le Thi Minh Thu ,Nguyen Tu Loan ,Nguyen Thi To Uyen ,Le Thanh Thao Trang ,Truong Thanh Nam,Doan Hoang Phu
1Faculty of Medicine,Ca Mau Medical College,Ca Mau 98000,Vietnam
2Ca Mau Obstetrics and Pediatrics Hospital,Ca Mau 98000,Vietnam
3Faculty of Basic Science and Public Health,Dong Thap Medical College,Dong Thap 81000,Vietnam
4Graduate University of Sciences and Technology,Vietnam Academy of Science and Technology,Ha Noi 10000,Vietnam
5Community Public Health Research Program,School of Public Health,Walailak University,Nakhon Si Thammarat 80160,Thailand
6Faculty Public Health,Can Tho University of Medicine and Pharmacy,Can Tho City 94000,Vietnam
7Doctoral Program in Health Sciences,College of Graduate Studies,Walailak University,Nakhon Si Thammarat 80160,Thailand
ABSTRACT Objective: To investigate the prevalence and risk factors associated with long COVID symptoms among children and adolescents who have recovered from COVID-19.Methods: This study applied a cross-sectional approach within community settings in a southern province of Vietnam.A structured questionnaire featuring socio-demographic information and common long COVID symptoms was employed.Phi correlation coefficients assessed associations among pairs of long COVID symptoms.Additionally,multivariable logistic regression models were performed to investigate the risk factors of long COVID in recovered COVID-19 children and adolescents.Results: Among 422 participants,39.3% reported long COVID symptoms,with a prevalence of 45.2% (SD=0.5) in children and 22.2% (SD=0.4) in adolescents.Common symptoms reported were cough 34.6% (SD=0.5),fatigue 20.6% (SD=0.4),shortness of breath 10.9% (SD=0.3),and lack of appetite 6.6% (SD=0.3).Concerning risk factors of long COVID,a higher risk was observed among demographic groups,including girls (OR 1.25,95% CI 1.15-1.37;P<0.001,reference: boys),children compared to adolescents (OR 1.24,95% CI 1.12-1.37;P<0.001),overweight individuals (OR 1.14,95% CI 1.02-1.27;P=0.018,reference: healthy weight),and participants without any COVID-19 vaccination (OR 1.36,95% CI 1.20-1.54;P<0.001),or have received only one single dose (OR 1.35,95% CI 1.10-1.64;P=0.004) compared to those who have received two doses.Besides,patients with a COVID-19 treatment duration exceeding two weeks also had a higher risk of long COVID (OR 1.32,95% CI 1.09-1.60;P=0.003) than those who recovered less than seven days.Conclusions: The insights from this study provide crucial guidance for predicting the factors associated with the occurrence of long COVID in pediatric patients,contributing to strategic interventions aimed at mitigating the long COVID risks among children and adolescents in Vietnam.
KEYWORDS: Long COVID;Prevalence;Risk factors;Children;Adolescent;Vietnam
Significance
A high prevalence of long COVID was observed in Vietnam’s community settings.Common symptoms included cough,fatigue,shortness of breath,and loss of appetite.Risk factors associated with long COVID included children (ref:adolescents),girls (ref: boys),overweight status (ref: healthy weight),lack of vaccination or receipt of a single dose (ref: two doses of COVID-19 vaccine),and recovery duration over two weeks (ref: less than seven days).
1.Introduction
The World Health Organization (WHO) announced the end of the COVID-19 pandemic as a global health emergency in May 2023[1].However,the post-outbreak focus has shifted to the prolonged symptoms experienced by individuals after recovering from COVID-19 infection,known as long COVID[2].The WHO officially defined long COVID in October 2021,indicating that these conditions typically arise approximately three months after the onset of COVID-19 symptoms,with the associated symptoms persisting for a minimum duration of two months without being explained by any other alternative diagnoses[3].Around 10% to 20% of COVID-19 patients are estimated to experience long COVID conditions[4].
Although children have lower rates of COVID-19 infection than adults[5,6],emerging evidence has revealed the existence of a long COVID syndrome in pediatric patients[7,8].Especially,multisystem inflammatory syndrome in children (MIS-C) is a severe delayed complication of SARS-CoV-2 infection,particularly affecting children aged 5 to 11 years[9].It causes inflammation in various body parts,increasing the risk of long COVID in affected children and adolescents[10].A previous study revealed a wide variety of prevalence of long COVID symptoms,ranging from 1.6% to 70%,in children and adolescents.The most commonly reported symptoms were fatigue,headache,chest tightness or pain[8].Notably,the persistence of fatigue could be intense and lasted for 6 to 8 months,making children unable to fully resume their regular school activities,eventually leading to prolonged school absences[11].Furthermore,mood symptoms,sleep disorders,cough,loss of taste/smell,and shortness of breath were also reported as common symptoms of long COVID[8,12,13].These symptoms significantly encumber children's daily lives,substantially limiting their daily functioning[14].According to a recent study,43.9% of children exhibiting these persistent symptoms faced adverse effects on their routine activities[15].
Numerous studies have identified specific demographic characteristics,such as older age and sex,as well as medical histories,as potential risk factors for developing long COVID conditions among children and young adults.In a prospective cohort study involving 518 children,those over six faced a higher risk of long COVID than children under six years old[16].Concerning sex,female patients exhibited a higher prevalence of long COVID symptoms[2].Additionally,medical histories,such as allergies or long-term medical conditions,were significantly associated with an increased risk of persistent symptoms of long COVID[17,18].Besides,various clinical factors have been identified as being linked to long COVID.These factors include muscle pain upon admission,admission to the intensive care unit,a higher body mass index,and a longer duration of infection[14,19].
There remains a significant gap in our understanding of long COVID in children and adolescents.This stems from the prevailing belief that children and young adults experience milder COVID-19 than adults,thereby underestimating the potential long COVID conditions in this demographic group[20,21].In Vietnam,previous long COVID studies primarily focused on adults,emphasizing typical symptoms such as insomnia[20],and the correlation between long COVID and mental health status[21].Although a recent study explored long COVID in children,its limited sample size due to relying on hospitalized individuals posed limitations[22].Therefore,our study aimed to investigate the prevalence of long COVID and identify the associated risk factors associated with long COVID conditions among children and adolescents who have recovered from COVID-19 in a southern province of Vietnam.The insights derived from our study offer valuable guidance for crafting targeted interventions to address the needs and mitigate the risks of long COVID among children and adolescents in Vietnam.
2.Subjects and methods
2.1.Ethics statement
The study was reviewed and approved by Human Research Ethics Committee of Ca Mau Medical College (No.6/150522-75/YD-CDTYCM).Data on children and adolescents infected with COVID-19 was provided by Ca Mau Obstetrics and Pediatrics Hospital and Center for Disease Control of Ca Mau province.All participants,including children or adolescents and their legal representatives (parents or guardians) were provided with a clear explanation of the study's objectives.The participants provided their written informed consent with the signature of their legal representative to participate in this study.
2.2.Study design and participants
The cross-sectional investigation was conducted in May 2023 in Ca Mau city and five districts of Dam Doi,Cai Nuoc,Tran Van Thoi,U Minh,and Thoi Binh within Ca Mau province in the Mekong Delta of Vietnam.A list of 722 children and adolescents diagnosed with COVID-19 between June 2022 and February 2023 was provided,as recorded in the databases of Ca Mau Obstetrics and Pediatrics Hospital and Center for Disease Control (CDC) of Ca Mau province.Eligible participants met the following criteria: (1) Age between 6 and 16;participants must be older than six to ensure effective communication with their parents/guardians in the interviews;(2) no prior mental health disorder and any birth defects diagnosis recorded in their medical history;and (3) the time point of recovery from COVID-19 infection was at least three months until the interview time.As a result,a list of 422 individuals was identified for study participation.We surveyed all participants in the list (n=422)to optimize the statistical power without applying sample size calculation.Appointments for interviews were scheduled via phone a week in advance to ensure the availability of participants and their parents/guardians for the study.
2.3.Study instruments
The study used a structured questionnaire comprising two main sections.The first section aimed to gather socio-demographic data,including age (categorized as children for 6-9 years old and adolescents for 10-16 years old,classified by WHO[23]),sex(boy/girl),and participant’s residence (participants from Ca Mau city classified as ‘urban,’ while those from the five districts were categorized as ‘rural’).Additional data on height and weight were also collected.Body mass index (BMI) was calculated based on their sex using the formula of weight-to-height squared (kg/m2)ratio.Individuals were categorized as underweight,healthy weight,overweight,or obesity based on Centers for Disease Control and Prevention guidelines for BMI measurement in children and teenagers[24].Furthermore,data on the number of COVID-19 vaccination doses and the duration of COVID-19 treatment measured from the onset until the day of recovery was also collected.
The second section of the questionnaire consisted of 17 commonly reported symptoms associated with long COVID,identified through the WHO case definition of long COVID condition by a Delphi consensus[3],and previous systematic reviews and meta-analyses of long COVID in children and adolescents[8,13].These symptoms included the clinical manifestations affecting systems of respiratory(cough,shortness of breath),neurological (loss of taste and smell,ringing in the ears,headache,dizziness,impaired concentration,insomnia),dermatological (skin rashes,significant hair loss),muscular (joint pain,muscle pain),gastrointestinal (diarrhea),cardiovascular (chest tightness,palpitations) and general (fatigue,asthenia).Participants were asked "Yes/No" questions to determine if they had experienced these symptoms lasting at least two months after recovery for a minimum of three months of getting COVID-19 infections.Participants who indicated their experience of at least one symptom were categorized as having long COVID.
Three public health experts were invited for evaluation to check the questionnaire's validity.An average index of item-objective congruence score was obtained at 0.86,with none of the items scoring lower than the minimum acceptable value of 0.75[25].Cronbach's was used to evaluate the internal consistency of the questionnaire[26],with the value obtained at 0.83,more significant than 0.70,indicating acceptable reliability[27].
2.4.Data collection
A team of 10 commune health volunteers (CHVs) conducted the data collection.CHVs visited the participants' houses to perform the interviews,which lasted approximately 30 minutes.Data from respondents’ responses were recorded using a hard-copy questionnaire through direct interviews.Participants and their parents/guardians could consult the CHVs if they had any questions during the interview.During the interview,CHVs measured participants' weight and height using a digital weight scale and a portable height measure.
2.5.Statistical analyses
The descriptive analysis of the prevalence of each long COVID symptom was determined using percentage calculation (%) and standard deviation (SD) among participants.Since the participants may experience multiple symptoms,we utilized Phi correlation coefficients to assess the correlations among all pairs of binary variables representing long COVID symptoms.The Phi coefficient,ranging from -1 to 1,indicates the strength and direction of association between two variables.A negative value indicates a negative association,and a positive value implies a positive correlation,while the Phi coefficient of zero suggests no detectable association between two variables[28].Furthermore,the significance of the association between each pair of variables was determined using theChi-squared test.
Logistic regression was applied to investigate the risk factors associated with long COVID among COVID-19 participants.The outcome variable considered participants with any long COVID symptoms.The explanatory variables included (1) sex,(2) age group,(3) BMI category,(4) living residence,(5) duration of COVID-19 infection (days),defined from the day of COVID acquisition until testing negative,and (6) number of COVID-19 vaccination doses.Akaike's Information Criterion (AIC) determined the final multivariable models.Variables contributing to the lowest AIC values were selected,as decribed in previous study[29].The multivariable model,including variables withP<0.05,identified significant risk factors associated with long COVID.Interactions between explanatory variables were examined for potential confounding effects.
All statistical analyses were conducted using theRstatistical software.Packages "stats" and "ggplot2" were applied for building logistic regression models and data visualizations.
3.Results
3.1.Characteristics of study participants
Among the 422 children and adolescents who participated in the study,232 (55.0%) were boys,and 190 (45.0%) were girls.Most participants were within the 6-9 age range (considered children)(74.4%),while adolescents comprised the remaining 25.6%.Twothirds of the participants hailed from rural areas (67.9%).BMI scores were assessed,revealing that most participants had a healthy weight (55.5%),100 were classified as overweight (23.7%),56 were obese (13.3%),and 32 participants were categorized as underweight(7.6%).The majority of participants had not received any COVID-19 vaccination doses (77.5%),62 children received two doses (14.7%),and 33 participants received only one dose (7.8%).The duration of COVID-19 treatment from onset to complete recovery varied,with 240 participants re-testing negative from COVID-19 infection within a week (56.9%),157 recovering after one week (37.2%),and 25 taking more than two weeks to recover (5.9%) (Table 1).
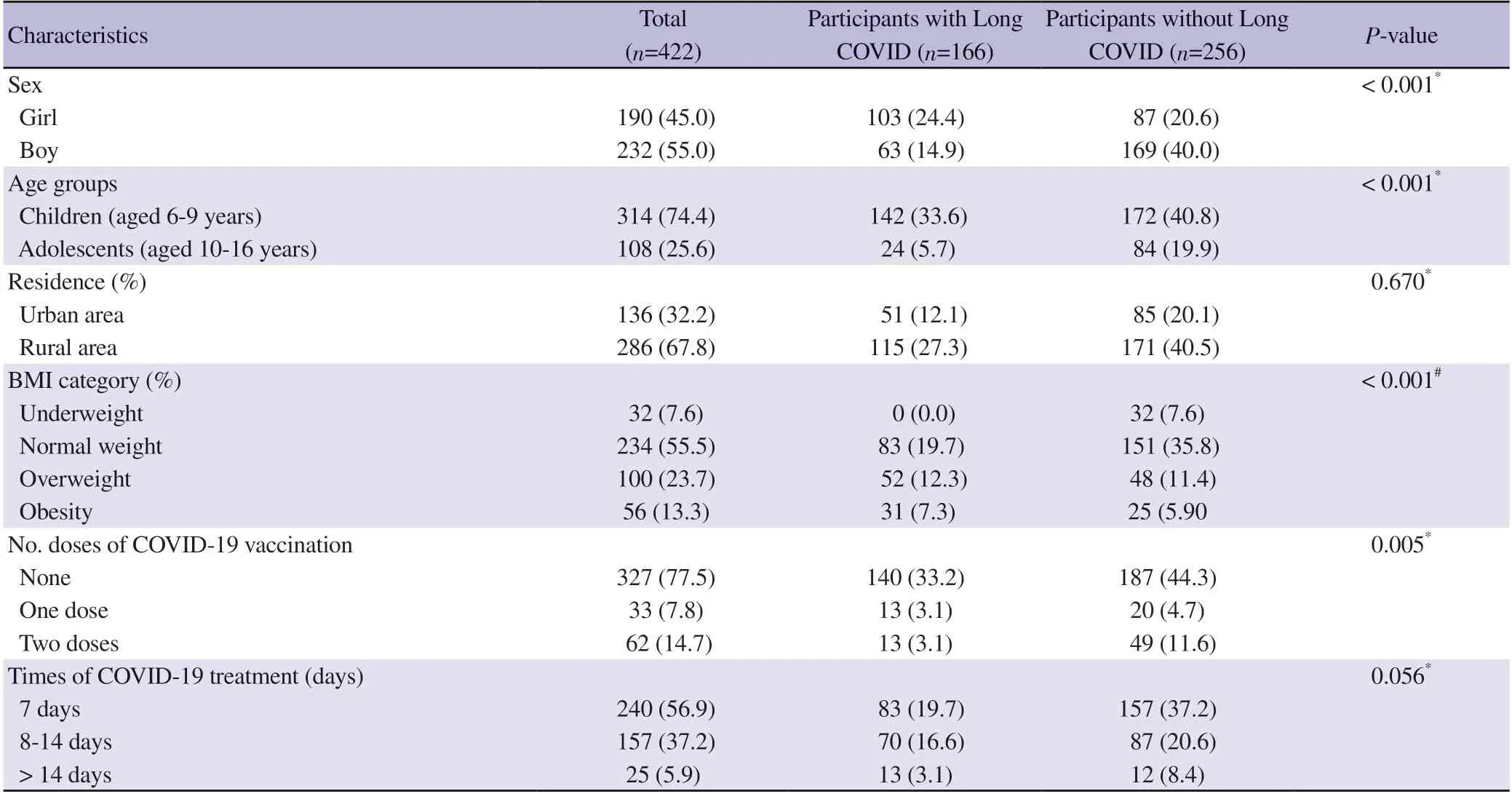
Table 1.Characteristics of study participants with and without long COVID [n (%)].
Of the total participants,166 (39.3%) reported experiencing long COVID,while 256 did not exhibit any prolonged COVID symptoms.Descriptive analyses revealed significant differences between long COVID conditions and participants’ sex (χ2test,P<0.001),age groups of children and adolescents (χ2test,P<0.001),BMI category(Fisher’s Exact test,P<0.001),and the number of COVID-19 vaccine doses administered (χ2test,P<0.005).No significant differences were found in participants with long COVID regarding their living residence (P=0.670) and the duration of COVID-19 treatment (P=0.056) (Table 1).
3.2.Prevalence of long COVID symptoms among participants
Seventeen symptoms characterized as long COVID conditions were surveyed among participants.One hundred sixty-six participants(39.3%) reported experiencing health issues regarding long COVID.Among these long COVID cases,36 (8.5%) reported suffering from a single symptom,48 (11.4%) reported two symptoms,52 (12.3%)reported three symptoms,27 (6.4%) reported four symptoms,and 3 (0.7%) reported five symptoms.Cough was the most common symptom 34.6% (SD=0.5),followed by fatigue 20.6% (SD=0.4),shortness of breath 10.9% (SD=0.3),lack of appetite 6.6% (SD=0.3),joint pain and muscle pain (both 4.3%) (SD=0.2),skin rashes 3.1% (SD=0.2),headache,impaired concentration,and insomnia(all 2.8%) (SD=0.2),ringing in the ears 1.7% (SD=0.1),dizziness and chest tightness (both 1.4%) (SD=0.1).Notably,loss of taste and smell,palpitations,significant hair loss and diarrhea were not reported by any participant.
In our study,314 participants were classified within the children's age range.Among them,142 participants reported experiencing at least one symptom of long COVID (45.2%,SD=0.5).The commonsymptoms were respiratory,with cough reported by 38.9% (SD=0.5) and shortness of breath by 14.6% (SD=0.4).Other prevalent symptoms included fatigue at 22.9% (SD=0.4) and lack of appetite at 8.9% (SD=0.3).In the adolescent group consisting of 108 participants,24 individuals (22.2%,SD=0.4) reported their clinical manifestations as long COVID.The reported symptoms were limited to five,including cough at 22.2% (SD=0.4),muscle pain at 16.7% (SD=0.4),fatigue at 13.9% (SD=0.3),joint pain at 11.1%(SD=0.2),and headache at 5.6% (SD=0.2).Figure 1 provides a detailed description of the prevalence of long COVID symptoms among study participants categorized into age groups of children and adolescents.

Figure 1.The prevalence of long COVID symptoms in children and adolescents.
3.3.The correlations of long COVID symptoms in children and adolescents
The most prevalent symptom,cough status,showed correlations with all other symptoms [Phi correlation coefficients (φ) ranged from 0.16 to 0.60,allP<0.002],except for symptoms,including loss of taste and smell,palpitations,diarrhea and significant hair loss that participants did not report.Another respiratory symptom,shortness of breath,was associated with lack of appetite,insomnia,impaired concentration,headache,and dizziness (allφ: 0.16-0.33,P<0.001).Fatigue also had correlations with most of reported symptoms (all φ: 0.18-0.60,P<0.017).Additional correlations were observed,including symptoms affecting neurological system such as dizziness with insomnia and impaired concentration (φ=0.70,φ=0.16,respectively) (bothP<0.001),and insomnia with headache and impaired concentration (φ=0.24,φ=0.49,respectively) (bothP<0.001).Furthermore,muscle and joint pain were strongly correlated(φ=0.65,P<0.001).The correlations among 17 long COVID symptoms reported by study participants are represented in Figure 2.

Figure 2.The correlation matrix of long COVID symptoms observed in children and adolescents.
3.4.Risk factors associated with long COVID symptoms in children and adolescents
In the univariable models,five variables associated with long COVID in children and adolescents were identified: sex,age group,BMI category,number of doses of COVID-19 vaccination,and the duration of COVID-19 treatment.These variables were selected for inclusion in the multivariable models.The findings from the multivariable model indicated that the girls had a 1.25 times higher risk of long COVID than the boys (P<0.001).The children group had a 1.24 times higher risk of long COVID than the adolescent group (P<0.001).Participants categorized as overweight had a 1.14 times higher risk of long COVID than those in the healthy weight group (P=0.018).Children or adolescents with no doses of COVID-19 vaccination and those with only a single dose had a risk 1.36 times and 1.35 times higher than those with two doses of vaccination (bothP<0.004).Furthermore,patients with a COVID-19 treatment duration longer than two weeks had a higher risk of long COVID 1.32 times than those who recovered within the first week after contracting COVID-19 (P=0.003).Details of the risk factors analysis for long COVID are described in Table 2.

Table 2.Risk factors associated with long COVID in children and adolescents.
4.Discussion
Our study conducted a retrospective cross-sectional investigation into long COVID symptoms among demographic groups of children and adolescents in community settings in both urban and rural areas within a southern province of Vietnam.The study revealed several key findings as follows: (1) a relatively high prevalence of long COVID conditions among study participants,with a higher prevalence of long COVID was observed in children than adolescents;(2) cough,fatigue,shortness of breath,and loss of appetite were frequently reported among surveyed participants;(3) significant positive correlations were observed among the common symptoms with almost all reported symptoms;and (4) risk factors associated with long COVID included various demographic groups,including those who were children (ref: adolescents),girls(ref: boys),overweight status (ref: healthy weight),no COVID-19 vaccination or receiving only one single dose (ref: two doses of COVID-19 vaccine),and the recovery duration from COVID-19 infections exceeding two weeks (ref: less than seven days).
The prevalence of long COVID-19 in children and young adults may vary due to heterogeneity in study designs,geographical locations,and sample sizes[30].Our study revealed a long COVID prevalence of 39.3% among children and adolescents.The finding aligns with a range reported in previous reviews,from 4.0% to 66.0%[31],and 1.6% to 70.0%[8].In agreement with these previous reviews,our findings identified respiratory,neurological,and sleep disorders and lack of appetite as prevalent symptoms of long COVID conditions among children and adolescents.We highlighted that cough,fatigue,shortness of breath,and loss of appetite were frequently reported symptoms among the surveyed participants.These observations were similar to the findings reported in a recent cross-sectional study conducted on hospitalized children in Vietnam,which demonstrated a high prevalence of cough (84%),fatigue(13.3%),and meal-skipping (12.0%) among participants[22].
Our study revealed that children are more susceptible to experiencing prolonged symptoms after recovering from the COVID-19 infection than adolescents.Findings from previous studies indicated a significant association between the prevalence of long COVID and the older age groups[12,15].The results from our study were different from these findings.However,a recent study indicated that symptoms related to cognitive and neurological disorders were linked to adolescents,while the younger age range exhibited respiratory problems[19].Our study found that most long COVID symptoms observed in participants were respiratory problems,particularly cough and shortness of breath.This is entirely consistent with our findings,with the most common long COVID symptoms being respiratory problems reported by most children rather than adolescents.Another possible explanation is that younger age groups have more parental needs and care than older ones[32].Clinical manifestations related to respiratory problems are more readily detected and recognized by parents than issues related to neurological and psychological disorders.Since our study was performed using interviews with children and adolescents with their parents,parental attention to their offspring may affect the varying prevalence of long COVID symptoms across different age groups.
Our study explored various factors associated with long COVID,including sex,BMI,the number of vaccination doses,and the time taken for COVID-19 infection recovery.These results aligned with prior research on long COVID in children and adolescents.Notably,girls exhibited a higher susceptibility to persistent symptoms than boys,with a 1.51 times according to Miller’s study[15],and a 2.7 times according to Berge’s study[2].Females typically exhibit more robust immune responses;however,this heightened activity may promote susceptibility to autoimmune diseases,contributing to chronic conditions associated with long COVID symptoms[33].Obesity has been identified as a potential risk factor for long COVID in the pediatric patients[17].Our univariable analysis initially indicated a significant association between obesity and long COVID.However,this significance was absent in the multivariable model,while overweight status remained significant.This change may be attributed to the small number of obese participants and the effect of other variables in the multivariable model,leading to non-significance.Nonetheless,weight gain poses a potential risk for long-term COVID-19.The COVID-19 pandemic has increased overweight and obesity rates due to reduced physical activity,heightened stress,and changes in dietary habits[34].Additionally,the cross-linking between gaining weight and chronic inflammation has been demonstrated[35],which may contribute to the manifestation of long COVID in overweight and obese participants.Furthermore,Bloiseet al.indicated that an extended duration of SARS-CoV-2 infection was also the risk factor for long COVID[17],highlighting the importance of infection duration in yielding prolonged symptoms among children and adolescents.The recovery period from COVID-19 infections depends upon the severity of the acute infection,and long COVID symptoms have been indicative of a correlation with the severity of acute COVID-19[36].Vaccination protects children and adolescents from the long-term consequences of SARS-CoV-2 infections.A recent prospective cohort study indicated a reduction in long COVID with at least one vaccine dose[37],supporting the protective role of vaccination.Our findings indicated that the higher the COVID vaccine doses,the higher the protection for children and adolescents against the persisting occurrence of long COVID.
Given the high variability of long COVID symptoms,with over 200 different manifestations affecting every organ system[38,39],the concurrence of these symptoms has been noted in individuals recovering from COVID-19.Our study observed the co-occurrence of multiple symptoms,with some participants experiencing up to five symptoms simultaneously.In a recent study,the number of long COVID symptoms reported was up to seven in the same patients,highlighting a significant association among long COVID symptoms including fatigue,shortness of breath,muscle pain,and mental health disorders[40,41].Since the correlations among long COVID symptoms are diverse,the specific combination and severity can vary among individuals.This poses a significant challenge in accurately diagnosing the long COVID condition.Therefore,further investigations into long COVID,especially in children and adolescents,are suggested to enhance research efforts to understand the patterns and variations in long COVID symptoms.
We acknowledge several limitations in our study.Our research was conducted in a community setting,but the data were retrieved from hospital and CDC databases.Our survey could not include all individuals who recovered from COVID-19 infections,especially those who experienced mild symptoms and opted for self-treatment.Furthermore,long COVID conditions were characterized by their persistence for at least two months after a 3-month recovery period.Considering the community-based nature of our study,the design relied on self-reported information obtained from children or their parents;the information bias might be unavoidable during data collection.Additionally,due to constraints in accessing the complete hospital database,we faced challenges obtaining sufficient data on symptoms at participants' hospital admission for a thorough comparison of the long COVID symptoms at the onset of COVID-19 infection and those occurring three months post-recovery.Besides,despite our study covering both urban and rural areas and finding no significant differences among participants experiencing long COVID,it is essential to consider that social contexts may vary,influencing study outcomes.The prevalence and factors associated with long COVID conditions in other regions may exhibit differences.Although our findings might apply to Ca Mau province,and could be extrapolated to the Mekong Delta region of Vietnam,further research is imperative to understand long COVID prevalence and associated factors among COVID-19 patients,encompassing children and adolescents,across other regions in Vietnam.
In conclusion,the impact of COVID-19 is still persistent,with post-COVID-19 conditions affecting individuals who have recovered from the infection,particularly among children and adolescents.Given the scarcity of research on long COVID in the pediatric population in Vietnam,our study revealed a relatively high prevalence of long COVID among children and adolescents in a southern province of Vietnam.Moreover,the findings of our study provide valuable insights into predicting the factors associated with the occurrence of long COVID in pediatric survivors.Therefore,strategic interventions are crucial and recommended to address and mitigate the risks of long COVID conditions among children and adolescents in Vietnam.
Conflicts of interest statement
All authors declare no conflict of interest.
Funding
The authors received no extramural funding for the study.
Authors' contributions
H.N.L,N.T.T,T.T.N,D.H.P conceived and designed the study.H.N.L,L.T.M.T,N.T.L,N.T.T.U conducted field survey,data collection.H.N.L,T.T.N,D.H.P contributed to data analyses.H.N.L,L.T.T.T,N.T.T.U,T.T.N,D.H.P contributed to writing up and editing the manuscript.All authors approved the summitted version of the manuscript.
Publisher’s note
The Publisher of theJournalremains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
杂志排行

Asian Pacific Journal of Tropical Medicine的其它文章
- Mitigating fire risks in hospitals: Are we primed and geared up?
- Navigating the future of malaria control: Insights from India's pioneering malaria slide bank
- Smoking of Carica papaya in Nigeria: The rationale,the public health effects and policies for intervention
- Dengue hemorrhagic fever with rectus sheath hematoma: A case report
- Characteristics of hospitalized patients with confirmed COVID-19 and their hospital management
- Epidemic management in a measles outbreak in 2023,the return of vaccinepreventable diseases: A single center,retrospective observational study